Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
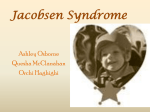
Ophthalmic Genetics, 27:1–7, 2006 c Taylor and Francis Group, LLC Copyright ISSN: 1381-6810 (print) / 1744-5094 (online) DOI: 10.1080/13816810500481832 RESEARCH REPORT The Ocular Manifestations of Jacobsen Syndrome: A Report of Four Cases and a Review of the Literature Garfield L. Miller and Sohel Somani University of Toronto, Toronto, Ontario, Canada Malgorzata J. M. Nowaczyk Clinical Genetics Service, McMaster University, Hamilton, Ontario, Canada Annette Feigenbaum, Ronald G. Davidson, and Teresa Costa University of Toronto, Toronto, Ontario, and Sainte-Justine Hospital and Université de Montréal, Montréal, Quebec, Canada Alex V. Levin University of Toronto and Department of Ophthalmology, Hospital for Sick Children, Toronto, Ontario, and Sainte-Justine Hospital and Université de Montréal, Montréal, Quebec, Canada Purpose: We report ophthalmic manifestations in four Jacobsen syndrome cases, review the literature, and suggest phenotype-genotype correlations. Methods: Chart review of Ocular Genetics Program patients at The Hospital for Sick Children, Toronto, Canada. Results: Four del11qter cases are presented. Hypertelorism/telecanthus, abnormally slanted palpebral fissures, abnormal retinal findings, nasolacrimal duct obstruction, anomalous extraocular muscles, amblyopia, and microcornea were found. Conclusions: We report typical findings and novel ocular presentations. Visual prognosis is generally good. Retinal dysplasia and coloboma seem associated with del11q23. ABCG4, NCAM, and Mfrp are candidate genes in this region that theoretically may be disrupted. Keywords Jacobsen syndrome; 11q terminal deletion disorder; 11q monosomy; review; eye findings INTRODUCTION A terminal deletion of 11q was first associated with specific clinical findings by Jacobsen and coworkers in 1973.1 Since then, more than 90 cases of terminal 11q deletion,2 most of them arising de novo, have been described as the clinical entity called Jacobsen syndrome, also known as the 11q terminal deletion disorder (Table 1).3 The most frequent breakpoints for the terminal deletion are located at 11q23.3 and have been attributed to the presence of fragile site FRA11B and other breakpoint clusters in the vicinity.4−6 A small number of patients have been reported in whom the 11q deletion was in the more distal 11q24 band, while still manifesting the Jacobsen phenotype. Band 11q24.1 has been suggested to be the critical region responsible for the typical features of the syndrome.7,8 This is supported by cases in which an 11q24.2-qter deletion was not associated with features characteristic of Jacobsen syndrome.7,9 Interstitial deletions proximal to 11q24.1, but involving 11q23, have also produced some of the features but a different overall phenotype.3,9,10 Ocular abnormalities most commonly associated with the 11q deletion disorder include telecanthus and/or hypertelorism, ptosis, epicanthal folds, and strabismus. Other ocular abnormalities such as unilateral or bilateral coloboma with or without microphthalmia,11,12 nuclear cataract,12 abnormal eyelashes/eyebrows,13,14 and iris discoloration have been variably reported.13 A review focused on the ocular findings of Jacobsen syndrome was recently performed by Lee et al.15 Most other reports have not thoroughly reported on ophthalmic Accepted 7 November 2005. Address correspondence to Alex V. Levin, M.D., MHSc, FRCSC, Department of Ophthalmology, M158, The Hospital for Sick Children, 555 University Avenue, Toronto, Ontario M5G 1X8, Canada. E-mail: [email protected] 1 2 G. L. MILLER ET AL. TABLE 1 Non-ocular clinical findings characteristic of Jacobsen syndrome Pre- and postnatal growth retardation Microcephaly Trigoncephaly or other craniosynostosis Mental retardation (mild to moderate) Short, flat nasal bridge with anteverted nares Short philtrum Carp mouth Micro/retrognathia Low-set ears with minor external malformations Miscellaneous minor hand anomalies Joint contractures Congenital heart disease Thrombocytopenia/pancytopenia were found with 11q deletions in the 11q23-24 region who did not have the Jacobsen phenotype. We included patients who had their deletions as part of a translocation only when the phenotype was consistent with Jacobsen syndrome. All