Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Implementation Guide for use
of SNOMED CT in Allergy and
Hypersensitivity Data Records
Subtitle
Date:
Version:
Status:
Document1
Status: Draft
20141315
0.02
Draft
Page 1 of 19
Date
<Document Name>
Version 0.01
Document1
Status: Draft
Page 2 of 19
Date
<Document Name>
Version 0.01
Amendment History
Version
Date
Editor
Kin Wah Fung
0.01
20141201
Bruce Goldberg
Jim Campbell
Amy Sheide
0.02
20150309
Beverly Knight
Kin Wah Fung
James Campbell
Comments
Glossary terms from IHTSDO discussions
Draft chapter from Bruce Goldberg
Addition of Background, Purpose, Scope,
Problem statement, Clinical use case
scenarios, proposal for inclusive
information model
Approvals
Version
Date
Approver
Comments
YYYYMMDD
Future Review Timetable
Review date
Responsible owner
Comments
YYYYMMDD
Person/group responsible
Summary of action
(remove or add rows if necessary)
© International Health Terminology Standards Development Organisation 2017. All rights
reserved.
Document1
Status: Draft
Page 3 of 19
Date
<Document Name>
Version 0.01
Table of Contents
1 Introduction ......................................................................................... 6
Background .............................................................................................. 6
Purpose .................................................................................................. 6
The benefits include: ................................................................................................... 6
Benefits for IHTSDO and its Members .............................................................................. 6
Benefits for SNOMED CT Implementers ............................................................................. 7
Benefits for SNOMED CT End-Users, Clinical Researchers, Health Provider Organizations, and Vendors7
Scope ..................................................................................................... 7
Audience ................................................................................................. 8
2 Statement of the problem ........................................................................ 8
3 Clinical use case scenarios........................................................................ 8
Documentation of an allergic reaction to a substance............................................ 8
Drug allergy or intolerance alert to provider ...................................................... 9
Additional scenarios clarifying scope for documentation of allergy/adverse reaction
statements .................................................................................................. 9
4 Survey of hypersensitivity information models .............................................. 10
Previous IHTSDO deliberations ...................................................................... 10
4.1.1 Historical perspective ........................................................................................ 10
4.1.2 Organization and features of hypersensitivity content currently in SNOMED CT .................. 12
Survey of reference information models and value sets ......................................... 13
4.2.1 HL7 CCDA model ............................................................................................... 13
4.2.2 HL7 Patient Care revised model ............................................................................ 13
4.2.3 FIHR .............................................................................................................. 13
4.2.4 epSOS ............................................................................................................ 13
4.2.5 openehr ......................................................................................................... 13
Proposal for inclusive information model .......................................................... 13
4.3.1 Propensity class ................................................................................................ 14
4.3.2 Adverse reaction (condition) class ......................................................................... 15
4.3.3 Sensitivity test result class .................................................................................. 15
5 SNOMED CT reference valuesets ............................................................... 16
6 Promoting interoperable EHR communication ............................................... 16
Document1
Status: Draft
Page 4 of 19
Date
<Document Name>
Version 0.01
7 Glossary of Terms ................................................................................ 18
Appendix A First Appendix ........................................................................ 19
A.1 First sub-heading if required ........................................................................ 19
Document1
Status: Draft
Page 5 of 19
Date
<Document Name>
Version 0.01
1 Introduction
Background
Interoperable deployment of SNOMED CT in support of Electronic Health Record (EHR)
hypersensitivity/allergy/adverse sensitivity data is inconsistent and fails to support interoperability
across IHTSDO member realms. This arises due to confusion regarding the scope and definition
of adverse sensitivity data, uncertainty regarding the reference models for defining relevant data
records and inconsistency in guidance for the appropriate value sets from SNOMED CT that
should populate those records.
This proposal expects to develop an implementation guide which will:
extend previous IHTSDO work on definitions of adverse sensitivity events,
survey and summarize the relevant interoperability standards,
advise the IHTSDO community regarding best practice deployment of allergy data within
the EHR and
identify the SNOMED CT refsets (value sets) that would constitute best practice for use in
electronic health records.
Several Standards Development Organizations (SDOs) such as HL7 and epSOS have also
provided some material to assist implementers, however without formal or informal collaboration
with IHTSDO.
