Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
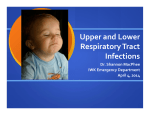
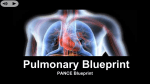
Pediatric Pulmonology 20:362-368 (1995) Oral Dexamethasone in the Treatment of Croup: 0.15 mglkg Versus 0.3 mglkg Versus 0.6 mglkg G.C. Geelhoed, FRACP, and W.B.G. Macdonald, FRACP Summary. The objective of this study was to compare the efficacy of a single dose of oral dexamethasone of varying sizes in 120 children hospitalized with croup in two sequential double 'blind, randomized, controlled clinical trials (Trials A and B). The study was conducted in the Emergency Department Observation Ward of a tertiary pediatric hospital. One hundred and twenty children (age range 6 to 160 months) hospitalized with croup participated. Baseline characteristics for the two groups in each trial were similar. In Trial A 60 children received either 0.6 or 0.3 mg/kg dexamethasone syrup; in Trial B 60 children received either 0.3 or 0.15 mg/ kg dexamethasone syrup. Duration of hospitalization, reduction in croup scores, and adrenaline usage were evaluated. Median duration of hospitalization was similar for children in Trial A (7 and 8 hr), and in Trial B (9 and 9 hr). Croup scores following treatment did not differ and were significantly lower than initial scores for all groups and in each trial. Other outcome measures were similar for the two groups in each trial, including need for nebulized adrenaline, numbers of patients admitted to intensive care, rate of return to medical care with reoccurrence of croup, and readmission to hospital with croup following discharge from hospital. We conclude that oral dexamethasone in a dose of 0.1 5 mg/kg is as effective as 0.3 or 0.6 mg/kg in relieving symptoms and results in a similar duration of hospitalization in children with croup. Pediatr Pulmonol. 1995; 20:362-368. 0 1995 Wiley-Liss, Inc. Key words: Croup, steroids, dexamethasone. no statistical differences in the efficacy of oral dexamethasone or nebulized budesonide with regard to hospitalizaCroup (acute laryngotracheobronchitis) is one of the tion time or croup scores, there was a consistent trend in more common childhood respiratory illnesses. Children favor of the oral preparation. Of the children who rewith moderate to severe airway obstruction are traditionmained hospitalized, children treated with oral dexamethally admitted to hospital for observation. Corticosteroids asone had a significantly lower mean pulse rate than the have been advocated as therapy in children hospitalised aerosol budesonide-treated group at 8 and 12 hr, and a with severe croup, however, studies in children with less lower respiratory rate at 8 hr, implying less work of severe illness have yielded conflicting result^.'^'^ In 1989, breathing. We did not specifically set out to answer this Kairys et al. published a meta-analysis of the nine methquestion, but it was our impression that oral medications odologically satisfactory studies conducted up to that (whether placebo or drug) were easier to administer to time. The results suggested that steroid therapy was assodistressed young children than nebulized treatment. Many ciated with faster clinical improvement in children hospisubjects found aerosol therapy distressing in its own right. talized with croup than placebo treatment, and that a Dexamethasone is also less expensive and requires no dose of greater than 0.3 m g k g dexamethasone was more facemask, tubing, or minimal time for delivery. Following effective than lower doses.13Five further studies examinour 1993 study the practice in our emergency department ing the use of inhaled and parenteral steroids in children is to use oral dexamethasone rather than inhaled budesonhospitalized with croup have been published since and ide for the above reasons. Although no side effects were all showed benefits from treatment.'1,'2.14-'6 Three of three studies have shown nebulized budesonide to be of benefit in ~ r o u p , ' ~and . ' ~the latter two studies found a reduction From the Emergency Department, Princess Margaret Hospital for Chilin duration of hospitalization. One of these studies" from dren, Perth, Western Australia. our emergency department performed in 1993 also demonstrated that budesonide and oral dexamethasone (0.6 Received December 8, 1994; (revision) accepted for publication July mglkg) were more effective than placebo, bringing about 8, 1995. reduced hospitalization time, reduction in croup scores Address correspondence and reprint requests to G . C. Geelhoed, Prinafter 1 hr, and reduced need for nebulized adrenaline after cess Margaret Hospital for Children, Box D184 GPO, Perth, W. A. 1 hr of therapy compard to placebo. Although there were 6001, Australia. INTRODUCTION 0 1995 Wiley-Liss, Inc. Dexamethasone in Croup TABLE 1-Croup Score Stridor None Only on crying, exertion At rest Severe (biphasic) Retractions None Only on crying, exertion At rest