Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
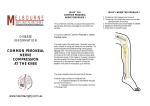
Neuro Anatomy Lumbar Spine Spinal Nerves Spinal nerves emerge from dura mater as ventral (anterior) and dorsal (posterior) nerve roots The ventral nerve root carries motor information away from the spine The dorsal nerve root carries sensory information from the body to the spine The dorsal root ganglion contains the cell bodies of the sensory neurons The dorsal root ganglion is particularly sensitive and is often the cause of radicular pain The two nerve roots then come together as they go through intervertebral foramen They will then split into ventral and dorsal rami to become peripheral nerves Dorsal rami supplies posterior back muscles Ventral rami progress into forming a plexus supplying the rest of the body Lumbar Nerve Roots The lumbar nerve root is named by the vertebrae above e.g the nerve below L2 vertebrae is L2 Lumbar Plexus Formed by the ventral rami of the first, second, third and part of the fourth lumbar nerves Form within the substance of psoas major First lumbar nerve divides into upper and lower branches Upper branch divides into iliohypogastric and ilioinguinal nerves Lower branch joins upper branch of second lumbar nerve to form genitofemoral nerve Lower branch of second lumbar nerve joint third and upper part of fourth to form anterior and posterior divisions Anterior divisions form the obturator nerve Posterior divisions form the femoral nerve Obturator Nerve From Anterior divisions of the lumbar plexus Root Value L2,3,4 Anatomy Merges in the substance of psoas major descending and emerging at the medial border of the muscle lateral to the sacrum Passes through the obturator canal and divides into anterior and posterior branches 1 These branches continue to descend through the adductor muscle group Muscles Supplied Adductor longus Adductor brevis Adductor magnus Gracilis Obturator externus Pectineus Cutaneous branch Medial aspect of the thigh Femoral Nerve From Posterior divisions of the lumbar plexus Root Value L2, 3, 4 Anatomy Emerges from the lateral border of psoas major running between psoas and iliacus Passess below the inguinal ligament The nerve then divides into various branches supplying the anterior lower limb The saphenous nerve arises approx. 3cm below the inguinal ligament and passes inferiorly and along the medial side of the leg finishing at the first metatarsal The saphenous nerve can often be a source of medial knee pain during squating Muscles Supplied Iliacus Sartorius Quadriceps femoris Cutaneous Branch Anterior cutaneous nerve of thigh Saphenous nerve Lumbosacral Plexus Formed by the ventral rami of the fourth lumbar to fourth sacral nerves Lies on the posterior wall of the pelvis between piriformis and its fascia Sciatic Nerve From Anterior divisions of the lumbar plexus 2 Root Value L4,5, S1, 2, 3 Anatomy Leaves the pelvis and enters gluteal region through greater sciatic foramen below piriformis Passes down back of thigh deep to hamstrings Divides into common peroneal and tibial nerve approx. 2/3 down the thigh but in some cases can be proximal to piriformis Muscles Supplied Hamstrings Hamstring part of adductor magnus Peroneal Nerve From Terminal branch of sciatic nerve Root Value L4, 5, S1, 2 Anatomy Passes along the upper lateral side of the popliteal fossa Wraps around the neck of fibula and splits into deep peroneal nerve and superficial peroneal nerve Deep peroneal and superficial peroneal nerves continue to pass down into the dorsum of the foot Muscles Supplied Peroneals Extensors of foot Tibialis anterior Cutaneous Branch Lateral cutaneous nerve of the calf Peroneal communicating branch Tibial Nerve From Terminal branch of sciatic nerve Root Value L4, 5, S1, 2, 3 Anatomy Passes along the upper medial side of the popliteal fossa 3 Passes underneath soleus and behind the medial malleolus into the plantar aspect of the foot The nerve then divides into the lateral and medial plantar nerves Muscles Supplied Gastrocnemius Soleus Plantaris Poplitieus Tibialis posterior Flexors of the foot Cutaneous Branch Sural nerve Peroneal communicating nerve Sural Nerve From Terminal branch of sciatic nerve Root Value L4, 5, S1, 2, 3 Anatomy Arises from tibial nerve between the two heads of gastrocnemius Passes down and behind the lateral malleolus and into the lateral foot The sural nerve only has a sensory component Neurodynamics 4 The Neurodynamic System Refers to the interaction of the nervous system with its surrounding structures Made up of 3 components o Mechanical Interface All the structures that surround the nervous system, i.e tendons, ligaments, fascia, blood vessels, disc etc o Neural Structures Brain, spinal cord, dura mater, nerve rootlets, nerve roots, peripheral nerves o Innervated Tissues Any structure that is innervated by a nerve If there is a restriction or alteration in any neural structure MTrP’s can develop in the muscles it may supply Sensory AND motor functions can be inhibited. Abnormal Neurodynamic System Can be the result of one or a combination of the following three components o Tension As the nervous system is connected at both ends it will act like a piece of string with certain movements taking up the slack increasing the amount of tension o Sliding The nervous system will slide in relation to the mechanical interface. There can be areas where the nervous system will struggle to slide through or between structures o Compression The mechanical interface can physically compress the nervous system Movement of the Nervous System Generally as a joint moves the neural structures move towards the joint distally and proximally. This temporarily increases the slack of the nerve surrounding the joint, allowing tension to be increased as the joint moves The