There is recognition that some realms have developed their own Drug dictionaries which would be
preferred for use in hypersensitivity/allergy/adverse sensitivity data.
Purpose
This implementation guide is intended to accelerate consistent implementation of vocabulary with
an emphasis on the use SNOMED CT within the domain of allergy and adverse reaction.
This guide expects to develop an implementation guide which will:
extend previous IHTSDO work on definitions of adverse sensitivity events,
survey and summarize the relevant interoperability standards,
advise the IHTSDO community regarding best practice deployment of allergy data within
the EHR and identify the SNOMED CT refsets (value sets) that would constitute best
practice for use in electronic health records.
The benefits include:
Benefits for IHTSDO and its Members
Members will have uniform, clear best practices for documenting adverse sensitivity events
This work will support how adverse sensitivity information models such as HL7 can
incorporate SNOMED CT
Provide definitions for the community to clearly understand the terms of allergy, adverse
sensitivity, adverse reactions, etc
Document1
Status: Draft
Page 6 of 19
Date
<Document Name>
Version 0.01
Cost savings: reduce investment requirements by member vendor community; consolidate
NRC costs for SNOMED CT distribution of value sets
Benefits for SNOMED CT Implementers
Support interoperability within and between realms in a consistent way by providing clear
guidance for structuring Adverse sensitivity data as part of a patients Electronic Health
Record
Enable consistent adoption of SNOMED CT by providing guidance on the representation of
adverse sensitivity information with different levels of granularity, with and without the use
of post-coordination
Benefits for SNOMED CT End-Users, Clinical Researchers, Health Provider Organizations, and
Vendors
Fill the knowledge gap in the community of practice by providing authoritative guidance and
ref sets that can be used consistently for the representation of;
o an allergy, pseudoallergy and intolerance
o an adverse reaction
o the criticality of the allergic condition (ie the potential seriousness of a future
reaction)
o the severity of a reaction
Provide guidance for the aggregation & analysis of reported adverse drug reactions (ADR)
and sharing/interoperability of ADR reports
Scope
The MapSIG and Implementation SIG will supply volunteer effort for preparation and
documentation of the implementation guide and refsets. The approach will include identification of
the areas of overlap and synergy with work underway at various StandaredHL7,epSOS, and
openehr and determine how this work will be coordinated, aligned and disseminated in
collaboration with SDOs, national release center representatives and vendors.
It is expected the delivery will be as part of IHTSDO regular release cycle. The scope will include
phases:
Phase 1: Implementation guide including:
1. Statement of the problem and documentation of scope
2. Summary of definitions and reference standard publications
3. Advice for best practice deployment of the binding of information model-todomain ontology in support of adverse sensitivity record data
4. Documentation of refsets/value sets
Phase 2: Refset (Value Set) development:
1. Hypersensitivity conditions and dispositions
2. Allergenic substances: drugs, chemicals, foods, animals, environmental agents
3. Sensitivity types
4. Adverse reactions (clinical findings: signs, symptoms and diagnoses)
5. Certainty
6. Criticality
7. Severity
Document1
Status: Draft
Page 7 of 19
Date
<Document Name>
Version 0.01
8. Explore the use and approach of the SCT drug hierarchy for drug allergy content
(consideration for generic only)
Value set publication, maintenance, and governance plan including joint agreement between
IHTSDO, HL7 and NRCs
Audience
The audience of this implementation guide includes but is not limited to IHTSDO and its
Members. Specifically this guide is targeted at SNOMED CT Implementers SNOMED CT EndUsers, Clinical Researchers, Health Provider Organizations, and Vendors.
2 Statement of the problem
The capture and exchange of hypersensitivity/allergy/adverse sensitivity data varies across EHRs.
As an effect, much of this data is not interoperable across electronic systems. Confusion regarding
the representation and definition of adverse sensitivity data within the EHR presents challenges to
organizations that are trying to implement SNOMED CT for electronic data sharing. Further, this
uncertainty limits the use of hypersensitivity/allergy/adverse sensitivity data for clinical decision
support and longitudinal patient care records. The capture of allergy data must be clearly defined
to support patient safety and a comprehensive health record.