of the patients in our database with translocations involving this region had a Jacobsen phenotype. CASE REPORTS findings, but have tried to make genotype-phenotype correlations. Here, we describe the ocular manifestations of four cases of Jacobsen syndrome seen in our clinic (Table 2), review the literature, and also look at chromosomal breakpoint correlations with ocular and oculofacial phenotypes. In our patients, we found many of the typical findings of Jacobsen syndrome, but also noted presentations rarely or never reported including funduscopic changes, nasolacrimal duct obstruction, amblyopia, and anomalous extraocular muscles. Case 1 This boy has a karyotype of 46,XY,del(11),+der(11)t(9;11) (p24.1;q24.2)mat. He was the first child of healthy nonconsanguineous parents. He was born at 38 weeks by cesarean section due to breech position, decreased intrauterine movements, and poor growth. His birth weight was 2375 g. Nonocular features in infancy included hepatosplenomegaly, developmental and growth delay, atrial septal defect, pancytopenia, recurrent ear infections, hearing deficit, lower limb hypertonia, upper limb hypotonia, and hyperreflexia. Dysmorphic features included widely spaced nipples, single palmar creases, anteverted nares, small mouth, and a prominent forehead (Fig. 1). METHODS We reviewed the records of all cases of 11q deletion with clinical features of the syndrome seen by one of the staff ophthalmologists (AVL) of the Ocular Genetics Program at The Hospital for Sick Children, University of Toronto. This program is a multidisciplinary ocular genetics service providing referral-based adult and pediatric care for much of the province of Ontario (population: approximately 12 million). Our database currently contains 14,254 patients, including those with retinoblastoma. We found four patients for inclusion in this report. No patients TABLE 2 Ocular findings in study patients Case 1 Case 2 Case 3 Case 4 11q24.2 11q23.3 11q23 11q23.3 Microcornea Exotropia Amblyopia Nystagmus Ptosis Nasolacrimal duct obstruction Retinal abnormality Optic atrophy ∗ Transient finding. + + + − − − − + − +∗ − + + + − +∗ − − − + − − + − − − +* − + − +∗ + FIG. 1. Case 1. Note characteristic facies, left head tilt, and right exotropia. THE OCULAR MANIFESTATIONS OF JACOBSEN SYNDROME 3 Ocular examination at one year of age revealed a comitant exotropia of 40 prism diopters that appeared exaggerated by the presence of gross hypertelorism. He also had downslanting palpebral fissures and bilateral microcornea (9.5 mm OU). The remainder of the examination, including dilated retinal examination, was within normal limits. At three years, he was astigmatic in both eyes (+0.50 + 0.75 × 60 OD, +0.50 + 0.75× 150 OS). He developed strabismic amblyopia that improved with occlusion of the right eye. When the child was 15 months old, the exotropia was corrected surgically with a bilateral lateral rectus recession of 4 mm. At surgery, he was noted to have anomalous extraocular muscles: the lateral rectus tendons were thin and tapered with narrow insertions (width 4.0 mm), although the muscle bellies appeared normal. A subsequent MRI showed the other extraocular muscles to be of normal size and location. Once the strabismus and amblyopia were successfully treated, a 30–45 degree non-ocular left head tilt, which had been intermittent pre-operatively, became more apparent and constant. The patient still has pseudo-exotropia from the prominent hypertelorism, but remains without true strabismus. No ocular, neurologic, or skeletal cause of the anomalous head position has been found. Follow-up visits at five and six years of age revealed no new findings. Case 2 This girl has a karyotype of 46,XX,del(11)(q23.3). She was the second of three children born to healthy non-consanguineous parents. She was born at term by cesarean section due to cephalopelvic disproportion. Her birth weight was 4 kg. She had developmental delay, recurrent urinary tract and lower respiratory tract infections, hearing deficit, hypotonia, and hyperreflexia. Dysmorphic features included low-set ears, anteverted nares with wide bridge of the nose, small mouth, and a prominent forehead (Fig. 2). She was referred to the Ophthalmology Service after parental concerns over her right eye, which appeared to ‘drift out’. Ocular