Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
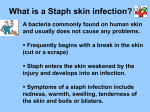
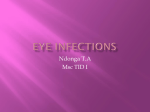
Microbiology 09/19/2008 Gram-Positive Cocci Transcriber: Sonia Nkashama 00:00-35:50 The audio didn’t start until the middle of slide 4. 4. Also ubiquitous in the human population is S. epidermidis and several others in this group. They are always present on the skin; everyone has this Staphylococcus. Usually it does not cause any problems. But if you get an IV put into your arm for some reason (to give fluids or medications, etc), this organism has a special ability to attach to plastic IV catheters. So it has a tendency to cause bloodstream infections, once you have allowed it to get into the bloodstream by entering with a foreign body. It’s not usually so virulent that it can go through intact skin to get into the bloodstream. But if you put an IV catheter in a vein and allow the organism to get there, it can certainly cause problems. Staphylococcus saprophyticus is an organism that actually causes urinary tract infections in young women. It’s actually found in the urinary tract and can cause infections there. 5. As far as some of the microbiological characteristics of the Staphylococci, there’s one thing that they all have in common: they stain as round, Gram-positive organisms. They will usually appear in grape-like clusters; this is a typical Gram stain. You can look at this Gram stain, and by the fact that it is dark-purple staining, round cells that appear in bunches, it is most likely a Staphylococcal organism. You can’t say which Staphylococcus that it is, however. They are usually a micrometer in size, and they occur in clusters. They are very easy to grow in a clinical lab. They’ll grow on most of the media that we have; they’ll grow under aerobic conditions. S. aureus is β-hemolytic. We will say more about hemolysis when we talk about the Streptococcus. And you will actually get to see hemolytic patterns in the laboratory. The Staphylococcus produces several exotoxins, and one of the toxins it produces is a hemolysin. This allows it to hemolyse red blood cells. If you grow the organisms on a blood agar plate (usually a sheep blood agar plate—standard media that is used in Micro lab), you’ll see a clearing around the organisms. This is a complete hemolysis, a complete lysis of the cell. This is referred to as β-hemolysis. Something else that you can use to identify S. aureus is that it will ferment mannitol. If you put the Staphylococcus on a plate that contains mannitol as a carbohydrate substrate, it will ferment the mannitol. And in doing so, it will cause a pH change. The pH indicator in the medium, such as phenol red, will cause the agar plate to turn from red to yellow, thus indicating mannitol fermentation. Two other important characteristics that help you identify S. aureus are the catalase and the coagulase test. You will do those in the lab next week. The catalase test is actually a test for the presence of hydrogen peroxide, and it will separate the Staph’s from the Strep’s. The coagulase test is another test that will separate S. aureus from some of the others. These are very important tests that you need to understand the biochemical basis of. 6. This is the reaction that you see in the catalase test and how you do it. You take hydrogen peroxide, and if you have the catalase enzyme in the Staphylococcus, it will produce water and oxygen, and you will see bubbles. And the way that you do the test is you just add hydrogen peroxide to a colony of the organisms that you are looking for, and you see if you get bubbles. So this is an easy way to distinguish the Staphylococcal organisms from the Streptococcal organisms. The Strep will be catalase-negative, while the Staph will be catalase-positive. So why would a bacterium want to produce catalase? It’s a virulence factor. Peroxides are toxic to many bacteria. We produce peroxides in our body as part of our innate host immune defense system. Peroxides will break down bacteria. If the bacteria can get ahead of the game and break down the peroxide, the peroxide can’t do anything to the bacteria. So it indeed is a virulence factor that many bacteria possess; Staphylococcus is among those bacteria that do possess this trait. Microbiology: Gram-Positive Cocci Sonia Nkashama pg. 2 7. The other reaction that I mentioned is the coagulase reaction. Coagulase is an enzyme that actually converts fibrinogen to fibrin. It will produce a clot around the Staph. And the advantage to this is that in the body, the organism that is producing coagulase will clot plasma around itself. Therefore it will protect itself from complement, antibodies, WBCs, etc. that the body is producing to try and get rid of it. So this is way that it has of protecting itself and avoiding the host immune system. This happens to be a very useful test because it will distinguish S. aureus and the relatively few other staph’s that are coagulase-positive from a large group of staph which are coagulase-negative. This group includes S. epidermidis and many