3 Clinical use case scenarios
Documentation of an allergic reaction to a substance
Scenario: A physician sees a patient in clinic for routine outpatient care. The patient has been
receiving care for diabetes and hypertension. Recently the patient was prescribed 25mg
hydrochlorothiazide for his blood pressure. He tells the physician that he has been having a lot
of itching lately and on examination, the physician notes hives. A review of systems fails to
reveal any other causes and the physician concludes that the patient is having an urticarial
reaction to hydrochlorothiazide; instructs the patient to stop the thiazide and employ
diphenhydramine for relief..
When preparing his encounter summary for the visit, the physician uses the EHR diagnosis list to
select his encounter diagnoses. He tries to find “Urticarial reaction to hydrochlorothiazide” but
the best he can locate is “89322006|Drug-induced urticaria|”. He employs a feature that the
vendor has supplied which allows him to choose a more specific diagnosis. The feature offers a
list of drugs causing the hives and he chooses “5487|Hydrochlorothiazide|”. The vendor
software creates a diagnosis reference in the EHR data dictionary for the diagnosis “Drug
induced urticaria due to hydrochlorothiazide” and creates an extension concept reference with
the full definition. The vendor mapping software suggests an ICD-10 diagnosis “L50.0 Y54.5” to
report the encounter. The vendor software asks if the physician wishes to make an update to
the allergy list.
Document1
Status: Draft
Page 8 of 19
Date
<Document Name>
Version 0.01
Drug allergy or intolerance alert to provider
Scenario: The clinic nurse calls the patient a week later with test results from his visit. She
inquires as to the urticarial and the patient verifies that they have disappeared with
discontinuation of the diuretic. Following clinic protocols she accesses the patient EHR and
proceeds to make a new entry into the allergy list. The software steps through a series of
questions asking: what was the offending agent, what were symptoms or findings resulting from
the reaction, what class of reaction occurred, what was the severity and criticality. The nurse
answers the questions and an allergy record appears in the list “Hydrochlorothiazide; Allergy;
Moderate severity; Moderate criticality; Symptoms-Hives”.
Years later the patient is seeing another physician for consultation on treatment of resistant
hypertension. The second physician decides that an ACE inhibitor/thiazide medication is
appropriate for the patient. When the physician creates an order for “Lisinoprilhydrochlorothiazide 20/25” and commits to the electronic prescription, an alert appears which
requires a response by the physician warning him of an allergy history to hydrochlorothiazide
which is an ingredient in the drug he is about to order. The physician retracts the order and
chooses another antihypertensive.
Additional scenarios clarifying scope for documentation of
allergy/adverse reaction statements
Animal allergy scenario: A physician sees a patient for the first time in clinic for routine
outpatient care. The patient tells the physician he has an allergy to cats. Upon further
exploration the physician learns the patient develops swollen and itchy eyes when in contact
with a cat. The physician documents the allergic propensity and reaction in the EHR ‘allergy
list’.
Non-drug allergy scenario: A patient reports to their physician that they react violently to
eating peanuts with symptoms that include generalized hives, wheezing and hypotension
requiring use of epinephrine for resuscitation. The physician records a peanut allergy with
anaphylaxis, hives and wheezing as reaction symptoms, records a criticality of high and reaction
severity of ‘severe’.
No Known Allergies scenario: A nurse is performing an intake examination on a patient that is
new to the clinical practice. As part of the clinical interview he inquires about medication
allergies. The patient reports that she is not allergic to any medications, foods, chemicals or
animals. The nurse opens the ‘hypersensitivity list’ in the EHR and documents ‘No known
allergies’ which electronically validates that the nurse inquired of the patient and that the
history was confirmed at the date and time recorded.
Document1
Status: Draft
Page 9 of 19
Date
<Document Name>
Version 0.01
4 Survey of hypersensitivity information models
Previous IHTSDO deliberations
4.1.1 Historical perspective
Efforts to revise the allergy-related hierarchies in SNOMED can be traced back to at least 2005
during which time several deficiencies were identified in the modeling of allergies and adverse
reactions involving the inconsistent use of the causative agent role and the need to clearly
differentiate the propensity to react from the reaction itself in order to better integrate with
proposed HL7 models for allergy. Thus allergy (disorder) was replaced by allergic state (disorder)
as a child of 420134006 | Propensity to adverse reactions (disorder) and adverse
reactions/allergy to various substances, food and drugs were updated in the 2006 release of
SNOMED CT.