Severe (biphasic) 0 1 2 3 0 1 2 3 noted in this or other studies using a single dose of dexamethasone of 0.6 mgkg, we felt it logical to evaluate whether smaller doses would have similar beneficial effects in croup. This seemed especially important since the alternative treatment (nebulized budesonide) results in a much smaller dose of steroid being administered to each child with croup. This present study was conducted in two parts: Trial A, to test the relative efficacy of a single dose of 0.3 mg/ kg oral dexamethasone compared to 0.6 mgkg in children hospitalized with croup; and Trial B, to test the relative efficacy of a single dose of 0.15 mgkg oral dexamethasone compared to 0.3 m g k g in children hospitalized with croup. The second trial was undertaken as no difference could be demonstrated between 0.3 and 0.6 m g k g of dexamethasone. Our hypothesis was that smaller doses of a single oral dose of dexamethasone would be as effective as 0.6 mgkg in the treatment of croup. PATIENTS AND METHODS Children older than 3 months of age with no other acute or chronic medical problems were eligible for inclusion in the studies when they were admitted to Princess Margaret Hospital for Children with a diagnosis of croup, defined as the acute onset of inspiratory stridor, chest wall retractions, “barking” cough, and hoarse voice. Generally, only those children with croup who have stridor and chest wall retractions at rest are admitted to our hospital; milder cases are discharged home from the emergency department. Inclusion criteria included a minimum croup score of three (see Table 1). This was done to exclude children with mild disease who were admitted for other reasons such as living a long distance from medical care. Children were also excluded when their families did not have a telephone or had a limited command of the English language, whenever they had received steroid therapy of any description in the preceding week, had a preexisting upper airway condition, had a history of prolonged stridor, or presented with a clinical picture suggesting a diagnosis other than croup. In addition, children admitted directly to the ICU with severe croup were excluded. Informed, 363 written consent was obtained from parents. The study was approved by the hospital’s ethics committee. Following enrollment, the parents completed a questionnaire in regard to current and past episodes of croup. Croup score (see Table l), pulse rate, respiratory rate at presentation, and arterial oxygen saturation (SaOJ from a finger probe in room air using a Nellcor N-100 pulse oximeter (Nellcor Incorporated, Hayward, California) were recorded. Subjects were randomized to one of two groups in each trial. In Trial A, one group received oral dexamethasone BP (0.3 mgkg, maximum 6 mg), while the other group received oral dexamethasone BP (0.6 mg/ kg, maximum 12 mg). In Trial B, one group received oral dexamethasone BP (0.15 mgkg, maximum 3 mg) while the other group received oral dexamethasone BP (0.3 mgkg, maximum 6 mg). Treatments were administered in a double-blind fashion. Subsequent management was administered according to standard hospital practice. Due to lack of objective evidence to support its use, mist therapy has not been used in our institution for many years. Clinical observations were recorded hourly for the first 4 hr, and four hourly thereafter until 24 hr after entry into the study or until discharge. Nebulized adrenaline 1:100, 0.05 mLkg (maximum 1.5 mL made up to 5 mL total with normal saline) was administered if clinically indicated at any time during the trials. Inhaled adrenaline treatments were generally given for severe stridor and chest wall retractions equivalent to a croup score of five or six. If the attending doctors considered that croup was severe and that children failed to improve, patients could be withdrawn at any time to receive further steroids and be transferred to intensive care. If the child was withdrawn from the study, their study code was broken. Full observations continued for these children as results were analyzed by intention to treat at trial entry. Children were discharged home based on the clinical judgment of the medical staff. Our main criteria for discharge were no stridor or chest wall retractions at rest or a croup score of one or zero. No child was sent home within 4 hr of receiving nebulized adrenaline. Following discharge parents of the children were contacted by telephone 7 to 10 days later and asked whether their child had attended any medical care for recurrent croup symptoms or for other reasons related to their hospitalization, and whether they had been readmitted to a hospital with croup. The principal outcome measures were duration of hospitalization, reduction in croup scores, the proportion of each group remaining hospitalized at 24 hr, and use of nebulized adrenaline. Based on our 1993 study we compared use of adrenaline during