others that are not as important as pathogens. Coagulase again is a virulence factor, and it’s one that we use in the lab all the time to help identify S. aureus and distinguish it from the other Staphylococci. The classic way that you do the test is the free coagulase test. You take rabbit plasma, put the Staph in the rabbit plasma, and it will clot if it produces coagulase. If the plasma doesn’t clot, then it’s a coagulasenegative Staph. This may take a few hours to produce the reaction, so it’s not as efficient. One of the ways that we do it is to look for clumping factor, which is a surface coagulase test. We just have latex particles that have the fibrinogen and IgG coated on the surface of the particle. The IgG is to protect protein A (another virulence factor). This is a way that you can test it quickly. You can just look quickly to see if there is agglutination of the Staphylococci with the latex particles. And that is presumptive identification of the bound coagulase that is present on the surface of the Staph. So you can get that info very quickly. This will be clearer when you do the test in lab. So remember catalase separates Staph and Strep; coagulase will distinguish S. aureus from the other coagulase-negative Staphylococci. 8-9. The staphylococci have a number of different surface structures that also enable it to be a pathogen. And of course, like most Gram-positive bacteria, it has a large layer of peptidoglycan. It also has teichoic acids & protein A (another surface antigen). This protein is also a virulence factor because it allows the bacteria to bind antibody. It will bind the Fc fragment of IgG and inactivate it. By doing this, it helps protect the Staph from the antibody that the host is producing. Clumping factor is the bound coagulase that I mentioned before. In other words, Staph actually has a surface molecule on it that is the clumping factor expressed, as well as an enzyme that it actually secretes into the environment. Some staphylococci actually have a capsule, a polysaccharide slime layer. This is an antiphagocytic action, helping evade it from the host immune system. And in the case of S. epidermidis, it also has this layer, which is part of what allows it to get through plastic, etc. The peptidoglycan, a big part of the Staphylococcal cell wall, is also a virulence factor because it will stimulate the host to produce interleukins, inflammatory mediators, as well as opsonic antibodies that will help to bind the Staphylococcus. It’s also one of the things that stimulates neutrophils. Remember that the prototype lesion of Staphylococcal infection is an abscess. S. aureus is one of the most common causes of abscesses anywhere in the body. Part of the reason that you get an abscess is that things that are on the organism are stimulating the WBCs (mainly the PMNs) to come to the place where the Staph is invading the body. Phagocytosis is a very important defense mechanism against this organism because it’s an extracellular organism that gets engulfed by the neutrophil and it will die. Question: How is the peptidoglycan a virulence factor? It’s a virulence factor in that it stimulates the host immune response. And in stimulating the host immune response, it’s causing damage. Remember part of the thing that we are doing in trying to kill the bacteria, we are producing a lesion. An abscess is disease caused by Staph. That’s a pathologic lesion. The reason that the Staph produces the lesion, to a large degree, is that the peptidoglycan stimulates PMNs to come. So it’s a virulence factor in that it’s allowing the Staph to produce disease to produce an abscess. Microbiology: Gram-Positive Cocci Sonia Nkashama pg. 3 It’s also involved in the binding of the bacteria to the tissue. One of the important things that bacteria have to do to cause disease in the body is to attach themselves somewhere. If they are going to produce toxins and cause tissue damage, they have to get into close approximation with the body. So the fibronectin component in the host cells actually is a target of the cell wall peptidoglycan. This is one of the things that actually allows the Staph to attach so that it can then produce its toxin and local damage there. I already mentioned Protein A as binding antibody. And of course, I mentioned the capsule as well. 10. In addition to the cell surface structures that are virulence factors in the Staph, it produces a lot of soluble virulence factors. These are exotoxins, usually enzymes or substances that the Staph produces and secretes around itself. They can actually travel to other parts of the body and cause disease. This is one of the reasons that S. aureus is such a successful pathogen; it has so many different ways that it can cause disease and so many different diseases that it can cause. For example, we talked about the catalase & the coagulase. An enzyme, hyaluronidase, elaborated by the Staph will actually destroy connective tissue. You learned in Microanatomy last year about the fascia and the tissue and what holds the tissues together. Well, hyaluronic acid is