Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
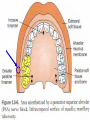
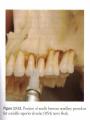
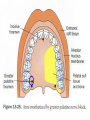
nerve block technique عمرو السويفي PROF. الطالب :مؤمن خالد محمود ابو حمره ID : 1002158 2013-2014 Maxilary nerve block Anatomy 3 Main Types of Maxillary Injections: 1) Local Infiltration 2) Field Block 3) Nerve Block Local Infiltration • Incision (treatment) is done in the same area in which the local anesthetic was deposited (interproximal papilla before Scaling and Root Planing) Field Block • Local anesthetic is deposited toward larger nerve terminal branches • Treatment is done away from the site of local anesthetic injection • Maxillary injections administered above the apex of the tooth to be treated are properly referred to as field blocks not local infiltrations Nerve Block • Local anesthetic is deposited close to a main nerve trunk, usually at a site removed from the area of treatment (PSA, IANB, NPB) Types of Injections 1) Supraperiosteal Injection 2) Intraligamentary (PDL) Injection 3) Intraseptal Injection 4) Intracrestal Injection 5) Intraosseous Injection 6) Posterior Superior Alveolar (PSA) Nerve Block 7) Middle Superior Alveolar (MSA) Nerve Block 8) Anterior Superior Alveolar (ASA) Nerve Block 9) Maxillary Nerve Block (2nd Division) 10) Greater Palatine Nerve Block 11) Nasopalatine Nerve Block 12) Anterior Middle Superior Alveolar (AMSA) Nerve Block 13) Palatal Approach Anterior Superior Alveolar (P-ASA) Nerve Block Maxillary and Mandibular Injections The following are used in both arches: • Supraperiosteal Injection • Intraligamentary (PDL) Injection • Intraseptal Injection • Intraosseous Injection Supraperiosteal Injection 1) Supraperiosteal Injection Used for pulpal anthesia in maxillary teeth Anesthetizes large terminal branches of the dental plexus Greater than 95% success rate 1 or 2 teeth Supraperiosteal Injection Dense bone covering the apices of the teeth can lead to failure -maxillary molar of children (zygomatic bone obscures) -central incisor of adults (nasal spine obscures) Negligible positive aspiration rate (less than 1%) Should not be used for large areas (multiple sticks/large amount of local anesthetic solution must be used) Technique Supraperiosteal Injection 1) 25 or 27 gauge short needle is recommended 2) Insert needle at height of mucobuccal fold over apex of desired tooth 3) Apply topical anesthetic for at least one minute 4) Orient bevel toward bone; lift lip pulling tissues taut 5) Hold syringe parallel to long axis of the tooth being anesthetized 6) No resistance to penetration should be felt and no patient discomfort 7) Aspirate twice 8) Deposit .6 ml (one-third of a cartridge) into tissue over 20 seconds 9) Do not allow tissues to balloon 10) Wait 3 to 5 minutes to begin dental treatment Problems/Failures If tooth does not anesthetize the needle tip could be below the apex of the tooth resulting in inadequate anesthesia If the needle lies too far from the bone then anesthesia will be inadequate because the solution was deposited in the soft tissue (lip) The needle must be oriented toward the periosteum but should be managed properly to avoid tearing the highly innervated periosteum Supraperiosteal vs. Infiltration These two words are used incorrectly; what most practitioners refer to as an infiltration injection is actually a field block Citing the ongoing economic crisis and growing competition from other insurers, Washington Dental Service will reduce reimbursement rates for all dental procedures by 15% starting June 1. Was it purely a business decision? Posterior Superior Alveolar Nerve Block (PSA) 2) Posterior Superior Alveolar Nerve Block Highly successful nerve block with greater than 95% success Effective for maxillary 1st, 2nd and 3rd molars and buccal periodontium Mesiobuccal root of the maxillary 1st molar is not consistently innervated by the PSA nerve Short dental needle is used for all but the largest of patients Average depth of soft tissue penetration is 16 mm (short needle is 20 mm in length) 28% of maxillary 1st molars’ mesiobuccal roots are innervated by the middle superior alveolar nerve (MSA) When the risk of hemorrhage is too great as with a hemophiliac, you should use the supraperiosteal or PDL injections Patient should feel no pain with this injection because bone is not contacted and there is a large area of soft tissue into which the solution is deposited Positive aspiration risk is 3.1% Patient will often say that they do not feel numb; reason why is because they