Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
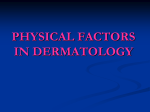
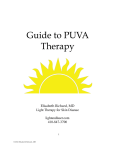
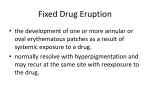
Adverse Events in Phototherapy Kathryn Thomson • Phototherapy involves exposure of the skin to ultraviolet light with or without the use of a phototoxic drug • Ultraviolet light is known to cause DNA damage and predispose to skin cancer • Phototherapy also has a number of other potential side-effects that need to be considered before starting treatment • It is essential to know about these in order to advise patients appropriately, prevent where possible and treat if not Adverse Events • Short Term/ Acute Events • Long Term / Chronic risks • Potential adverse events vary according to type of phototherapy used, extent of treatment (local/ whole body),previous treatments, patient specific factors • Differences between PUVA and UVB Adverse Effects of PUVA Four main variables; The Psoralen (drug choice and mode of delivery) The ultraviolet radiation The patient (skin type/ photosensitivity/ patient size) The equipment Adverse Events related to Psoralen • • • • • • • • Nausea: common with 8MOP, rarer with 5MOP Headache, dizziness, sweating, general malaise Itch- more common with 8MOP Rarer side-effects include rashes, asthma, deranged LFTs Exacerbation of cold sores Drug interactions Exacerbation of photosensitivity eg PLE PUVA blisters (lesional and perilesional) Contraindications to oral PUVA • • • • • • Pregnancy Severe Liver or renal disease Immunosuppressant agents Previous skin cancers Previous severe adverse reaction to psoralen Patients where compliance with eye protection cannot be ensured Drug History Medications may interact with psoralen or cause photosensitivity or phototoxicity • Coumarin anticoagulants eg warfarin . Manufacturers recommend that they are not used together • Tolbutamide causes increased photosensitivity • Anticonvulsants can reduce psoralen levels Psoralen Pharmacology • A light meal increases bioavailability of 8MOP by up to 50%, heavy meals decrease peak concentration and increase time taken to reach peak • Psoralen binding in tissues is shortlived- 24 hours after taking minimal psoralen detected in skin and organs • psoralen is rapidly metabolised in liver, but once the enzymes are saturated psoralen is allowed to accumulate. Over the threshold small increases in dose result in larger increases in plasma levels ie dose increase of 10-40mg results in 25 x one hour plasma level How to Manage Psoralen Induced Events Nausea: 1) take psoralen with food (light low fat meal as high fat diets reduce psoralen absorption) or 2) Prescription anti-emetics 3) switching to 5MOP which is absorbed more slowly and has a lower peak plasma level PUVA Itch 1)Emollients 2)Antihistamines 3) Switch to 5MOP 4)Switch to bath PUVA (can still occur but is less common) 5) Consider TLO1 or other treatments if persistent Can be painful- PUVA pain Ultraviolet triggered events Cold sores 1) Ask about history before treatment 2) Consider visor / sunblock to protect the affected site PLE Consider changing to TLO1 with lower dose regime. Acute Ultraviolet Reactions • • • • • Sunburn like erythema Redness, oedema and potential blistering Oral PUVA peak: 2-3 days Bath peak: 3-5 days More common in normally covered protuberant areas • Can be graded on basis of severity (see later) • Localised burning in bath PUVA Chronic Adverse Effects of PUVA • Skin aging- epidermal thinning, wrinkling, loss of elasticity, leathery texture, elastotic degeneration, uneven pigmentation (hyper and hypo), PUVA keratoses • Eyes- cataracts (eye protection for oral PUVA for 24 hours) • Non-melanoma skin cancer: steep dose response curve seen, highest risk at male genital skin: risk increased if on immunosuppression, type I and II skin, previous skin cancer, keratoses, previous radiotherapy Adverse Events in UVB Acute • Erythema and sunburn-like reaction (more common than with PUVA). Reactions are maximal at 24-36 hours • Transient erythema- starts a few minutes after UV exposure and persists for up to 8 hours. Not visible by next appointment • Itch: less common than with PUVA • Cold sores: as with PUVA • Eyes: keratitis and conjunctivitis (eyes feel gritty) • Facial pigmentation (particularly with pregnancy/ hormones) • Facial dermatitis- mild seen in around 5% patients Chronic Effects of UVB • Premature ageing- less than with UVA • Non melanoma skin cancer: risk is probably lower than with PUVA, although not fully established Clinical Assessment of Erythema (taken from Cardiff phototherapy manual 2010) E0: no erythema E0+: patient reported initial erythema but settled by attendance E1: barely perceptible asymptomatic erythema E2: well defined erythema, with mild discomfort E3: symptomatic painful well defined erythema E4: painful erythema with blisters Erythema Grading E1 E2 E3/4 Erythema Protocols ADVERSE EFFECTS a) Grade 1 erythema (mild) - barely perceptible erythema repeat previous dose consider reduction to 10% increments b) Grade 2 erythema (moderate) - well defined symptomatic erythema postpone until settled then give penultimate dose at next visit and thereafter reduce to 10% increments c) Grade 3/4 erythema (severe) - symptomatic erythema and/or bullae. No treatment and reviewed by a doctor on call. When settled treat at 50% of previous dose Risks of Carcinogenesis • Risks of skin cancer are hard to quantify • Increased risk with immunosuppressants, fair skins (red hair and freckling), high levels of sun exposure • Risk thought to be significantly higher after 200 exposures of PUVA and 500 exposures of TLO1 (some centres use 300) • Annual skin surveys are recommended for patients with high treatment levels and other risk factors Reducing Risk • Optimum phototherapy regime achieves complete clearance with minimum exposure numbers, low cumulative dose and fewest possible side effects Reducing Acute Adverse Events • Careful assessment of patients considering all absolute and relative contraindications • Written information sheets • Clear information about good practice in the cabinet • Advice about topical applications/ cosmetics/ deodorants • Avoid hair cuts • MED/ MPD pre treatment • Accurate and careful record keeping to ensure correct dosing • Adverse incident recording • Audit Reducing Long Term Risks • Cover areas not needing treatment (genital and ocular protection, visors) • Minimise use in patients with high treatment numbers • Use adjuvant therapies where possible to reduce exposure numbers • Ensure phototherapy used appropriately (ie not just to avoid topical treatments) • Annual screening for patients with high cumulative treatment numbers Reducing Risks (continued) • Regular discussion about adverse events to look for trends • Audit