examination at three months of age revealed absent fixation and following movements with occasional brief bursts of nystagmus. Vestibular induced nystagmus was intact and dampened appropriately. Optokinetic nystagmus was absent with only an occasional upward beat to a vertical stimulus. There was a comitant right exotropia of 30 prism diopters with full extraocular movements. Her pupils measured 5 mm in diameter bilaterally and were round with a sluggish reaction to light. No relative afferent pupillary defect was present. Dilated funduscopic examination revealed a mild cherry red spot bilaterally. Systemic evaluation revealed no other cause. An electroretinogram (ERG), performed in accordance with ISCEV standards,16 showed that all responses were at the lower limit of normal.17 At 12 months, the macula appeared normal and both eyes had normal age-appropriate fixation and following movements. The nystagmus had also resolved. Glasses were prescribed for FIG. 2. Case 2. Characteristic facies of Jacobsen syndrome. bilateral astigmatism (plano+2.50 × 90 OD, plano+3.00 × 90 OS). The patient also had a right nasolacrimal duct obstruction which was being managed conservatively. After being hospitalized for left periorbital cellulitis and left maxillary/ethmoid sinusitis, nasolacrimal duct probing and irrigation was successfully performed at 20 months of age. Her exotropia resolved spontaneously by two years of age. Case 3 This girl has a karyotype of 46,XX, del(11)(q23). She was the fourth child of healthy non-consanguineous parents. She was born at 38 weeks after an uncomplicated pregnancy and delivery. One sibling of the proband was diagnosed with cerebral palsy after a premature birth, while another sibling had strabismus but was otherwise normal. Non-ocular features in our proband with Jacobsen syndrome included developmental and growth delay, clinodactyly, toe syndactyly, thrombocytopenia, and pyloric stenosis. Dysmorphic features included a broad nasal bridge, anteverted nares, small mouth, dysmorphic external ears, and a prominent forehead. Ocular examination at two months of age revealed ageappropriate fixation in both eyes. Although vestibular induced 4 G. L. MILLER ET AL. nystagmus was normal, there was mild manifest symmetric horizontal nystagmus worse on side gaze. Extraocular movements were full, but there was a variable alternating exotropia of approximately 30–40 prism diopters. She had bilateral microcornea (9.5 mm OU). The anterior chambers were shallow. Pupils were normal with no relative afferent pupillary defect. Both corneas and lenses were clear. Dilated funduscopic examination was unremarkable except for a granular appearance throughout the retinal pigmented epithelium (RPE). There was a hyperopic refractive error in both eyes (+5.00 sphere). At seven months, her strabismus had resolved and vision responses remained normal. Follow-up at two years revealed no changes. The granular appearance of the RPE was still present, but no other signs of retinal dystrophy were noted. The inner canthal distance (ICD) was 31 mm (90th percentile), the measured interpupillary distance (IPD) 52 mm (97th percentile), and the palpebral fissure lengths 21 mm (<3rd percentile). The Mustarde index (ICD/IPD) was 0.59, indicating telecanthus.18 When examined at seven years of age, the mottling of the RPE was within normal limits. Case 4 This girl has a karyotype of 46,XX,del(11),+der(11)t(5;11) (q35.3;q23.3)pat. She was the first child of healthy nonconsanguineous parents. Delivery was at 34 weeks after premature rupture of the membranes. Birth weight was 2 kg. Non-ocular features included developmental and growth delay, thrombocytopenia, recurrent upper respiratory infections and otitis media, hearing deficit, a single left palmar crease, camptodactyly, and hypotonia. There was also a generalized skeletal dysplasia which manifested as shortened metatarsals, leg-length discrepancy, and decreased extension of the proximal interphalangeal finger joints. Dysmorphic features included dysplastic and low-set external ears, small mouth, and a prominent forehead. Ocular examination at 18 months of age revealed visual fixation that was central, steady, and maintained in the right eye. The left eye was central and steady, but not maintained. There was a history of mild bilateral