are accustomed to the intense feeling of anesthesia experienced by the IANB; reassure patient that you are going to make sure they are comfortable during the procedure Technique PSA Nerve Block 1) 25 gauge short needle is recommended 2) Insert needle at the height of the mucobuccal fold above the maxillary 2nd molar 3) Target area is the PSA nerve which is posterior, superior and medial to the posterior border of the maxilla 4) Apply topical anesthetic for at least one minute 5) Have patient open their mouth half way which makes more room 6) Retract the patient’s cheek with mirror 7) Pull the tissues taut 8) Orient bevel toward bone 9) Insert needle at height of mucobuccal fold over the 2nd maxillary molar 10) Advance needle upward, inward and backward direction 11) Odd feeling of having no resistance whatsoever 12) Penetrating to an average depth of 10-14 mm is adequate 13) Aspirate in two planes by rotating bevel one quarter turn 14) Deposit 0.9 ml of a cartridge (1/2 cartridge) 15) Wait 3 to 5 minutes to start treatment Advance the needle in one movement, not three separate movements; usually atraumatic to most patients Problems/Failures (PSA) Hematoma formation if needle is overinserted too far posteriorly Pterygoid plexus of veins leads to this hematoma Visible intraoral hematoma develops within minutes; bleeds until the pressure of the extravascular blood equals that of the intravascular blood which can result in a large, unsightly hematoma Problems/Failures (PSA) Patients will usually claim that they do not feel any anesthesia which is not uncommon because patients can not reach this area to gauge their own level of anesthesia If using a long dental needle the maximum insertion should be one-half on its length or 16 mm Middle Superior Alveolar Nerve Block (MSA) 3) Middle Superior Alveolar Nerve Block Middle Superior Alveolar Nerve is not present in 28% of the population When the infraorbital nerve block fails to provide anesthesia to teeth distal to the maxillary canines, the MSA is indicated MSA provides anesthesia to 1st and 2nd premolars and mesiobuccal root of maxillary 1st molar; anesthetizes buccal periodontium and bone If MSA is absent the premolars and mesiobuccal root of maxillary 1st molar is innervated by the ASA Positive aspiration risk is less than 3% (negligible) Infraorbital nerve block can block 1st premolar, 2nd premolar and mesiobuccal root of the maxillary 1st molar if you need an alternative block when the MSA is not adequate Technique MSA Nerve Block 1) 25 or 27 gauge long or short needle 2) Insert needle at the height of the mucobuccal fold above 2nd maxillary premolar 3) Target is the maxillary bone above the apex of the 2nd maxillary premolar 4) Orient bevel toward bone to avoid tearing periosteum 5) Apply topical anesthetic for one minute 6) Pull tissues taut 7) Penetrate tissues placing bevel of needle well above the apex of the 2nd maxillary premolar Technique- Middle Superior Alveolar Nerve Block 8) Aspirate 9) Slowly deposit 0.9-1.2 ml of solution 10) Wait 3 to 5 minutes before starting treatment Problems/Failures MSA Anesthetic not deposited above the apex of the 2nd premolar Solution deposited into the soft tissue too far from the periosteum (lip) Hematoma may develop; Dentist should apply pressure to the area with gauze for at least sixty (60) seconds; up to 2 to 3 minutes Middle Superior Alveolar Nerve Block Anterior Superior Alveolar Nerve Block (ASA) Highly successful extremely safe block that causes hesitation in most clinicians Provides profound pulpal and soft tissue anesthesia from the maxillary central incisor distal to the premolars in 72% of patients Used in place of the supraperiosteal injection Uses less anesthetic solution than the supraperiosteal injection Supraperiosteal 3.0 ml solution ASA 1.0 ml solution #1 fear is damage to the patient’s eye which is unfounded Also known as the Infraorbital Nerve Block which is inaccurate Failed ASA is just a supraperiosteal injection over the 1st premolar Areas Anesthetized ASA Nerve Block 1) Pulp of the maxillary central incisor through the canine 2) 72% of patients have premolars and mesiobuccal root of 1st molar anesthetic 3) Buccal periodontium and bone of the above teeth 4) Lower eyelid, lateral aspects of the nose and upper lip When Do I Use This Block? 