one of the things that binds your tissue together. One of the things that the Staph does is produce an enzyme called hyaluronidase; this allows it to spread in the tissues by breaking down the glue that holds your tissues together. This allows it to spread through fascial planes and the cause of disease is spread this way. S. aureus is resistant to many antibiotics. One example is a β-lactamase that it produces. The β-lactams includes all of the penicillin and cephalosporin antibiotics (some of the most common antibiotics that we use to treat infections). When penicillin was first introduced in the 1940s, all staphylococci were susceptible to it. Within a very short time, most staphylococcus became resistant to penicillin. This is because it will produce an enzyme that breaks down the β-lactam ring and destroys the penicillin. β-lactams work because they have this βlactam ring in their structure that resembles the amino acids that are used to link the peptidoglycans together. And by breaking down and opening the β-lactam ring, the penicillin molecule will no longer resemble the substrate to cross-link the cell wall binding. And that’s why penicillins don’t work on S. aureus. Several other enzymes are also produced by the Staph aid it in producing human disease. I won’t go into detail about all of them; I just mention what they are on this slide. 11. In addition to some of these, you also have cytotoxins and leukocidins. One particular substance called the Panton-Valentine leukocidin is an enzyme that allows the Staph to lyse WBCs. Remember all of these virulence factors not only are the things that allow the Staph to produce lesions, but they’re also the things that allow it to damage the host immune system so that they can survive. WBCs are very important in getting rid of Staph. So if you can kill the WBCs before they kill you, this is an example of what successful bacteria can do. This is a particularly important virulence factor in the new strains referred to as community-acquired methicillinresistant Staph. They nearly all have this Panton-Valentine leukocidin. The Staph produces a lot of different enzymes that, when it’s present in the body, can damage tissue. And this is part of the reason that you get liquefactive necrosis when you have an abscess due to this organism. That’s due not only to the enzymes that the PMNs are secreting to try to kill the bacteria, but it’s also from the enzymes that the bacteria is secreting to help spread through the human body. There a lot of these different toxins that aren’t produced by every strain of Staph. So this is why not every Staphylococcal disease is the same. For example, there is one disease referred to as the “Scalded Skin Syndrome” because of a toxin that’s produced by some strains of Staph called the exfoliatin toxin. Literally what it does if the Staph gets into the body or onto the skin and produces this toxin, it interrupts the intercellular skin junctions and causes the skin to literally slough Microbiology: Gram-Positive Cocci Sonia Nkashama pg. 4 off. It looks like if you had a bad burn, got a blister, and then the skin peeled off. That’s what the skin looks like because of this toxin that the Staph is producing. Another thing that you see is the toxic shock toxin. In the late 1970s, this was first described as an entity called “Toxic Shock Syndrome.” This syndrome is due to the toxic shock toxin that’s produced by the Staph; this toxin is referred to as a superantigen. It stimulates the T cells to release lots of cytokines and the proinflammatory cytokines. Ultimately what you get is endothelial damage to the capillaries in the skin and this is why you get leakage of the capillaries and you get a rash associated with this. Staph can also cause food-borne disease. Along with the other Gram-(-) bacteria, the enterotoxins that are produced by some strains of Staph are actually known to produce food poisoning because they stimulate vomiting by interaction with the GI neural receptors. So this is where you can actually get a food-borne disease by eating the toxin while eating the bacteria. If you ingest the toxin, as may be found in potato salad or ice cream or other foods that have not been properly maintained or refrigerated, the Staph, if they grow in these foods, can produce the toxin. Then if you ingest the toxin, whether you ingest the bacteria or not, you can get the toxin acting in your body and mainly producing a self-limiting disease that includes a lot of vomiting. 