ptosis, which had been surgically treated elsewhere. She had a left exotropia of 40 prism diopters with full extraocular movements. The pupils were normal with no relative afferent pupillary defect. The anterior chambers were unremarkable. The right optic disc was small and pale temporally with two small lacunae inferior to the disc, suggestive of colobomas. The maculae appeared hypoplastic. DISCUSSION Our cohort of patients demonstrated karyotypes and features indicative of the 11q deletion syndrome. Growth retardation (3/4), mental retardation (4/4), craniosynostosis (4/4), abnormal facies (4/4), thrombocytopenia/pancytopenia (4/4), congenital heart malformations (1/4), and hand/foot skeletal dysplasia (2/4) were some of the more common characteristics that were present. Our cases also demonstrated some of the typical ocular findings that have been mentioned in previous reports along with some novel findings. Two of the cases that we investigated were the result of translocations. In addition to the deletion of chromosome 11, Case 1 had a trisomy of 9p24.1ter and Case 4 a trisomy of 5q35.3ter. Although these cases matched the Jacobsen phenotype, there is still the possibility that some of the features may have been caused by the trisomy. There is some overlap between Jacobsen syndrome and trisomy 9p or 5q, but there was only one feature found in our cases that can be best explained by the trisomic region. Atrial septal defect (Case 1) has not been strongly associated with Jacobsen syndrome. However, its incidence is increased with 9p duplication.19 Oculofacial Oculofacial abnormalities, including hypertelorism, epicanthus, upward or downward slanting palpebral fissures, and ptosis, are some of the more common features seen in Jacobsen syndrome.2,14,20,21 Hypertelorism/telecanthus was observed by clinical inspection in 3/4 of our cases. Only one of these was confirmed using the Mustardé index measurements. In the literature, hypertelorism has been associated with many different chromosome 11 interstitial deletions and terminal deletions.3,8,9,11,12,22 Perhaps there may be more than one gene on 11q that affects interpupillary and intercanthal distance. Hypertelorism may be a finding that is secondary to another gene(s) on 11q that affects craniofacial development. Epicanthus is reported in up to 50% of the Jacobsen syndrome cases.20,22 This was seen in 1/4 of our cases. Abnormally slanted palpebral fissures were observed in 3/4 of our cases. Upward or downward slanted palpebral fissures, which are common in various genetic syndromes, appear to be present in over half of the Jacobsen cases.20−22 Typically reported in about 50% of the Jacobsen syndrome cases,6,20,22 ptosis was seen in 1/4 of our patients. Our patient had bilateral ptosis, but both bilateral and unilateral cases have been documented without association to a specific breakpoint.7,11,13,23 It is seen with breakpoints as proximal as 11q22 and as distal as 11q25, suggesting a possible candidate region near the end of the chromosome. Krasner et al.24 proposed BARX2 (MIM #604823) as a potential candidate gene for craniofacial abnormalities in Jacobsen syndrome, as it is located in 11q25. This gene is believed to be involved in craniofacial development and has also been shown to have high expression in pockets around the developing eye. BARX2 is not, however, disrupted in Jacobsen cases with interstitial deletions proximal to 11q25 although the craniofacial abnormalities associated with Jacobsen syndrome are still present.9,10 In addition, terminal deletions distal to 11q24.1 show abnormalities significantly different from the classical Jacobsen phenotype.3,7,9 These distal deletions have not been associated with trigonocephaly, flat nasal bridge, anteverted nares, low-set ears, or hypertelorism. THE OCULAR MANIFESTATIONS OF JACOBSEN SYNDROME Strabismus, Amblyopia, and Nystagmus Strabismus, reported in up to 67% of literature cases,6,20,22 was noted in all of our cases. Each of our patients had exotropia. Only Case 1 required intervention. This child also developed strabismic amblyopia, which was treated successfully with occlusion therapy. Upon reviewing the literature, only five other cases of amblyopia with Jacobsen syndrome have been found.6,15 However, given the high incidence of strabismus, this would