1) Dental procedures involving more than one tooth, i.e., central and lateral incisor 2) Inflammation/Infection precluding the use of the supraperiosteal injection 3) Ineffective supraperiosteal injections due to dense cortical bone Technique ASA Nerve Block 1) 25 gauge long needle is recommended 2) Insert needle at the height of the mucobuccal fold over the 1st premolar 3) Target: Infraorbital Foramen 4) Landmarks: Infraorbital Notch, Mucobuccal fold, Infraorbital Foramen 5) Apply topical anesthetic for at least one minute 6) Feel the infraorbital notch moving your finger down the notch palpating the tissues gently; the outward bulge is the lower border of the orbit which is the roof of the infraorbital foramen; continue the finger inferiorly until a depression is felt which is the infraorbital foramen 7) Maintain pressure over the foramen while inserting the needle down the long axis of the 1st premolar 8) Advance the needle slowly until bone is contacted gently which is the upper rim of the infraorbital foramen 9) 16 mm total advancement of needle;1/2 of long needle length 10) Estimate the distance between the infraorbital foramen and mucobuccal fold 11) Aspirate 12) Deposit 1.0 ml of anesthetic solution 13) Administrator can feel the anesthetic expanding the tissue with finger tip 14) Maintain finger pressure over the foramen for at least one minute to disperse the anesthetic solution 15) Needle should not be palpable in most patients 16) Wait 3 to 5 minutes for anesthesia to result Problems/Failures (ASA) Failure is from the needle deviating to the medial or lateral away from the infraorbital foramen Failure to reach the infraorbital foramen will result in anesthesia of the lateral side of the nose, upper lip and lower eyelid but not the teeth Hematoma formation can result although rarely; apply pressure to area for 2 to 3 minutes; at least 60 seconds Palatal Anesthesia Palatal Anesthesia Easily one of the most traumatic experiences for dentists due to the pain that is sometimes elicited from the patients Palatal injections can be administered atraumatically STEPS- Results in painless palatal injections 1) Apply topical for two minutes 2) Apply pressure to site both before and during deposition of the solution 3) Deposit solution slowly 5 PALATAL INJECTIONS 1) Anterior (Greater) Palatine Nerve Block: no pulpal anesthesia 2) Nasopalatine Nerve Block: no pulpal anesthesia 3) Local Infiltration: no pulpal anesthesia 4) P-AMSA: pulpal and soft tissue 5) P-ASA: pulpal and soft tissue Greater Palatine Nerve Block GP Nerve Block (soft tissue and bone only) Anesthetizes palatal soft tissue distal and medially to the canine (posterior portion of the palate) Tissues around the Greater Palatine Foramen are able to accommodate a larger volume of solution than the tissue in the vicinity of the Nasopalatine Foramen less patient discomfort Indications for palatal injections: 1) Scaling and root planing 2) Subgingival restorations 3) Deep placed matrix bands 4) Extractions (oral surgery) Technique Greater Palatine Nerve Block 1) 27 gauge short needle 2) Insert needle in soft tissue slightly anterior to the greater palatine foramen 3) Target is the greater palatine nerve as it passes from the foramen between the soft tissue and bone of the hard palate Locate the Greater Palatine Foramen: -use cotton swab/mirror handle -place a cotton swab at the junction of the maxillary alveolar process and the hard palate -press firmly into tissues moving posteriorly from the maxillary 1st molar -swab “falls” into the depression of the greater palatine foramen 4) Foramen is most often located distal to the 2nd maxillary molar 5) Apply considerable pressure to cotton swab in area of foramen until a noticeable ischemia occurs; hold pressure for 30 seconds before injection 6) Continue to apply pressure throughout the injection with the cotton swab 7) Slowly advance the needle until bone is gently contacted 8) Depth of penetration is usually less than 10 mm 9) Aspirate 10) Deposit solution very slowly Do not enter the greater palatine canal There is no reason to have the needle penetrate the canal There is no negative repercussion except post-operative pain Nasopalatine Nerve Block Nasopalatine Nerve Block (soft tissue and bone only) Considered by many to be the most traumatic, painful injection of all the dental injections Most important injection to follow the protocol about to be explained Anesthetizes the anterior portion of the hard palate (soft and hard tissues) from the mesial of the left premolar to the mesial of the right premolar Use this injection for the same reasons as Greater Palatine Nerve Block Target area is the incisive foramen beneath the incisive papilla Technique Nasopalatine Nerve Block 1) 27 gauge short needle is recommended 2) Insertion point: palatal mucosa