the first hour following treatment and subsequently. The former study“ showed no difference in use of adrenaline in the first hour, but a significant reduction after I hr in those children treated with steroids compared to placebo. We also compared 364 Geelhoed and Macdonald TABLE 2-Baseline Characteristics of 120 Children Hospitalized With Croup’ B A Number Male/female Age (months) Duration of symptoms (hr) Temperature (“C) Pulse rate Respiratory rate Sa02 in room air Initial croup score Previous croup Viral/soasmodic2 0.3 m g k g 0.6 m g k g 0.15 m g k g 0.3 m g k g 29 18/11 35 (19) 18 (38) 38.0 (1.2) 146 (23) 31 (7) 97 (2) 3.8 12 15/6 31 25/6 42 (27) 25 (31) 37.8 (1.2) 144 (23) 33 (9) 96.9 (1.8) 3.7 29 2613 38 (34) 11 (17) 37.4 (0.9) 148 (29) 33 (9) 97 (1.7) 4.0 11 6/8 31 2 3 ~ 32 (23) 16 (19) 37.5 (1.0) 147 (27) 33 (8) 97.3 (1.3) 3.7 14 10/6 11 12/3 ‘No parameter was different for the two groups in each study with P 5 0.05. Numbers are mean (SD). 3 e e text for definition of “viral” and “spasmodic.” TABLE 3-Outcome Measures for 120 Children With Moderate Croup’ Trial group Median hospital stay (hr) Hospitalized at 24 hr Adrenaline in first hour ( y h ) Adrenaline after 1 hr (y/n) ICU (y/n) Represented with croup (y/n)’ Readmitted with croup (y/n)* Children withdrawn from trial A B 0.3 nigkg 0.6 m g k g 0.15 mgkg 0.3 mgkg 7 6.9% 21% 0% 0% 7% 3% 0% 8 6.5% 16% 3% 0% 10% 6% 3% 9 3.4% 45 % 0% 0% 3% 0% 0% 9 0% 19% 0% 0% 3% 2% 0% ‘No outcome measure was different for the two groups in each study with P 5 0.05. 2Eight children were not followed up. the number of children transferred to intensive care and the number requiring further medical care with recurrent croup following discharge. Kaplan-Meier survival analysis with log rank statistics was used to compare the two groups in terms of duration of hospitalization. The influence of the two treatments on the likelihood of continuing hospitalization and clinical improvement (croup score) was assessed by COX’proportional hazards regression. Mean croup scores at each observation time were compared, using Mann-Whitney U analysis for nonparametric, ordinal data, while the remaining normally distributed observations were compared using unpaired Student’s t tests. To demonstrate a difference of a doubling of the duration of hospitalization time at the 5 % level of significance with 80% power, a sample size of 33 was required. To demonstrate a significant difference of 20% in use of adrenaline after the first hour at the 5% level of significance with 80% power, a sample size of 37 was required. respectively, and 60 from each group were enrolled in each trial. The majority of children not enrolled were refusals by parents to take part in the study. A small number of failures to enroll was due to staff not attempting to enroll suitable subjects when the department was very busy. The children whose parents refused were not different to the study population in any of the parameters reported, including severity. The children’s age range was 6 to 160 months with 90% being younger than 6 years of age. Baseline characteristics for the two groups in each trial were similar (Table 2). Outcome measures were similar for both groups in each trial (Table 3). The median duration of hospitalization was similar for children in both groups in each trial (Fig. 1). Twenty four hours following entry into the study, there was no difference between the number of children in each group who remained hospitalized with only two children in each group remaining hospitalised in Trial A and only one child in Trial B. No difference was seen between the two groups in RESULTS either trial in regard to use of nebulized adrenaline either During the study periods for Trial A (July 10 to August in the first hour posttreatment or subsequently (Table 3). 17, 1994) and Trial B (August 22 to December 7, 1994), Of the 120 children in both trials only one child who 92 and 72 children with croup were admitted to hospital received 0.6 mgkg dexamethasone required nebulized Dexarnethasone in Croup A i % 2 365 B FN W l 40 i vOsm,ik,l II 0.3 mglkg 8 -n Q 60 UJ 0 40 c C 20 20 0 0 0 10 20 0 40 30 10 time (hrs) 20 40 30 time (hrs) Fig. 1. Kaplan-Meier plot of percent children hospitalized vs time. + 0.3 mg/kg 2 8fn '1 o ! 