sequence of movements can affect the localization of stress The first region to be moved or moved strongest will increase the chance of a response in this area Assessing Neurodynamics Start with standard straight leg raise 5 Change the mechanical interface o E.g ipsilateral lumbar side flexion will close the intervertebral foramen Check neural structures sliding and tensioners Check the innervated tissues o Dermatome, Myotome and Deep Tendon Reflexes o Also check anatomical muscular contraction vs muscular contraction under neural load Femoral Nerve Tension Test Position 1. Client side lying- tested side upper most 2. Clients down most hip and knee flexed 3. Clients cervical spine flexed 4. Therapist standing behind client 5. Therapists stabilises hip and holds medial aspect of knee Procedure 1. Knee flexion to 90° 2. Hip extension 3. Hip abduction to stress obturator nerve 4. Hip adduction to stress lateral femoral cutaneous nerve Sciatic Nerve Tension Test Position 1. Client supine 2. Therapist standing to side facing cephalad 3. Clients foot placed on therapists shoulder Procedure 1. Knee extension 2. Hip flexion 3. Hip internal rotation 4. Hip adduction 5. Lumbar contralateral flexion Peroneal Nerve Tension Test Position 1. As sciatic nerve tension test Procedure 1. As sciatic nerve tension test 6 2. Ankle plantarflexion 3. Ankle inversion Sural Nerve Tension Test Position 1. As sciatic nerve tension test Procedure 1. As sciatic nerve tension test 2. Ankle dorsiflexion 3. Ankle inversion Tibial Nerve Tension Test Position 1. As sciatic nerve tension test Procedure 1. As sciatic nerve tension test 2. Ankle dorsiflexion 3. Ankle eversion Slump Test- Spine, cord and meninges Position 1. Client sat over edge of bed 2. Therapist stood to clients side 3. One hand on clients head 4. One hand on clients foot Procedure 1. Posterior pelvic tilt 2. Cervical flexion 3. Ankle dorsiflexion 4. Knee extension Determining The Outcome Of A Test Neurodynamic tests are never positive or negative They are best describes as normal or abnormal Abnormal results include o Reproduction of clients familiar symptoms (pain or radiculopathy) that is altered through structural differentiation o Reduced OR Increased range of movement compared to normal side o Reproduction of pain or radiculopathy in an area that they would not be expected confirmed by structural differentiation 7 Therefore when writing patient notes the following can be used o SLR – Peroneal Nerve – Right- Abnormal- Reproduce lateral ankle pain- Decreased with hip abduction Structural Differentiation To determine whether symptoms reported during testing is due to the neurodynamic system structural differentiation must be used This is done in the following way o Elicit a response using a test and hold this position o Move a joint that is at least 2 steps away from the area of symptoms o If this increases/decreases symptoms the neurodynamic system is the structure at fault o Should symptoms remain exactly the same there is a mechanical cause to the clients symptoms during testing Dermatome Testing Test the dermatome patterns of the lumbar spine bilaterally simultaneously Abnormalities require further investigation which can be completed with sharp or blunt testing N.B there is considerable overlapping of dermatome patterns which often differ between texts Dermatome abnormalities that fail to respond to physiotherapy require investigation by a spinal or neurological specialist o L1: lower abdomen and groin, lumbar region between levels L2 and L4, upper, outer aspect of the buttock o L2: two separate areas: lower lumbar region and upper buttock, whole of the front of the thigh o L3: two separate areas: upper buttock, medial aspect and front of the thigh and leg as far as the medial malleolus o L4: lateral aspect of the thigh, front of the leg crossing to the medial aspect of the foot, big toe only o L5: lateral aspect of the leg, dorsum of the whole foot, first, second and third toes, inner half of the sole of the foot o S1: sole of the foot, lateral two toes, lower half of the posterior aspect of the leg o S2: posterior aspect of the whole thigh and leg, plantar aspect of the heel o S3: circular area around the anus, medial aspect of the thigh o S4: saddle area: anus, perineum, genitals, medial upper thigh o S5: coccygeal area Test the myotomes of the lumbar spine bilaterally and simultaneously where possible Maintain resistance for 5 seconds at least Nerve root weakness will be evident after 5 seconds, peripheral nerve weakness is evident immediately 8 Myotomal weakness requires further investigation by a spinal or neurological specialist Management Soft Tissue Release While holding the limb in a position that represents the abnormal tension test perform soft tissue release along the pathway of the peripheral nerve Mobilisations The neurodynamic system can be mobilised by either ‘sliders’ or ‘tensioners’ Sliders Tension is never increased through the nerve Point A and B of a nerve will always stay the same distance from one another Sliders are the treatment of choice for very irritable symptoms Tensioners Point A and B of a nerve will increase in distance from one another This can be done into resistance or symptoms, or can be completed before the onset of symptoms Joint Mobilisations Joint mobilisations can be performed during neural load E.g Slump sitting with peroneal nerve testing while performing inferior tibio-fibular mobilisations Home Exercise Programme Clients can be instructed of self- mobilisations to complete at home Caution-ensure correct technique of sliders and tensioners etc to avoid aggravation of symptoms Monitor symptom response from neurodynamic home exercise programmes as regular selfmobilisations may aggravate symptoms if done too aggressively and regularly 9