just lateral to the incisive papilla 3) Approach the injection site at a 45 degree angle 4) Apply topical anesthetic for two minutes 5) Apply considerable pressure to the incisive papilla until ischemia 6) Continue to apply pressure to the cotton applicator tip while injecting 7) Advance the needle until bone is gently contacted 8) Depth of needle penetration is usually 5 mm 9) Slowly deposit ¼ cartridge over a 30 second interval 10) Wait 2-3 minutes for anesthesia Other Than P-ASA and Maxillary Nerve Blocks There is no reason to enter the Greater Palatine Foramen or the Nasopalatine Foramen when providing these injections do not advance needle more than 5 mm into the incisive canal because it could enter the floor of the nose causing infection Back Spray During palatal injections, the pressure generated within the syringe will cause the solution to spray into your mask/face; always wear the appropriate safety glasses and mask when giving any injection regardless of how trivial it may seem at the time nd 2 Example of Nasopalatine Injection Technique 2nd Example of Nasopalatine Injection Insertion Points: 1) Labial frenum; midline of maxilla (0.3 ml over 15 seconds) 2) Interdental papilla of #8 and #9 (0.3 ml over 15 seconds) 3) Palatal soft tissues lateral to the incisal papilla (contact bone) 2nd Example of Nasopalatine Injection Important Points: • Topical and pressure anesthesia on the palate are not necessary because the first injection anesthetized the palatal tissues • Contact bone on the 3rd injection (incisive papilla) only • Interdental papilla between maxillary central incisors is sore for a few days • Greater palatine nerve may overlap and lead to inadequate anesthesia of the canine and 1st premolar P-ASA P-ASA Palatal Approach Anterior Superior Alveolar Nerve Block • Described in the 1990s by the inventors of the CCLAD systems • Comparative to the Nasopalatine Nerve Block • Insertion: lateral point of the incisive papilla but the big difference: NEEDLE TIP IS POSITIONED IN THE INCISIVE CANAL • Deposit 1.4 – 1.8 ml of solution at 0.5 ml per minute • Primary method of achieving bilateral pulpal anesthesia of the maxillary anterior six teeth; anterior palatal 1/3rd • Provides profound soft tissue anesthesia of the gingiva and mucoperiosteum • Soft tissue of the facial attached gingiva is achieved anterior to the maxillary anterior six teeth • P-ASA is the 1st injection to produce bilateral pulpal anesthesia of the maxillary anterior six teeth from a single injection MAIN POINT OF THIS INJECTION: P-ASA is designed to provide pulpal anesthesia of the maxillary anterior six teeth in addition to the facial gingival soft tissue and mucoperiosteum it does not anesthetize the lip as with the regular mucobuccal fold approach; esthetic Dentistry can then be assessed without dealing with lip anesthesia when smiling • Palatal approach allows anesthesia to be limited to the subneural plexus for the maxillary anterior teeth and nasopalatine nerve • Minimum volume for injection is 1.8 ml (full cartridge) over 0.5 ml/minute • Insert needle very slowly • 4% anesthetics should have volume reduced by ½ (Prilocaine/Articaine) • Do not use 1:50,000 epinephrine • May need supplemental mucobuccal fold injections for canines because of their very long roots • Palatal ulcers develop from ischemia 1-2 days after treatment and are selflimiting; healing occurs in 5-10 days Technique P-ASA 1) 27 gauge short needle is recommended 2) Insert needle just lateral to the incisive papilla in the papillary groove 3) Target is the nasopalatine foramen 4) Needle held at 45 degree angle to the palate (same as central incisors) 5) Insert needle 6 to 10 mm; if resistance is found do not force needle 6) Insert needle 1-2 mm every 4-6 seconds while administering solution 7) Resistance means you have to reinsert the needle; careful of nose floor 8) Aspirate 9) Deposit 1.8 ml of anesthetic solution very slowly 0.5 ml/minute 10) Patient may feel “needle shock” very disturbing to patient Maxillary Nerve Block 1) Greater Palatine Approach 2) High Tuberosity Approach Maxillary Nerve Block Facts Also known as a nd 2 Division block Anesthetizes the maxillary division of the trigeminal nerve Areas Anesthetized: 1) Pulpal anesthesia of all teeth on the side of injection (ipsalateral) 2) Buccal periodontium and bone on the side of injection 3) Soft tissues and bone of the hard palate/soft palate medial to midline 4) Skin of lower eyelid, side of the nose, cheek and upper lip Maxillary Nerve Block Approaches It would require 4 other injections to