12. This is an example of some of the skin and soft-tissue diseases that Staph produces. Impetigo is a disease that is commonly seen in young children; it can be caused by Staph, as well as Streptococcus pyogenes. This is typical of what you see here. You see a reddened area of the cell & a lot of “honey-crusted” scabbed-over skin lesions. Kids especially get it on their arms and legs. So the pathogenesis of this is that children, especially in the summer months, may be playing outdoors & wearing shorts. If a mosquito or another insect bites the leg or the arm, it itches. So the child scratches it. And if there is dirt on the hands or the fingernails, by scraping the skin you finish what the insect bite has already started, and you break the skin. Then these Staph that are present in the environment get into the intact skin, and they start causing these lesions. Staph uses all of these different virulence factors that it produces to spread throughout the skin, and you get these coalescing lesions like you see here. Where you have a pus-filled lesion is a furuncle or a boil. If you get several of these spreading together like this, you can refer to them as carbuncles. So you can get little local abscesses or you can get conditions that we refer to as cellulitis, which is actually a spreading of inflammation without an obvious pocket of pus. This is a little furuncle on the eyelid, and all of this area on the face where you see this red, erythematous area is all cellulitis. And one of the bad things that you can get from something like this or from a direct invasion of the body is entrance in the bloodstream where the bacteria can travel throughout the body. And when they do that, you run the risk of getting the organisms settling on a heart valve and causing endocarditis. And that’s a very serious consequence. Anytime you have a damaged heart valve (or even if you don’t have a damaged heart valve), if you get a virulent organism in the bloodstream, there’s always the concern that the bacteria can land on the heart valve and multiply, ultimately damaging the heart valve and causing heart failure. Occasionally you will see Staph as the cause of brain abscesses or meningitis or even epidural abscesses. We had a case that I heard about just last month from an elderly man who was having a lot of back pain due to osteoarthritis. So one of the treatments they do for back pain is they give an epidural block. They will inject steroids and anesthetics into the spinal area, into the epidural space to relieve the pain. Well, this man had this block, and shortly after he developed an abscess at the site of the epidural injection. And he had a severe and protracted hospital course as a result of this. Ultimately they showed the abscess by doing x-rays of the spine, and you could see a large developing cavity of abscess. This had to be drained surgically, and it was S. aureus that had almost certainly been introduced into this area when he had the injection. So it was a complication of the injection that he had that he got this epidural abscess that he had. Microbiology: Gram-Positive Cocci Sonia Nkashama pg. 5 13. This is a child with the scalded skin syndrome. This is the toxic shock syndrome, the rash that you see here on the buttocks and the legs. Staph is a cause of pneumonia; we don’t think of Staph as an important cause of the community-acquired pneumonia. But for pneumonia in people who are in the hospital (especially those who are on mechanical ventilation), S. aureus, esp. the methicillin-resistant one, are important pathogens of nosocomial , esp. ventilator-associated, pneumonias. S. aureus is the single most common cause of osteomyelitis, aka bone infections. It’s almost always due to this organism; it’s a very successful pathogen that can cause bone infections. It can also get into the urinary tract, although we don’t think of it as common in the urinary tract. 14. The treatment of Staph infections has been complicated by the increase in the oxacillin- or methicillinresistant organisms. We have been dealing with these in the hospital as important nosocomial pathogens that spread from person to person for the last 25 years. In the last five years, a new strain of this called the community-associated MRSA that people are actually bringing in the hospital is causing a lot of people to seek medical care for skin infections. People are getting bad abscesses on the skin and other cutaneous areas. At first they think that they had an insect bite or a spider bite that got infected, but that probably had nothing to do with it. They probably just got a MRSA that caused a bad abscess formation. Sometimes they’re sick enough to have to come into the hospital. You can drain the abscess, but you also have to give antibiotics. But the problem with this is that physicians in ambulatory care clinics and ERs and other places are not accustomed to dealing with these drug-resistant bacteria, so sometimes they are prescribing the wrong antibiotics because they don’t realize that we now have these drug-resistant bacteria. The term MRSA is the abbreviation for methicillin-resistant S. aureus. Methicillin is an antibiotic that was introduced in the 1960s; it is no longer used. We don’t even use it to test susceptibility because it doesn’t work well in the lab. We actually test oxacillin in the lab. But the name MRSA was developed over 20 years ago, and it has stuck with the organism. Even though we don’t use methicillin to identify the resistance and we don’t use it to treat the patient, it’s still the name that you will hear. The thing that you have to remember about that is that MRSA are resistant to all the other β-lactam antibiotics, so we have to use a drug like vancomycin to treat them. And now because we are using so much vancomycin, we are beginning to see some vancomycin-resistant Staph’s as well. So that really limits our treatment options even further because we don’t have very many good treatments for the vancomycin-resistant MRSA. So that’s just an important change that we are seeing in the Staphylococcus. 