certainly be likely to occur as a secondary phenomenon. In other reports,2,3,13,25 strabismus has been seen in terminal deletions with breakpoints in regions ranging from q23 to q25, but we are not aware of any candidate genes in this region which might offer a pathophysiology. It is also possible that the strabismus is secondary to the craniofacial developmental abnormalities. We noted nystagmus in 2/4 of our cases. Both cases (2 and 3) showed a breakpoint at 11q23 and their nystagmus resolved spontaneously. To our knowledge, nystagmus has been reported only once previously, with a terminal deletion at 11q24.2 To our knowledge, the incidental finding of anomalous extraocular muscles, as seen in Case 1, has not been previously reported in the literature. However, the preponderance of exotropia in our patients and the lateral rectus anomalies seen at surgery in the absence of other muscle abnormalities on MRI scanning raises the possibility that the lateral recti are uniquely abnormal in Jacobsen syndrome. Anterior Segment Anterior segment abnormalities have not typically been associated with Jacobsen syndrome. Rare cases of cataract and glaucoma have been described,2,20,26,27 although neither was seen in any of our cases. The breakpoint regions in these rare cases were similar to those in our patients and in others from the literature that did not show glaucoma or cataracts, suggesting a coincidental occurrence. We did observe mild microcornea in two patients, with one of them (Case 3) also having clinically insignificant shallow anterior chambers. Lee and colleagues reported astigmatism to be a common refractive error in their case series.15 Two of our cases demonstrated astigmatism. Retinal Abnormalities Retinal changes, including coloboma and retinal dysplasia, are some of the less commonly reported abnormalities in patients with Jacobsen syndrome. In our cases, abnormal retinal findings were found when the deletion involved 11q23 (Cases 24). Case 1, with a terminal deletion breakpoint at 11q24.2, had no retinal findings. Funduscopic abnormalities observed included transient cherry red spots with spontaneously improving visual function (Case 2), nonspecific granular appearance of the RPE (Case 3), coloboma (Case 4), and macular hypoplasia (Case 4). The resolution of the cherry red spot and the macular underdevelopment suggest a delay in retinal development with an overall favorable prognosis. We are unsure about an explanation 5 for the transient cherry red spot seen in Case 2. There is no reason to believe that this child had ganglion cell deposition or problems with arterial perfusion. Perhaps the observed findings represent an unusual abnormality in retinal development that later resolved. Other reports of retinal findings in Jacobsen syndrome also consistently show an association with deletion of 11q23, suggesting a possible region for candidate genes. Cases where 11q23 is intact due to more distal terminal deletions9,28 or to more proximal interstitial deletions10 have not been associated with any fundus abnormalities. Ono and colleagues have shown retinal findings with interstitial deletions ending at 23.1 and 23.2. Our cases and an individual who presented funduscopically like familial exudative vitreoretinopathy, described by Uto and colleagues,22 have shown terminal deletions beginning at 23.3. The fact that these interstitial and terminal deletions do not overlap may indicate that more than one gene in the vicinity could lead to the retinal abnormalities. The recently cloned human ATP-binding cassette gene, ABCG4 (MIM 607784), has been mapped to 11q23.3.29 Although the specific function of this presumed transporter is not fully known, homologues in Drosophila melanogaster are believed to transport retinal pigment precursors or metabolites.30 Oldfield and colleagues have demonstrated that expression is confined to the brain and neural retina.31 Perhaps this gene may also play a role in the developmental delay seen in Jacobsen syndrome. A candidate gene found at 11q23.3 that may also contribute to retinal development is Mfrp (MIM 606227). This frizzledrelated protein is expressed mainly in the lower brain, RPE, and ciliary epithelium of the eye.33 It is believed to facilitate the binding and signaling of Wnt, which is also expressed in the RPE.33 Wnt is