Additional revisions to the SNOMED CT allergy content occurred in 2006 included an attempt to
align the terminology with the nomenclature for allergy developed by the WAO/EAAACI in 2001.
The most recent update to the allergy terminology was implemented for the July 2013 release of
SNOMED CT. This update organized all of the three main allergy classes (conditions, propensities
and reactions) which up to this point resided in three unrelated hierarchies under a single
“allergy condition” hierarchy. Additionally, the July 2013 release included a more robust
concept model for hypersensitivity/allergy conditions, particularly for the allergy propensity
class (since named allergic disposition). Text definitions for the major organizing classes were
also included for the first time.
Revising SNOMED CT to the three class model meant that hypersensitivity data were represented
by:
Dispositions (propensities) which model the patient state of an “Allergy to x”.
<<420134006|Propensity to adverse reactions(finding)|
Processes (reactions) Example: “Allergic reaction to x”. <<281647001|adverse reaction
(disorder)|
Conditions (may be either propensities or reactions) Example: “Allergic rhinitis due to x”.
<<473010000|Hypersensitivity condition (disorder)|
Abnormal structure was not felt to be relevant to this particular model.
An initial “Aspirational” model for allergy/hypersensitivity was constructed using formal
ontological principles based on BioTop.
Document1
Status: Draft
Page 10 of 19
Date
<Document Name>
Version 0.01
Figure 1 Aspirational Model of hypersensitivity
Realizing that such a model would be difficult to implement at least in the short term, several
features of this model were able to be represented using the current SNOMED CT description
logic and roles (see section IV Features of current implemented model for allergic conditions in
SNOMED CT).
Document1
Status: Draft
Page 11 of 19
Date
<Document Name>
Version 0.01
Figure 2 Current organization of hypersensitivity conditions in SNOMED CT
4.1.2 Organization and features of hypersensitivity content currently in SNOMED
CT
Top level terms fully defined by means of pathological process role using the following role
values:
472963003|Hypersensitivity process (qualifier value)|
o 472964009|Allergic process (qualifier value)|
472965005|Allergic sensitization process(qualifier value)|
o 609404002|Pseudoallergic process (qualifier value)|
A novel approach was taken to link a causative agent to the allergy disposition for purposes of
data retrieval. Since causative agents cause the realization of the disposition (the allergic
reaction process) and not the disposition itself (the allergic disposition) we allowed that only
processes and not dispositions can have causative agents. For this reason, in the “aspirational”
model, a unique property, agent_of_realization was created. In order to approximate this
Document1
Status: Draft
Page 12 of 19
Date
<Document Name>
Version 0.01
functionality using current SNOMED CT description logic, causative agent was linked to another
process (allergic sensitization) upon which the disposition is dependent using the following role
group:
Group {255234002|after (linkage concept)|=609327009|allergic sensitization (disorder)|,
246075003|causative agent (linkage concept)|= 105590001|substance (substance)|}
From this, an allergic disposition must necessarily follow an allergic sensitization caused by an
allergen.
Survey of reference information models and value sets
4.2.1 HL7 CCDA model
4.2.2 HL7 Patient Care revised model
4.2.3 FIHR
4.2.4 epSOS
4.2.5 openehr
Proposal for inclusive information model
After considering reference information models from various standards development
organizations and other national or regional sources, an inclusive information model is proposed.
This model aligns the essential elements of different information models into a coherent and
comprehensive model. Classes and data elements in the inclusive information model can be
mapped to individual models for compatibility.
The inclusive information model is made up of three classes. The Propensity class is the
centerpiece which must be present. A propensity class may be associated with zero-to-many
Adverse Reaction classes and zero-to-many Sensitivity Test Result classes. Note that in some
information models, propensity and adverse reactions are documented as a single entity. This is
unsatisfactory because a propensity may not be associated with a reaction (e.g., allergy
diagnosed by sensitivity test alone), or may be associated with more than one reaction (e.g.,
multiple exposure to a single allergen with different reactions). Moreover, a severe reaction may
not necessarily be a severe (or critically important) propensity, and vice versa.
The following tables depict the three classes and their data elements. Only data elements
specific to the allergy/intolerance use case are shown. Generic data elements such as date,
time, patient and provider identifiers are omitted.
