Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
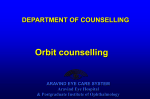
Grand Rounds Conference Eric Downing MD University of Louisville Department of Ophthalmology and Visual Sciences Subjective CC/HPI: 31F presents with right eye pain, upper lid edema/tenderness and copious discharge OD x 2 days. She has mild/moderate pain with EOM, but no diplopia. She denies any vision changes, fever, or congestion. History POH: none PMH: none Eye Meds: none Meds/Allergies: none, NKDA Social Hx: no pets, no travel Objective VA: Pupils: IOP: EOM: OD 20/25 5->2 21 full OU OS 20/20 5->2, no rAPD 18 Objective PLE: E/L/L: C/S K AC I/L Vit DFE: all WNL OU OD ST erythema/edema 1+ injection, mild temporal chemosis Clear D&Q WNL WNL Clinical photos Clinical photos Assessment 31F with moderate/severe unilateral superotemporal orbital pain x 2 days with copious watery discharge. CT scan showing inflammation/hyperintensity of the right lacrimal gland Dx: Acute Dacryoadenitis Laboratory CBC: 14.1 12.8 318 43.0 BMP: WNL ESR/CRP: 7/9.4 EBV: IgG positive, IgM positive Laboratory CBC: 14.1 12.8 318 43.0 9 BMP: WNL ESR/CRP: 7/9.4 EBV: IgG positive, IgM positive Treatment One dose IV Vanc and Ceftriaxone in ED Sent home on po Keflex x 5 days Warm compresses PRN Background Self-limited condition Inflammatory enlargement of the lacrimal gland Pathophysiology poorly understood but thought to be due to ascension from the conjunctiva 1/10K ophtho patients Acute & Chronic forms Forms of Dacryoadenitis Acute Unilateral severe pain, redness, and pressure in ST quadrant Rapid onset Chronic Unilateral or bilateral Painless enlargement of lacrimal gland > 1 month More common Etiology Infectious Viral: Mumps, Epstein-Barr Virus, HZV, Mononucleosis Bacterial: Staph aureus, N. gonorrhoeae, Syphilis, Chlamydia, TB Inflammatory Sarcoidosis, Grave’s Dz, Sjögren’s, IgG-4 related disease, benign lymphoproliferative lesions Exam Gland is often prolapsed, enlarged, and tender Chemosis Injection Mucopurulent discharge Eyelid edema/erythema Submandibular adenopathy Mild ophthalmoplegia Treatment Viral: supportive measures (e.g. warm compresses, oral NSAIDs) Bacterial: oral Cephalosporin such as Keflex Inflammatory: treat underlying disease Consider biopsy if refractory to treatment of underlying disease Research Retrospective case series 8 patients with IgG-4 related disease of salivary and lacrimal glands Performed EBV FISH analysis on biopsied tissues Found a positive correlation between IgG-4 concentrations and EBV load EBV viral load may have prognostic value in these pts References 1. 2. 3. 4. Kanski JJ. Acute dacryoadenitis. Clinical Ophthalmology: A Systemic Approach 6th edition. Butterworth, Heineman, Elsevier; 2014: 178-179. BCSC 7 Orbit, Eyelids, and Lacrimal System:2014. pp 273-274 Rhem MN, Wilhelmus KR, Jones DB. Epstein-barr virus dacryoadenitis. AM J Ophthlmol 2000;129:372-5 Boruchoff SA, Boruchoff SE. Infections of the lacrimal system. Infect Dis Clin North Am. Dec 1992;6(4):925-32.