Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
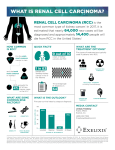
Renal Pathology Introduction: • 150gm: each kidney • 1700 liters of blood filtered 180 L of G. filtrate 1.5 L of urine / day. • Kidney is a retro-peritoneal organ • Blood supply: Renal Artery & Vein • One half of kidney is sufficient – reserve • kidney function: Filtration, Excretion, Secretion, Hormone synthesis. Kidney Location: Kidney Anatomy: Renal Pathology Outline • Glomerular diseases: Glomerulonephritis • Tubular diseases: Acute tubular necrosis • interstitial diseases: Pyelonephritis • Diseases involving blood vessels: Nephrosclerosis • Cystic diseases • Tumors Clinical Syndromes: • Nephritic syndrome. – Oliguria, Haematuria, Proteinuria, Oedema. • Nephrotic syndrome. – Gross proteinuria, hyperlipidemia, • Acute renal failure – Oliguria, loss of Kidney function - within weeks • Chronic renal failure. – Over months and years - Uremia Introduction • Functions of the kidney: – excretion of waste products – regulation of water/salt – maintenance of acid/base balance – secretion of hormones • Diseases of the kidney – glomeruli – tubules – interstitium – vessels Abnormal findings • Azotemia: BUN, creatinine • Uremia: azotemia + more problems • Acute renal failure: oliguria • Chronic renal failure: prolonged uremia Nephrotic syndrome Nephritic syndrome • Massive proteinuria • Hematuria • Hypoalbuminemia • Oliguria • Edema • Azotemia • Hyperlipidemia/-uria • Hypertension Glomerular diseases – Nephrotic syndrome • Minimal change disease • Focal segmental glomerulosclerosis • Membranous nephropathy – Nephritic syndrome • Post-infectious GN • IgA (immune) nephropathy Nephrotic Syndrome • Massive proteinuria • Hypoalbuminemia • Edema • Hyperlipidemia • Lipiduria Causes • Adults: systemic disease (diabetes) • Children: minimal change disease • Characterized by loss of foot processes • Good prognosis Minimal change disease Minimal change disease Normal glumerular structure Minimal change disease Normal glomerulus Focal Segmental Glomerulosclerosis • Primary or secondary • Some (focal) glomeruli show partial (segmental) hyalinization • Unknown pathogenesis • Poor prognosis Focal segmental glomerulosclerosis Membranous Glomerulonephritis • Autoimmune reaction against unknown renal antigen • Immune complexes • Thickened GBM • Subepithelial deposits Membranous glomerulonephritis Nephritic Syndrome • Hematuria • Oliguria, azotemia • Hypertension Causes • Post-infectious GN, IgA nephropathy • Immunologically-mediated • Characterized by proliferative changes and inflammation Post-Infectious Glomerulonephritis • Child after streptococcal throat infection • Immune complexes • Hypercellular glomeruli • Subepithelial humps Post-infectious glomerulonephritis IgA Nephropathy • Common! • Child with hematuria after (URI) Upper Respiratory Infection • IgA in mesangium • Variable prognosis IgA nephropathy URINARY TRACT INFECTION • Tubular and interstitial diseases – Inflammatory lesions • pyelonephritis Pyelonephritis • Invasive kidney infection • Usually ascends from UTI • Fever, flank pain • Organisms: E. coli, Proteus Urinary Tract Infection • Women, elderly • Patients with catheters or mal-formations • Dysuria, frequency • Organisms: E. coli, Proteus Acute pyelonephritis with abscesses Pyelonephritis Cellular cast Chronic pyelonephritis Drug-Induced Interstitial Nephritis • Antibiotics, NSAIDS • IgE and T-cell-mediated immune reaction • Fever, eosinophilia, hematuria • Patient usually recovers • Analgesic nephritis is different (bad) Drug-induced interstitial nephritis Acute Tubular Necrosis • The most common cause of ARF! • Reversible tubular injury • Many causes: ischemic (shock), toxic (drugs) • Most patients recover Acute tubular necrosis Benign Nephrosclerosis • Found in patients with benign hypertension • Hyaline thickening of arterial walls • Leads to mild functional impairment • Rarely fatal Benign nephrosclerosis Malignant nephrosclerosis • Arises in malignant hypertension • Hyperplastic vessels • Ischemia of kidney • Medical emergency Malignant Hypertension • 5% of cases of hypertension • Super-high blood pressure, encephalopathy, heart abnormalities • First sign often headache, scotomas • Decreased blood flow to kidney leads to increased renin, which leads to increased BP! • 5y survival: 50% Malignant hypertension Adult Polycystic Kidney Disease • Autosomal dominant • Huge kidneys full of cysts • Usually no symptoms until 30 years • Associated with brain aneurysms. Adult polycystic kidney disease Childhood Polycystic Kidney Disease • Autosomal recessive • Numerous small cortical cysts • Associated with liver cysts • Patients often die in infancy Childhood polycystic kidney disease Medullary Cystic Kidney Disease • Chronic renal failure in children • Complex inheritance • Kidneys contracted, with many cysts • Progresses to end-stage renal disease • Tumors – Renal cell carcinoma – Bladder carcinoma Renal Cell Carcinoma • Derived from tubular epithelium • Smoking, hypertension, cadmium exposure • Hematuria, abdominal mass, flank pain • If metastatic, 5y survival = 5% Renal cell carcinoma Bladder Carcinoma • Derived from transitional epithelium • Present with painless hematuria • Prognosis depends on grade and depth of invasion • Overall 5y survival = 50% Bladder carcinoma Thank you