important to processes such as cell polarity, cell adhesion, and cell proliferation during embryogenesis. Pivnick and colleagues suggested that NCAM (MIM #116930) may also be an important retinal candidate gene.14 It maps to 11q23.1 and plays an important role in neural cell adhesion, particularly during the embryonic period. In chick embryos, expression has been found in the neural retina, but not in the pigmented retinal epithelium.34 Recently, however, Syrrou and Fryns reported a normal ophthalmic examination in a case with interstitial deletion 11q22.3–11q23.2, the same region containing the NCAM gene.7,35 We believe that the lacunae seen inferior to the right optic disc in Case 4 represent colobomas. Other literature cases involving terminal deletions beginning at 11q22-23 have been associated with unilateral or bilateral coloboms.6,11,12,20,32,36 However, most reported cases of 11q23 deletion do not present with coloboma. Of our three cases of 11q23ter deletion, coloboma was seen in only one (Case 4). Other reports of coloboma have deletions that do not share any common region. For example, one reported case of coloboma had interstitial deletion 11q21.123.1,14 while another had deletion 11q23.3-ter.14 6 G. L. MILLER ET AL. CONCLUSIONS It was not possible to make strong correlations between breakpoints and phenotypes with our cases. In fact, this has been the problem for many scientists studying this syndrome. Because presentations often vary even when breakpoints are in the same sub-bands, it is believed that deletions occur at slightly different locations disrupting different genes.5,14,35 This suggests a high concentration of genes in areas such as 11q23.3. We have reported a variety of ocular abnormalities, both novel and previously recognized, in Jacobsen syndrome. Patients with this syndrome should have complete ocular examinations. Should strabismus be present, it may be prudent to observe for some time as spontaneous resolution does occur. If surgery is indicated, one should be aware of the possibility of anomalous muscle anatomy. Visual prognosis may be affected by such findings as retinal abnormalities, coloboma, or amblyopia. Continued follow-up is indicated. The overall ocular prognosis in these patients, however, is good. Further genotype-phenotype correlation studies may be helpful in identifying candidate genes for ocular disorders, particularly in the 11q23 region. ACKNOWLEDGMENTS The authors would like to acknowledge the invaluable contributions of our Research Assistant, Enza Perruzza. Presented in part at The American Society of Human Genetics 1995 and the International Society of Genetic Eye Disease 1995. REFERENCES 1. Jacobsen P, Hauge M, Henningsen K, Hobolth N, Mikkelsen M, Philip J. An (11;21) translocation in four generations with chromosome 11 abnormalities in the offspring. Hum Hered. 1973;2:568585. 2. Leegte B, Kerstjens-Frederikse WS, Deelstra K, Bergeer JH, Van Essen AJ. 11q- syndrome: three cases and a review of the literature. Genet Couns. 1999; 10(3):305-313. 3. Penny LA, Dell’Aquila M, Jones MC, et al. Clinical and molecular characterization of patients with distal 11q deletions. Am J Hum Genet. 1995;56:676-683. 4. Jones C, Slijepcevic P, Marsh S, Baker E, Langdon WY, Richards RI, Tunnacliffe A. Physical linkage of the fragile site FRA11B and a Jacobsen syndrome chromosome deletion breakpoint in 11q23.3. Hum Mol Genet. 1994;3:2123-2130. 5. Tunnacliffe A, Jones C, Paslier DL, et al. Localization of Jacobsen syndrome breakpoints on a 40-mb physical map of distal chromosome 11q [letter]. Genome Res. 1999;9:44-52. 6. Grossfeld PA, Mattina T, Lai Z, Favier R, Jones KL, Cotter F, Jones C, 11q Consortium. The 11q terminal deletion disorder: a prospective study of 110 cases. Am J Med Genet. 2004;129A:5161. 7. Fryns JP, Kleczkowska A, Buttiens M, Marrin P, Van Den Berghe H. Distal 11q monosomy. The typical 11q monosomy syndrome is due to deletion of subband 11q24.1. Clin Genet. 1986;30:225-260. 8. O’Hare AE, Grace E, Edmunds AT. Deletion of the long arm of chromosome 11[46,XX,del(11)(q24.1-qter)]. Clin Genet. 1984;25:373-377. 9. Ono J, Hasegawa T, Sugama S, Sagehashi N, Hase Y, Oku K, Endo Y, Ohdo S, Ishikiriyama S, Tsukamoto H, Okada S. Partial deletion of the long arm of chromosome 11: ten Japanese children. Clin Genet. 1996;50:474-478. 