0 I I I i o ! I I I 1 2 4 6 8 0 2 4 6 8 time (hrs) time (hrs) Fig. 2. Croup score vs time for children hospitalized with croup. Croup scores for all four groups were less than their initial score by 1 hr ( P < 0.05). adrenaline after the first hour. She was discharged home at 7 hr with no subsequent problems (Table 3). There was no difference between the croup scores of the two groups in either trial at any time. Mean croup scores for the two groups in each trial were significantly lower at 1 hr after treatment than their initial score and continued to decline over the ensuing 3 hr ( P < 0.05) (Fig. 2). This improvement was maintained for up to 8 hr posttreatment. After this time comparisons became less meaningful as the numbers in each group had fallen dramatically. One child who received 0.6 m g k g dexamethasone was withdrawn from the trial by their attending physician in order to be given further steroids (Table 3). During the study period, none of the 164 children admitted to hospital with croup was transferred to intensive care. During the study period, children admitted with croup and not included in the trials received 0.6 mg/ kg dexamethasone during Trial A and 0.3 m g k g during Trial B. Fifty-seven of the families in Trial A and 55 of the families in Trial B were contacted following discharge from hospital. Nine children attended a medical facility subsequently for croup following discharge, and five children were readmitted to hospital; there was no significant difference between the two groups in each trial (Table 3). There was no difference between the pulse rate, respiratory rate, temperature, or SaOz in air of the two groups in either trial at presentation or for those who remained hospitalized for 24 hr following administration of dexamethasone. No child had an SaOz lower than 90% at any time. Although no attempt was made to categorize children as viral or episodic croup on entry into the trials, we recorded whether children had symptoms of fever and 366 Geelhoed and Macdonald rhinorrhea at home, had fever in hospital, the number of previous episodes of croup, the number of admissions to hospital with croup, and the duration of symptoms prior to presentation. We arbitrarily defined viral croup as having a temperature of greater than 38°C and/or fever and rhinorrhea at home and symptoms of 6 hr or more, and episodic spasmodic group as no history of fever and rhinorrhea at home, a temperature of less than 38°C while in hospital, duration of symptoms less than 4 hr, and at least one episode of croup in the past. Based on these definitions we were able to label 66 of the 120 children as either viral or spasmodic. There was no difference in the proportion of viral, spasmodic, or undefined children in either of the two groups in both trials (Table 2). There was no significant difference in the duration of hospitalization between the 43 “viral” children (1 1.5 hr) and the 23 “spasmodic” children (8.6 hr, P = 0.07). DISCUSSION These two trials have shown that treatment with small doses of oral dexamethasone (0.15 mgkg) resulted in no significant difference in the duration of hospitalization and resolution of symptoms in children admitted with croup than in a group reported by us when we used 0.6 mg/kg oral dexamethasone.I6 Because of the interplay between clinical and social factors when deciding to discharge a patient with croup, we felt that it was possible that a smaller dose of dexamethasone might have resulted in a similar hospitalization time, but possibly a less dramatic effect on symptoms in the first few hours after treatment. This would have resulted in higher croup scores and a greater need for adrenaline after the first hour in the 0.3 or 0.15 mgkg groups. This was not the case as all outcome measures were similar for all four groups, and we found little need for nebulized adrenaline after 1 hr of steroid treatment. In our previous study,I6 none of the 50 children who received steroids required nebulized adrenaline after 1 hr of steroid treatment compared with 20% of the 30 children in the placebo group. This decrease in the use of adrenaline was also found by Super et al.” In the two trials presented here, only one child out of 120 (0.8%) required adrenaline after the first hour. The use of adrenaline during the first hour after treatment with dexamethasone was not significantly different in either trial, although the greater percentage who required adrenaline in the 0.15 mg/kg group (45%) almost reached statistical significance ( P = 0.06; Table 3). This group also had the highest croup score at presentation (Fig. 1). As the 0.15 mgkg group received the most adrenaline, it might be argued that this contributed to their favorable outcome. As the effects of adrenaline are thought to last only a few h o ~ r s ” and ~ ’ ~ as the majority of adrenaline treatments were administered on entry into the trial in the first 5 to 10 min, it suggests that this group was more distressed and the greater use of adrenaline should be interpreted in that light and not as a failure of steroid therapy. The subsequent favorable course of this group supports this interpretation. Our 1993 studyL6demonstrated the ongoing need for adrenaline after 1 hr in those children treated initially with adrenaline and placebo only. As in our former study we have demonstrated the speed with which children improve following administration of oral steroids. This rapid lowering of the croup score along with the dramatic decline in the need for adrenaline emphasizes the very early relief of symptoms achieved by the use of steroids with consequent easing of patient, parental, and clinician anxiety. In the meta-analysis of Kairys et a1.,13 there appeared to be a dose-response effect of steroids in croup. The greatest clinical improvement was seen in studies in which the highest doses of steroids (greater than 0.3 mg/ kg dexamethasone) were u ~ e d . ~ . ’To - ’ ~the meta-analysis should be added the studies of Kuusela and Vesikari” and Super et a1.,I2both of which also used high doses of steroids and both of which showed a beneficial effect from drug treatment. The “low dose” studies in the metaanalysis, however, used an average dose of only 0.08 mg/ kg of de~amethasone.’