15. So now let’s move from the S. aureus to another group of the Staphylococci that we lump collectively as the coagulase-negative staphylococci. They are not nearly as virulent or as successful as pathogens. Usually you have to have something to help them along to cause disease, whereas S. aureus can certainly cause disease in a normal host. We refer to organisms like this as opportunistic infections. I mentioned bacteremias and endocarditis; well, bacteremias often occur in people that have an IV in. Endocarditis typically occurs in people that shoot up IV drugs (heroin, etc) and use dirty needles. Because when they inject the IV drugs, they are injecting the bacteria into their veins. So endocarditis in the right side of the heart, in the tricuspid valve in particular, is most commonly caused by S. epidermidis. And it’s largely because of the contaminated needles that the drug users use. We also see this as a cause of infection in newborn babies that often have IVs, usually the premature ones. And S. saprophyticus is one of the many species of the coagulase-negative Staph that causes urinary tract infections. If you look at an agar plate, you can often tell whether an organism is likely to be S. aureus or S. epidermidis by looking at the colonies. Remember that S. aureus will be large, creamy colonies with an off-white Microbiology: Gram-Positive Cocci Sonia Nkashama pg. 6 appearance and will be β-hemolytic. The S. epidermidis colonies will usually be white and not hemolytic. A major virulence factor for these organisms is this polysaccharide “slime” layer that they secrete on their surfaces that allow them to attach to catheters, etc. that helps them invade the body. 16. Now we’ll say some things about the Streptococci, which are also very important human pathogens. They are Gram-positive cocci like the Staph. One of the things that you can look at if you do a Gram stain and get a good actively growing culture from body fluid is that streptococci, instead of growing in clumps, more typically grow in pairs or short chains or long chains like necklaces. Now you can not absolutely tell by looking at a Gram stain whether it’s a staph or a strep, but if you see predominately chains like this, you will see the strep. The staph are mostly in clumps, and the strep are mostly in chains. But you can see some of them that are sort of inbetween. Then some of them will be little tetrads like this. So it’s not absolute. But you can easily tell the difference between a staph or a strep, if the organism is growing, by doing a catalase test. 17. One of the other things that you will be looking at in the lab and that you will need to get an appreciation for is to be able to identify and describe the different hemolytic reactions of bacteria. And the streptococci will produce the whole spectrum of hemolysis, which we refer to as alpha, beta, and gamma. Beta-hemolysis is the complete hemolysis, the complete lysis of red blood cells by the hemolytic toxins of the organism. The alphahemolysis is a partial hemolysis; this will appear as a green area on the blood agar. In other words, the agar won’t be completely clear (where the cells have been lysed completely). Some of the cells will have been lysed, so you will see a green pigment appearing where the attacked red cells were. And then if you have no hemolysis, this is referred to as gamma-hemolysis. And that’s where you see the bacteria growing on the plate, but you don’t see any evidence of the destruction of the red blood cells. And this is one of the ways that we actually classify the streps. We’ll talk about the beta-hemolytic streptococci versus the alpha-hemolytic streptococci. The beta-hemolytic streptococci could also be classified according to their Lancefield groups. Now Rebecca Lancefield was a microbiologist that discovered 60+ years ago that the beta-hemolytic streptococci had different carbohydrates making up their cell wall and antigens. These were unique to the different groups, and they were immunologically distinct. So she named the groups alphabetically as the different beta-hemolytic streptococci because of the group-specific cell wall polysaccharides. And the alpha-hemolytic streptococci have their own groups as well. You can also group the streptococci as far as species with different phenotypic biochemical reactions. We actually use a combination of all these things when we are in a clinical lab describing diseases and lab characteristics of the strep’s. 18. Much like the staph’s, the strep’s are ubiquitous microorganisms. They are present all throughout the body; they are very successful human pathogens. For example, some of the α-hemolytic