Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neonatal infection wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Hepatitis B wikipedia , lookup
Marburg virus disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hepatitis C wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Typhoid fever wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Meningococcal disease wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Leptospirosis wikipedia , lookup
Gastroenteritis wikipedia , lookup
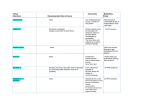
CROSS INFECTION CONTROL IN CHILDCARE Prevent the spread of infections by ensuring: routine immunisation, high standards of personal hygiene and practice, particularly hand washing and maintaining a clean environment. Please contact the Public Health Agency – Health Protection ‘Duty Room’ on 02890 553994/7 or visit www.publichealth.hscni.net or www.gov.uk/government/organisations/public-health-england if you would like any further advice or information, including latest guidance. RASH AND SKIN INFECTIONS Recommended period to be kept Disease away from the setting Athletes Foot None Chickenpox* Five days from onset of rash. Cold sores None (Herpes simplex) German Measles (Rubella) Six days from onset of rash. Hand, foot and mouth None Impetigo Measles Molluscum contagiosum Ringworm Roseola (infantum) Comments Athlete’s foot is not a serious condition – treatment is recommended. See: vulnerable children and female staff – pregnancy. Avoid kissing and contact with the sores. Cold sores are generally mild and selflimiting. Preventable by immunisation of MMR x 2 doses. See: female staff – pregnancy. Contact the duty room if a large number of children are affected. Exclusion may be considered in some circumstances. Until lesions are crusted and healed or Antibiotic treatment speeds healing and 48 hours after commencing antibiotic reduces the infectious period. treatment. Preventable by immunisation of MMR x 2 Four days from onset of rash. doses. See: female staff – pregnancy. None A self-limiting condition. Exclusion not usually required. Treatment is required. None None Scabies Child can return after first treatment. Household and close contacts require treatment. Scarlet Fever Child can return 24 hours after commencing appropriate antibiotic treatment. Antibiotic treatment recommended for the affected child. Slapped cheek (fifth disease or parvovirus B19) None See: vulnerable children and female staff – pregnancy. Shingles Exclude only if rash is weeping and cannot be covered. Warts and verrucae None Can cause Chickenpox in those who are not immune i.e. have not had Chickenpox. It is spread by very close contact or touch. If further information is required, contact the Duty room. See: vulnerable children and female staff – pregnancy. Verrucae should be covered in swimming pools, gymnasiums and changing rooms. DIARRHOEA AND VOMITING ILLNESS Recommended period to be kept Disease away from the setting Diarrhoea and / 48-hours from last episode of or vomiting diarrhoea and vomiting. E. coli O157 VTEC Typhoid [and paratyphoid] (enteric fever) Shigella (dysentery) Cryptosporidiosis Should be excluded for 48 hours from the last episode of diarrhea. Further exclusion may be required for some children until they are no longer excreting Should be excluded for 48 hours from the last episode of diarrhea. RESPIRATORY INFECTIONS Recommended period to be kept Disease away from the setting Flu (influenza) Until recovered. Tuberculosis Always contact the Duty room. Five days from commencing antibiotic Whooping cough treatment, or 21 days from onset of (pertussis) illness if no antibiotic treatment. OTHER INFECTIONS Recommended period to be kept Disease away from the setting Comments Further exclusion may be required for young children under five and those who have difficulty in adhering to hygiene practices. This guidance may also apply to some contacts who may require microbiological clearance. Please consult the Duty Room for further advice. Exclusion from swimming is advisable for two weeks after the diarrhea has settled. Comments See: vulnerable children. Requires prolonged close contact for spread. Preventable by vaccination. After treatment, non-infectious coughing may continue for many weeks. The Duty room will organise any contact tracing necessary. Comments If an outbreak/cluster occurs, consult the Duty room. Family contacts must be excluded until cleared to return by the Duty room. Preventable by vaccination. The Duty room will organise any contact tracing necessary. Conjunctivitis None Diphtheria Exclusion is essential. Always consult with the Duty room. Glandular Fever None Headlice None Treatment is recommended only in cases where live headlice have been seen. Hepatitis A Exclude until seven days after onset of jaundice (or seven days after symptom onset if no jaundice). In an outbreak of hepatitis A, the Duty room will advise on control measures. None Hepatitis B and C and HIV are bloodborne viruses that are not infectious through casual contact. For cleaning of body fluid spills. See: Good hygiene practice. Hepatitis B / C HIV / Aids OTHER INFECTIONS / cont....... Recommended period to be kept Disease away from the setting Meningococcal meningitis / septicaemia Until recovered. Meningitis due to Until recovered. other bacteria Meningitis viral None MRSA None Mumps Exclude child for five days after onset of swelling. Threadworms None Tonsillitis None Comments Meningitis C is preventable by vaccination. There is no reason to exclude siblings or other close contacts of a case. The Duty room will advise on any action needed. Hib and pneumococcal meningitis are preventable by vaccination. There is no reason to exclude siblings or other close contacts of a case. The Duty room will give advice on any action needed. Milder illness. There is no reason to exclude siblings and other close contacts of a case. Contact tracing is not required. Good hygiene, in particular hand washing and environmental cleaning, are important to minimize any danger of spread. If further information is required, contact the Duty room. Preventable by vaccination of MMR x 2 doses. Treatment is recommended for the child and household contacts. There are many causes, but most cases are due to viruses and do not need an antibiotic. Outbreaks: if a setting suspects an outbreak of infectious disease, they should inform the Duty Room.