Document1
Status: Draft
Page 13 of 19
Date
<Document Name>
Version 0.01
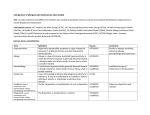
4.3.1 Propensity class
Table 1. Propensity class
Data element
Description
Notes
Substance
Represents the specific allergen or
other agent/substance to which the
patient has an adverse reaction
propensity. A substance is a physical
material which can mean a drug or
biologic, food, chemical agent, plants,
animals, plastics etc.
Must be present. Primary key
to identify a propensity
record and to link to the
corresponding adverse
reaction and sensitivity test
result records.
Substance type
Represents the type of substance
related to the propensity e.g. drug,
food, environment, vaccine etc.
This can usually be inferred
from the hierarchy in the
terminology used for
documenting the substance.
May need to be entered
separately if the substance
falls outside the terminology.
Propensity type
Indicates whether the propensity is of
an allergic nature or an intolerance to
a substance.
Propensity certainty
Indicates whether there is evidence
that the propensity has been
confirmed. For example, an allergy
could be further categorized as:
Confirmed - via laboratory testing or
witnessed observation or other strong
evidence, or Suspected (Unconfirmed)
- Patient reported but not further
verified by clinical history, diagnostic
testing or is uncertain.
Propensity
criticality
Indicates the potential seriousness of
the propensity for a future reaction.
This represents a clinical judgment
about the worst case scenario for a
future reaction. It would be based on
the severity of past reactions, the dose
and route of exposure that produced
past reactions, and the lifethreatening or organ system
threatening potential of the reaction
Document1
Status: Draft
Not the same as severity of
the reaction, because a
severe reaction can be noncritical and vice versa.
Page 14 of 19
Date
<Document Name>
Version 0.01
type. Criticality is an attribute of the
propensity, not the reaction(s).
Propensity status
Indicates the current status of the
propensity. For example, an allergy
may become ‘Resolved’ after desensitization.
4.3.2 Adverse reaction (condition) class
Data element
Description
Notes
Substance
Represents the specific allergen or
other agent/substance to which the
patient has an adverse reaction.
Must be present. Primary key
to identify an adverse
reaction record and to link to
the propensity record.
Reaction
manifestation
Indicates the specific adverse reaction
that occurred. Example: Rash, Hives
A negative entry (e.g., “no
adverse reaction observed”)
can be used to document an
exception to a propensity to
a class of substance (e.g.,
patient has penicillin allergy
but can tolerate amoxicillin)
Reaction severity
How severe the reaction was
Exposure type
How the exposure occurred. Example:
Vaccination, Prescription
Administration, Accidental
Observation method
How the observation was made e.g.,
patient reported, observed by family
member, observed by healthcare
professional
4.3.3 Sensitivity test result class
Data element
Description
Notes
Substance
Represents the specific allergen or
other agent/substance being tested.
Must be present. Primary key
to identify a sensitivity test
result record and to link to
the propensity record.
Sensitivity test
performed
Document1
Status: Draft
Page 15 of 19
Date
<Document Name>
Version 0.01
Sensitivity test
result
5 SNOMED CT reference valuesets
This section of the document is not going to contain the ref sets themselves but rather survey
the available ref sets that are related to allergy/hypersensitivity that are available from IHTSDO
and other organizations. It will also acknowledge that SNOMED CT will not be suggested as the
only terminology for allergy information but highlight what parts of SNOMED CT fit into the
inclusive information model above. Additionally, this section of the document is going to provide
a reference point on where implementers can find the allergy/intolerance ref sets.
6 Promoting interoperable EHR communication
This section of the document focuses on how this work applies to interoperable HER
communication. It also acknowledges that this is a living document and is going to be revised
and added to over time. It will acknowledge that there is a need for terminology modeling with
an information model as well as an understanding that mappings between information models
may be necessary for the fully integrated EHR across settings and countries. This section should
highlight ‘what’s next.’
<This is where the main content of the document is inserted. Please use the Styles to format
the text as follows:
Heading 1
First Level Heading (appears in the contents list)
Heading 2
Second Level Heading (appears in the contents list)
Heading 3
Third Level Heading (appears in the contents list)
Heading 4
Fourth Level Heading (does not appear in the contents list)
Appendix 1 First Level Heading for an Appendix (appears in the contents list)
Appendix 2 Second Level Heading for an Appendix (appears in the contents list)
DraftNote For text which is a drafting note and therefore needs to be attended to before the
document is finalised and approved. Draft notes must be removed from the document before it
can be approved. The Draft notes are automatically numbered for ease of reference and appear
in a red font.