strep’s, the viridans streptococcus group includes strep mutans (an important organism that causes dental caries). The Strep’s are very common in the mouth. And that’s the association in there with the mutans streptococci with the production of dental caries; that’s an important ecological niche that these organisms use. These are not the β-hemolytic streptococci; they are α-hemolytic. Also during the winter months, 1/5 (or 20%) of young children may carry group-A strep (β-hemolytic), which causes strep throat, in their pharynx. But not all of them will get sick, but they can spread it to one another. S. pneumoniae is one of the α-hemolytic streptococci, and it’s commonly carried in the respiratory tract of asymptomatic persons. It’s an important cause of ear infections and pneumonia. The enterococci used to be grouped in the streptococcus genus, but in the 1980s, they were given their own separate genus. Enterococci are organisms found mainly in the enteric organs, like the GI tract, where they Microbiology: Gram-Positive Cocci Sonia Nkashama pg. 7 are normal flora. They have now evolved as important hospital pathogens because of developed resistance to antibiotics such as vancomycin. They can spread from person to person easily, and they can cause bloodstream infections and other GI-type infections. They are selected for in patients where there has been a lot of antibiotic use because they are resistant to a lot of antibiotics used in the hospital. The streptococci are very easily spread by airborne droplets, direct contact, or inanimate objects like fomites (needles, etc). They are very successful pathogens. 19. There are some things we have to do to distinguish the strep from one another. Looking at them, this is what the strep would look like in a bloodstream infection that had been grown in our blood culture instrument in the clinical lab. You can see here very characteristic Gram-positive cocci and chains sitting around here in the RBCs. Now if you have a patient with pneumonia and you want to know what the cause of it is, you can do a Gram stain of the patient’s sputum. If you see inflammatory cells in the sputum (like seen on this slide) and Grampositive cocci in pairs (called Gram-(+) diplococci) and short chains, you can suspect that this is going to be S. pneumoniae. That’s a typical appearance of a patient with pneumococcal pneumonia. They are going to be catalase-negative, and most of them will grow on sheep blood agar. They’re aerobic organisms, but some of them are obligate anaerobes. Many of them are capnophilic; they have the ability to grow in CO2 and grow better in the presence of CO2. We have antigenic grouping that we use to group the β-hemolytic streptococci. If you have a βhemolytic strep, you can take antibodies, put them on latex particles, and react that with your unknown strep and see which Lancefield group the organism falls into. We can also identify them biochemically with some fairly specific reactions that they may have. 20. There are a lot of cell surface structures on S. pyogenes, which is the prototype organism of the βhemolytic strep’s. You can compare/contrast them with the staphylococcus. They have a hyaluronic acid capsule, which is antiphagocytic. It can also produce a hyaluronidase enzyme that will help in tissue penetration, similar to staph. And of course, we mentioned the β-hemolysis and the group-specific carbohydrates and the peptidoglycan that does many of the same things for the strep that it does for the staph. There a lot of things that help it produce disease. 21. The M protein is a surface structure of the strep that is very important, since it’s a virulence factor. If you don’t have the M protein, organisms are much less able to cause disease because they are very easily oxidized and phagocytized. It binds fibrinogen and fibrin and forms a coating on the organism’s surface to help block complement. Antibody against the M protein is a very important protective mechanism. But since you have 80+ different types of S. pyogenes that have different M protein types, you can get re-infections over and over with different strains of S. pyogenes. The single most important thing that we need to mention is rheumatic fever. Rheumatic fever is an autoimmune disease. When you have a throat infection with S. pyogenes and if you have the rheumatogenic strains that have a particular M protein, your body makes antibody against the M protein on the strep. And that antibody cross-reacts with antigens in the heart; as a result of that, you can get rheumatic fever—damage to the myocardium and heart valves. This can cause heart valve dysfunction. This is important for dentists because anyone with a history of rheumatic fever, a heart murmur, etc. is at risk for getting an infection on the heart valves, especially after dental work. This history would tell you to be sure to pay attention because if you are doing dental procedures that could result in a transient bacteremia in abnormal heart valves because of the rheumatic fever, these patients are at risk for developing endocarditis.