Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
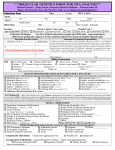
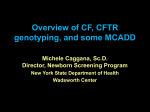
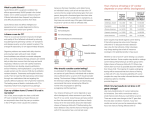
Improving test properties for neonatal cystic fibrosis screening in the Netherlands before the nationwide start by May 1st 2011 Geneva 30.08.2011 International Society for Neonatal Screening Martina Cornel, MD, PhD Professor of Community Genetics & Public Health Genomics, Dept Clinical Genetics Quality of Care EMGO Institute for Health and Care Research Cystic fibrosis • Mucoviscidosis • Lung infections • Nutritional problems www.nhlbi.nih.gov/.../Diseases/cf/cf_signs.html • Chronic obstructive pulmonary disease, pancreatic fibrosis, hepatic fibrosis, diabetes, azoospermia, etc. Life expectancy improved: now ± 40 y Dankert-Roelse, Lancet 1986 Autosomal recessive • 2 mutations in CFTR gene: infant develops disease • Most parents (80-90%) do not know in advance that they are (healthy) carriers Neonatal screening for cystic fibrosis? •First studies decades ago •IRT (dried blood spots) •Less days in hospital Wilcken & Chalmers 1985 •Wisconsin: Pseudomonas Aeruginosa in children diagnosed through newborn screening Sir Muir Gray (Nat Scr Comm UK) All screening programmes do harm. Some do good as well and, of these, some do more good than harm at reasonable cost. Pros and cons need to be evaluated • Live longer & healthier • Less days in hospital • Life expectancy increases? • False positives (referral for sweattest; in majority of cases this concerns healthy infants) • Uncertainty for days or weeks • # carriers and false positives New technological possibilities – Attunement between parties Achterbergh et al. Health Policy 2007; 83: 277-286. Neonatal screening for cystic fibrosis? Health Council report NL 2005: • 50-60 patients per year • 600 infants referred for sweat test • 400 heterozygotes diagnosed (carriers of CF) • prognosis improved after screening • Advice to perform Pilot Study: CHOPIN (Cystic fibrosis Heelprick screening in a newbOrn Population In the Netherlands). Balancing pros and cons Good test available? • False positives : 550/179.450 • Specificity (1-FP): 99,7% • False negatives • Sensitivity (1-FN) • Positive predictive value Disease → Present Absent Test Result↓ Positive Negative A B C D CHOPIN • PI Jeanette Dankert-Roelse • Publications submitted • Three provinces of NL • Protocols in parallel (IRT/PAP or IRT/DNA) • Summary of results in Health Council Report Four step protocol proposed: 1. IRT <60 µg/l: negative, otherwise 2. PAP < 1,0 µg/l if IRT < 100 µg/l or < 1,8 µg/l if IRT 60-100 µg/l : negative, otherwise 3. DNA panel of 36 most common mutations in NL • INNO-LiPA CFTR 19 and INNO-LiPA 17+Tn if 1 mutation or IRT ≥ 100 µg/l : 4. DNA sequencing of CFTR gene Screening protocol diagram www.gr.nl neonatal screening CF 2010 Expected to be reported to parents • 25 infants with cystic fibrosis – excl 4 with earlier diagnosis: meconium ileus • 12 carriers (heterozygotes) • Ministry of Health accepted Health Council advice and implementated by 1 May 2011 Preliminary results NL 3 months 11 patients sequencing: LiPA: 8 CF patients in 3 months 3 CF patients in 3 months www.gr.nl neonatal screening CF 2010 Benefits of screening • Better feeding status, prevention of an often protracted and aggravating diagnostic process and decrease in hospital admissions • Specificity 100% – Few referrals to pediatrician • Sensitivity – Panel: only 44% for Turkish migrants and 69% for North African migrants (Lakeman 2008) – Higher due to sequencing and failsafe in IRT≥100µg/l Additional benefits of screening Is carrier status information a benefit? • Complicating pre-test counseling: “If the newborn child is a carrier, then it follows that one, or both, parents (and possibly other children) are carriers. The parents should be alerted to these possible outcomes prior to screening. Information of this kind can, in practice, give rise to misunderstandings with regard to the health of the carriers. etc” “One problem lies in the fact that it is not always possible to determine for certain whether only one parent is a carrier (as is the case with, for example, cystic fibrosis, where not all mutations are known).” Phases of life & genetic screening • Preconceptional • Antenatal • Neonatal • Later in life Carrier screening – when? • Before pregnancy (in preconceptional screening) more reproductive options: – No children (adoption) – Preimplantation genetic diagnosis (embryo selection) – Prenatal diagnosis and termination of affected fetuses – Different partner – Donor gametes (artificial insemination donor sperm) – etc A CF carrier identified in NBS A a A A AA Aa A AA a Aa aa a Aa ? If child is carrier, at least one of parents is carrier as well. If 1:30 is carrier, the allele frequency is 1:60, and for each next pregnancy the risk of of CF affected infant is 1/4X1/60=1/240. Report carrier information from NBS? • Relevant for some parents in connection with future family planning • Secondary finding rather than objective • CF is a severe disorder – if requested, it would be necessary to provide genetic advice and treatment options. • Certainly, parents must be able to make an informed and conscious choice and the consent of parents is required for the provision of information on being a carrier. Opting out of carrier status information Conclusion • In the new program as of 1.5.2011 100% specificity is achieved • Sensitivity will be very high, further evaluation is needed, esp. for infants with migrant ancestors. • Carrier status information is provided to small #, if parents do not opt out, and clinical geneticist can provide counseling to carriers upon request. Thank you!