get the effect of the Maxillary Nerve Block i.e., PSA, Infraorbital, Greater Palatine and Nasopalatine 2 Approaches: 1) Greater Palatine Approach 2) High Tuberosity Approach 1) Greater Palatine Approach Technique 25 gauge long needle recommended Insert into palatal soft tissue over greater palatine foramen Target is the maxillary nerve as it passes through the Pterygo-palatine Fossa; the needle passes through the Greater Palatine Canal to reach the Pterygopalatine Fossa Find the foramen by using a cotton swab until it “falls into” the foramen Most often found at distal of the maxillary 2nd molar Topical anesthetic for at least two minutes Inject into the area adjacent to the Greater Palatine Foramen in order to block the nerve before probing into the actual foramen itself 1) Greater Palatine Approach Technique Remember to apply constant pressure into this area until the tissue blanches which will lessen the discomfort of the needle penetration Probe gently for the foramen with the needle tip at a 45 degree angle After finding the canal advance the needle 30 mm 5 to 15% of foramens have boney obstructions, so if you encounter an obstruction do not force the needle, try again then abort Maxillary Nerve Block 2nd Approach 2) High Tuberosity Approach 25 gauge long needle recommended Insert to the height of the mucobuccal fold distal to the 2nd molar Target is maxillary nerve as it passes through the pterygopalatine fossa Superior and medial to the target site of the PSA Again, advance the needle to a depth of 30 mm Upward, inward and backward direction same as PSA Resistance should not be felt, if it is, the angulation is too medial At 30 mm the needle tip should lie within the pterygopalatine fossa Aspirate several times and inject 1.8 ml (one cartridge) slowly Maxillary Nerve Block 2nd Approach 2) High Tuberosity Approach Complications Hematoma develops rapidly if the maxillary artery is punctured with the needle tip Thin, porous substance of the maxillary bone allows for rapid diffusion of solutions into the cancellous bone Most Dentists rely solely on the supraperiosteal injection to provide anesthesia in the maxilla PSA and ASA combined can deliver safe anesthesia to virtually all patients requiring maxillary anesthesia Universal: -applying topical anesthetic for one minute -proper patient positioning -aspiration -making the needle safe after each injection with the scoop technique Long Buccal Nerve Block Anterior branch of Mandibular nerve (V3) Provides buccal soft tissue anesthesia adjacent to mandibular molars Not required for most restorative procedures Buccal Nerve Block Indications Anesthesia required - mucoperiosteum buccal to mandibular molars Contraindications Infection/inflammation at injection site Buccal Nerve Block Advantages Technically easy High success rate Disadvantages Discomfort Buccal Nerve Block Alternatives Buccal infiltration Gow-Gates PDL Intraseptal Buccal Nerve Block Technique Apply topical Insertion distil and buccal to last molar Target - Long Buccal nerve as it passes anterior border of ramus Insert approx. 2 mm, aspirate Inject 0.3 ml of solution, slowly Buccal Nerve Block Landmarks Mandibular molars Mucobuccal fold Buccal Nerve Block Complications Hematoma (unusual) Positive aspiration 0.7 % Mental Nerve Block Terminal branch of IAN as it exits mental foramen Provides sensory innervation to buccal soft tissue anterior to mental foramen, lip and chin Mental Nerve Block Indication Need for anesthesia in innervated area Contraindication Infection/inflammation at injection site Mental Nerve Block Advantages Easy, high success rate Usually atraumatic Disadvantage Hematoma Mental Nerve Block Alternatives Local infiltration PDL Intraseptal Inferior alveolar nerve block Gow Gates Mental Nerve Block Complications Few Hematoma Positive aspiration 5.7 % Incisive Nerve Block Terminal branch of IAN Originates in mental foramen and proceeds anteriorly Good for bilateral anterior anesthesia Not effective for anterior lingual anesthesia Incisive Nerve Block Nerves anesthetized Incisive Mental Incisive Nerve Block Areas Anesthetized Mandibular labial mucous membranes Lower lip / skin of chin Incisor, cuspid and bicuspid teeth Incisive Nerve Block Indication Anesthesia of pulp or tissue required anterior to mental foramen Contraindication Infection/inflammation at injection site Incisive Nerve Block Advantages High success rate Pulpal anesthesia w/o lingual anesthesia Disadvantages Lack of lingual or midline anesthesia Incisive Nerve Block Complications Hematoma Positive aspiration 5.7 %