.’~~~ These findings are compatible with the existence of a “plateau” effect where an improvement in outcome occurs with increasing doses up to somewhere between 0.08 and 0.15 mgkg dexamethasone with no further improvement achieved with greater doses. No placebo group was included in our present trials as we felt that the benefits of steroids in the treatment of croup have now been However, as no placebo group was used in these trials and the 120 children generally did so well, the question arises whether this result could be explained independent of the effects of steroids. A critic may be tempted to suggest that we only treated mildly affected children with more severe cases being missed or treated elsewhere. This does not appear to be the case, as we did require subjects to have symptoms at rest to be entered into the trials, and approximately 20% of the subjects had severe stridor and chest wall retractions requiring adrenaline when first seen. It is important to note that Princess Margaret Hospital for Children is the only tertiary childrens hospital for Western Australia with a population of approximately 1.6 million. The city of Perth is the most isolated city of its size in the world ensuring that all serious cases of croup in the state are referred to our emergency department, either directly or transferred from other hospitals if requiring intensive care. Historically our hospital admits between 300 to 500 cases of croup a year, with up to 10% of these children being admitted to intensive care prior to the routine use of steroids. During the study period none of the 164 children admitted to hospital with croup (either included or excluded from the trials) was transferred to intensive care and all had received dexamethasone. Dexamethasone in Croup We recognize that a clinical scoring system is not the ideal means of assessing response to a therapeutic intervention, but alternative means of doing so are not practical in this condition. Oxygen desaturation and the requirement for intubation are such rare events in children with croup that they are not realistic parameters by which to measure outcome, except perhaps in very large, multicenter studies. Clinical scoring systems are a well established means of evaluating therapeutic interventions in c r o ~ p . * The ~ ~ ~croup " score used in this study differs from that used in other studies in that we did not include measures for degree of restlessness or cyanosis. Both of these measures are difficult to standardize and are seen primarily in children with very severe croup, a group that was excluded from our study. A subjective assessment of cyanosis was not necessary in our study as all children were monitored at presentation and then at regular intervals with pulse oximetry. No patient in this study had a recorded SaOz below 90%. To ensure an acceptable level of interobserver agreement for our modified croup score, a score was blindly assigned prospectively by two workers to 15 randomly selected children with croup not in the trial. The weighted kappa statistic was 0.87, indicating acceptable interobserver agreement. The two trials, 0.3 vs 0.6 mgkg and 0.15 vs 0.3 mg/ kg, were conducted sequentially in the same department with the protocol varying only in the doses administered. To avoid randomization bias we have presented the results as separate trials. However as the baseline characteristics for the four groups in the two trials were similar (Table 2) and the same protocol was used for both trials, we subsequently combined the two 0.3 mgkg groups and compard the outcome of the resulting three groups, 0.15, 0.3, and 0.6 mgkg to achieve greater power to detect a more subtle difference in outcome. No difference was found. This was not surprising given the median duration of hospitalization for the two groups in Trial A were 7 and 8 hr, and identical in Trial B being 9 hr, thus making a type I1 error extremely unlikely. As in our 1993 study, we did not attempt to distinguish viral from spasmodic croup as it is often difficult in practice to make this distinction and definitions of viral and spasmodic croup vary. Studies have demonstrated improvement following steroid administration in both virail2 and spasmodic'0," croup, although other investigators have not distinguished between the two en ti tie^.