List
For lists of items (that you may then also apply numbering or bullets to). This is
the same as the Normal style except there is no spacing between paragraphs and hence the
items in the list are closer together.
Normal
Document1
Status: Draft
For all other document content.
Page 16 of 19
Date
<Document Name>
Version 0.01
When using this template you must:
1. Edit the title on the first page to reflect the name of the document you are creating.
This title will then be automatically replicated in the Header of every subsequent page.
2. Edit the subtitle on the first page to appropriate text, or delete it if not required.
3. Edit the version number on the first page to reflect the version number of the
document. Version numbers start at 0.01 for the first draft, progressing through 0.02,
0.03 etc until the document is approved, at which point it becomes version 1.00. If the
document is subsequently amended, then the first draft of the amendment is version
1.01, the second draft 1.02 etc until the amended version is approved, at which point it
becomes version 2.00. Subsequent amendments of the document follow the same
pattern. The version number is automatically replicated in the Header of each page.
4. Edit the Status on the first page. This should have the value “Draft” until the document
is ready for approval, at which point you should change it to “Draft for approval”.
Following approval then prior to publication this should be set to “Approved” and the
version number set to the appropriate “x.00” value
5. Ensure the contents list and any cross references are updated by pressing Ctrl + A
(to select all the document text) and then pressing F9 to update all the fields. The
footers will not get updated unless you use Print Preview or double click the footer
and again press Ctrl + A and F9. Alternatively you can right click on an individual field
(such as the contents list) and select “Update Field” to just update that item.
6. Delete all the guidance text included in this document. This is formatted with the style
“guidance” and is included within the < > symbols. There is a macro called
“DeleteGuidance” that will remove all guidance text and this can be run by pressing
Alt+g, however depending upon your security settings you may have to enable macros for
this to be available (when opening this template you may have a Security Warning under
the toolbar providing you with the option to enable macros). CAUTION: please note that
this macro will delete all text that is formatted with the style “guidance” and therefore
if you have accidentally used this to format some of the text in your document, then it
will be deleted.
>
Document1
Status: Draft
Page 17 of 19
Date
<Document Name>
Version 0.01
7 Glossary of Terms
The following table contains the definition of any terms used within this document.
<insert any terms used within the document into the following table. This section should be the
last section of the document before any Appendices. If there are no terms requiring definition,
then delete this section.>
Term
Definition
Hypersensitivity condition
The disposition to develop an allergic or pseudoallergic
reaction, the reaction itself or its consequences.
Hypersensitivity disposition
The disposition to develop an allergic or pseudoallergic reaction
Hypersensitivity reaction
A pathological process initiated by exposure to a defined
stimulus at a dose tolerated by normal persons. It is the
realization of the disposition to hypersensitivity.
Allergic condition
The disposition to develop an allergic reaction, the allergic
reaction itself or its consequences
Allergic disposition
The disposition to develop an allergic reaction
Allergic reaction
A pathological immune process generally directed towards a
foreign antigen, which results in tissue injury, which is usually
transient. It is the realization of the allergic disposition. It is
most often applied to type I hypersensitivity but other
hypersensitivity types especially type IV (e.g. allergic contact
dermatitis) may be involved
Allergic sensitization
A process characterized by a humoral or cell-mediated immune
response to a foreign antigen resulting in the production of
specific antibodies and/or immune cells which may then lead to
an allergic disposition.
Pseudoallergic condition
The disposition to develop a pseudoallergic reaction, the
pseudoallergic reaction itself or its consequences
Pseudoallergic disposition
The disposition to develop a pseudoallergic reaction
Pseudoallergic reaction
A pathological nonimmune process generally directed towards a
foreign substance, which results in tissue injury, which is usually
transient. It is the realization of the pseudoallergic disposition.
A variety of mechanisms such as direct histamine release,
complement activation, cyclooxygenase activation and
bradykinin generation may be involved
Document1
Status: Draft
Page 18 of 19
Date
<Document Name>
Version 0.01
Appendix A First Appendix
A.1 First sub-heading if required
<insert content here>
Document1
Status: Draft
Page 19 of 19
Date