10. Wakozano A, Masuno M, Yamaguchi S, et al. Interstitial deletion of the long arm of chromosome 11: report of a case and review of the literature. Jpn J Hum Genet. 1992;37:229-234. 11. Linarelli LG, Pai KG, Pan SF, Rubin HM. Anomalies associated with partial deletion of the long arm of chromosome 11. J Pediatr. 1975;86:750-752. 12. Ferry AP, Marchevsky A, Strauss L. Ocular abnormalities in deletion of the long arm of chromosome 11. Ann Ophthalmol. 1981;13:1373-1377. 13. Schinzel A, Auf der Mauer P, Moser H. Partial deletion of chromosome 11[del(11)(q23)]: Jacobsen syndrome. Two cases and review of clinical findings. J Med Genet. 1977;14:438-444. 14. Pivnick EK, Velagaleti GVN, Wilroy RS, et al. Jacobsen syndrome: report of a patient with severe eye anomalies, growth hormone deficiency, and hypothyroidism associated with deletion 11 (q23q25) and review of 52 cases. J Med Genet. 1996;33:772-778. 15. Lee WB, O’Halloran HS, Grossfeld PD, et al. Ocular findings in Jacobsen syndrome. J AAPOS. 2004;8:141-145. 16. Marmor MF, Zrenner E. Standard for clinical electroretinography (1994 update). Doc Ophthalmol. 1995;89:199-210. 17. Westall CA, Panton CM, Levin AV. Time courses for maturation of ERG response types from infancy to adulthood. Doc Ophthalmol. 1999;96:355-379. 18. Mustarde J. Epicanthal folds and the problem of telecanthus. Trans Ophthalmol Soc UK. 1963;83:397-411. 19. Roskes EJ, Boughman JA, Schwartz S, Cohen MM. Congenital cardiovascular malformations (CCVM) and structural chromosome abnormalities: a report of 9 cases and literature review. Clin Genet. 1990;38:198-210. 20. Obregon M, Mingarelli R, Digilio M, Zelante L, Giannotti A, Sagatino G, Dallapiccola B. Deletion 11q23-qter (Jacobsen syndrome): report of three new patients. Ann Genet. 1992;35:208-212. 21. Lewanda AF, Morsey S, Reid CS, Jabs EW. Two craniosynostotic patients with 11q deletions, and review of 48 cases. Am J Med Genet. 1995;59:193-198. 22. Uto H, Shigeto M, Tanaka H, Uchida H, Ohnishi Y, Nishimura M. A case of 11q- syndrome with abnormalities of the retinal vessels. Ophthalmologica. 1994;208:233-236. 23. Frank J, Riccardi VM. The 11q- syndrome. Hum Genet. 1977;35:241-246. 24. Krasner A, Wallace L, Thiagalingam A, Jones C, et al. Cloning and chromosomal localization of the human BARX2 homeobox protein gene. Gene. 2000;250:171-180. 25. Meyer DR, Selkin RP. Ophthalmic manifestations of the chromosome 11q deletion syndrome. Am J Ophthalmol. 1993;115:673674. 26. Ishida Y, Watanabe N, Ishihara Y, Matsuda H. The 11q- syndrome with mosaic partial deletion of 11q. Acta Paediatr Jpn. 1992;34:592-596. 27. Puvabanditsin S, Garrow E, Zia-Ullah MO, Supavekin S, Lianthanasarn P, Denev KI. Monosomy 11q: report of new phenotypic manifestations. Genet Couns. 2001;12:283-286. 28. Cousineau A, Higgins J, Scott-Emaukpor A, Mody G. Ring-11 chromosome: phenotype-karyotype correlation with deletions of 11q. Am J Med Genet. 1983;14:29-35. THE OCULAR MANIFESTATIONS OF JACOBSEN SYNDROME 29. Annilo T, Tammur J, Hutchinson A, Rzhetsky A, Dean M, Allikmets R. Human and mouse orthologs of a new ATP-binding cassette gene, ABCG4. Cytogenet Cell Genet. 2001;94:196-201. 30. Mackenzie SM, Howells AJ, Cox GB, Ewart GD. Sub-cellular localisation of the white/scarlet ABC transporter to pigment granule membranes within the compound eye of Drosophila melanogaster. Genetica. 2000;108:239-252. 31. Oldfield S, Lowry CA, Ruddick J, Lightman SL. ABCG4: a novel human white family ABC-transporter expressed in the brain and eye. Biochim Biophys Acta. 2002;1591:175-179. 32. Felding I, Mitelman F. Deletion of the long arm of chromosome 11. A clinical entity. Acta Paediatr Scand. 1979;68:635-639. 7 33. Kameya S, Hawes NL, Chang B, Heckenlively JR, Naggert JK, Nishina PM. Mfrp, a gene encoding a frizzled related protein, is mutated in the mouse retinal degeneration 6. Hum Mol Genet. 2002;11:1879-1886. 34. Opas M, Davies J R, Zhou Y, Dziak E. Formation of retinal pigment epithelium in vitro by transdifferentiation of neural retina cells. Int J Dev Biol. 2001;45:633-642. 35. Syrrou M, Fryns JP. Interstitial deletion of chromosome 11 (q22.3q23.2) in a boy with mild developmental delay. J Med Genet. 2001;38:621-624. 36. Kaffe SA, Yeatman GW, Riccardi VM. Partial deletion of long arm of chromosome 11: del (11)(q23). Clin Genet. 1977;12:323-328.