Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
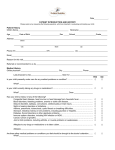
Dental Clinic for Children and Adults Na Rybníčku 1364/12, 120 00 Prague 2 - Nové Město Tel./fax: +420 224 941 597, Mobile: +420 602 814 818 E-mail: [email protected] Patient information Title, surname and first name:...................................................................................................................................... Address:………………………………………………………………………………………………………………………….. Birth certificate no.:……………………………... Insurance company:………………………………………..... Telephone (mobile, work, home):…………………………………………………………………………........... E-mail: ……………………………………………. Contact person, in case of a need to leave a message (doctor's unavailability, change in the date of the visit): ........................................................................ Telephone: …………………………………………… State of health: 1. Have you incurred any serious disease or head injury in the past: YES – NO If your answer is yes, please specify which..…………………………………………………............................... 2. Are you currently undergoing a long-term treatment of some of these diseases? High blood pressure YES NO YES NO Heart disease and arrhythmia (irregular heartbeat) Asthma Thyroid disease Blood coagulation disorders Hematopoietic disorders and diseases of the blood Immune system disorders Liver diseases Kidney diseases Diabetes If your answer is yes, please specify the method of treatment Heavy rheumatism Hepatitis (A, B, C ...) or any other serious infectious diseases (tuberculosis, HIV) suffered in the past Seizure disorders (e.g. epilepsy) 1. Treatment by diet 2. Treatment by medication (peroral antidiabetics) 3. Treatment by insulin YES YES YES YES YES YES YES YES YES YES NO NO NO NO NO NO NO NO NO NO YES YES YES NO NO NO YES NO 3. Do you take any long-term medication? YES – NO If your answer is yes, please specify which medication and in what dosage ……………………………………………………………………............................................................................ 4. Do you experience any manifestations of allergies? YES – NO If your answer is yes, please specify which..…………………........................................................................... If you suffer from any allergies to medications, please specify which medication you are allergic to: .......................................................................................................................................................................... 5. (For women only) Are you pregnant YES- NO 6. Do you suffer from gnashing of teeth in your sleep? YES – NO – I DO NOT KNOW 7. How many times a day do you brush your teeth? ........................................ 8. How often do you visit the dentist? ............................................................... 9. Have you undergone orthodontic (braces) or periodontal (name of the doctor) treatment? ……………………………………………………………………………………………………………………………………. 10. Do you smoke? YES – NO How many cigarettes a day?….…………………………….. 11. How did you get to know about us or who recommended us to you? ……………………………………………………………………………………………………………………………………. I declare that I have been acquainted with the price list of above-standard dental care of dental clinic Radno spol. s.r.o. Date:………………………. Signature of the patient:….…………………………………...... Thank you for your time spent completing this questionnaire. The data you provided to us will be considered strictly confidential and will only be used to adjust the treatment to your state of health.