^" Many children presenting in our studies had features to suggest both viral (e.g., fever and rhinorrhea) and spasmodic (e.g., recurrent episodes) features, and some workers argue that the two conditions lie at either extreme of a continuous s p e c t r ~ m .It' ~has been noted that the natural history of spasmodic croup with early resolution of symptoms would not allow time for steroids to help and could theoretically explain the early and similar outcome in our different groups if the majority had spasmodic croup. We 367 arbitrarily categorized children as viral or spasmodic to ensure that random selection of cases took place in the two trials. Almost half of the subjects could not be categorized, using our stated definitions and having features of both entities. However, more than half the children in each study, 72% in Trial A and 54% in Trial B, had a temperature of 38°C or more recorded in hospital or had a reported fever at home often with rhinorrhea which implies an infective process in the majority of children. Also, many children had a prolonged duration of symptoms prior to presentation (Table 2). These findings would be in keeping with the majority of studies in the metaanalysis and would argue against the notion that most children in our studies had spasmodic croup and would have recovererd quickly without steroid therapy. Finally, the outcome of the 120 children in these current trials including early decrease in croup scores, lack of need for adrenaline after 1 hr, and short duration of hospital stay is very similar to that of the 50 children who were treated with steroids in our 1993 study16 and is in sharp contrast to that of the 30 children in the placebo group. The protocol for both the 1993 study and the current trials differed only in the medications administered. In summary, we have demonstrated that using oral dexamethasone in a dose of 0.15 mgkg is as effective as 0.3 or 0.6 mgkg in children with croup with no significant difference in the duration of symptoms and hospitalization time. ACKNOWLEDGMENTS We thank Mr. David McKnight and the staff of Pharmacy for their help and support in the setting up of this study, and the staff of the Emergency Department for participating so enthusiastically. REFERENCES 1. Martensson B, Nilson G, Torbjar J. The effect of corticosteroids 2. 3. 4. 5. 6. 7. 8. in the treatment of pseudo-croup. Acta Otolaryngol (Stockh) 1960; 158(~~ppl):62-69. Novik A. Corticosteroid treatment of non-diphtheritic croup. Acta Otolaryngol (Stockh) 1960; 158(suppl):20-22. Eden A, Larkin VP. Corticosteroid treatment of croup. Pediatrics 1964; 33:768-769. Sussman S, Grossman M, Magoffin MD, Schieble J. Dexamethasone (16 alpha-methyl, 9 alpha-fluoroprednisolone) in obstructive respiratory tract infections in children. Pediatrics 1964; 34: 851-855. Skowron PN, Turner JAP, McNaughton GA. The use of corticosteroid (dexamethasone) in the treatment of acute laryngotracheitis. Can Med Assoc J. 1966; 94528-531. Eden A, Kaufman A, Yu R. Corticosteroid and croup. JAMA 1967; 200:403404. James JA. Dexamethasone in croup. Am J Dis Child. 1969; 11 7 51 1-5 16. Leipzig B, Oski FA, Cummings CW, Stockman JA, Swender P. 368 9. 10. 11. 12. 13. Geelhoed and Macdonald A prospective randomized study to determine the efficacy of steroids in the treatment of croup. J Pediatr. 1979; 94:194-196. Muhlendahl KE v, Kahn D, Spohr HL, Dressler F. Steroid treatment in pseudo-croup. Helv Paediatr Acta 1982; 37:43 1 4 3 6 . Koren G, Frand M, Barzilay Z , MacLeod SM. Corticosteroid treatment of laryngotracheitis v spasmodic croup in children. Am J Dis Child. 1983; 137:941-944. Kuusela A, Vesikari T. A randomised, double-blind, placebo-controlled trial of dexamethasone and racemic epinephrine in the treatment of croup. Acta Paediatr Scand. 1988; 77:99-104. Super DM, Cartelli NA, Brooks LJ, Lembo RM, Kumar ML. A prospective randomized double-blind study to evaluate the effect of dexamethasone in acute laryngotracheitis. J Pediatr. 1989; 1151323-329. Kairys SW, Olmstead EM, O’Connor GT. Steroid treatment of laryngotracheitis: a meta-anatysis of the evidence of randomized trials. Pediatrics 1989; 83:683-693. 14. Husby S, Agertoft L, Mortensen S, Pedersen S. Treatment of croup with nebulised steroid (budesonide): a double blind, placebo controlled study. Arch Dis Child. 1993; 68:352-355. 15. Klassen TP, Feldman ME, Watters LK, Sutcliffe T, Rowe PC. Nebulized budesonide for children with mild-to moderate croup. N Engl J Med. 1994; 331:285-289. 16. Geelhoed GC, Macdonald WGB. Oral and inhaled steroids in croup: A randomized, placebo-controlled trial. Pediatr Pulmonol. 20:355-361. 17. Westley CR, Cotton EK, Brooks JG. Nebulized racemic epinephrine by IPPB for the treatment of croup. Am J Dis Child. 1978; 132:484487. 18. Skolnik NS. Treatment of croup. A critical review. Am . I Dis Child. 1989; 143:1045-1049.