Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CUN. CHEM. 25/8, 1394-1398(1979)
Inter- and Intra-IndividualVariations in the Saliva/Blood Alcohol
Ratio During Ethanol Metabolism in Man
A. W. Jones
The inter- and intra-individual components of variation in
the saliva/blood alcohol ratio have been calculated from
experiments with 48 male subjects after they drank 0.72
g of ethanol per kilogram of body weight as neat whisky
after a short fast. Saliva and blood ethanol profiles were
monitored at 30-60 mm intervals for up to 7 h after intake.
The analytical component of variation inherent in an estimate of the saliva/blood alcohol ratio, expressed as
coefficient of variation, was 1.75%. I calculated saliva/
blood ethanol ratios for each subject at each sampling time
by taking the antilogarithm of the difference (log saliva
alcohol - log blood alcohol). The mean ratio between 60
and 360 mm after drinking was 1.077 (n = 336) with 95%
confidence limits of 1.065 and 1.088. Moreover, the individual ratios showed no systematic variation throughout
the absorption, distribution, and elimination phases of
ethanol metabolism. Using a two-way analysis of variance
and allowing for analytical sources of variation, I determined that the inter- and intra-subject variance components were 53 and 47% of the total biological variation.
The saliva/blood alcohol ratio during ethanol metabolism,
determined once in a single individual, had a biologically
derived coefficient of variation of 10%.
reinvestigation
AddItional Keyphrase:
experiments
in evaluating
ratio
alcohol ratio (8). The re-
blood-alcohol concentrations (5) and show that the saliva!
blood alcohol ratio is remarkably constant throughout the
entire ethanol biotransformation
(8).
At the present time there is increasing
emphasis
on saliva
as a biological specimen for drug monitoring (9, 10). The nuof saliva over blood or plasma samples for
this purpose have been pointed out in a recent review article
merous advantages
(11). If saliva-ethanol
determinations
are to be of value for
estimating
blood-alcohol
concentration,
then the observed
saliva/blood
alcohol ratios should be concentration-inde-
pendent, with a low inter- and intrasubject variation.
I report the results from a controlled study to determine the
biological variations inherent in the saliva/blood alcohol ratio
when capillary blood and a mixed salivary secretion are the
assay materials. The relationship
has been followed over the
entire blood-alcohol time course, representing
absorption,
distribution,
and elimination
phases of ethanol metabolism
in man.
Material and Methods
Subjects
and Conditions
Forty-eight
log differences
of the saliva/blood
sults confirm a high correlation between saliva-alcohol and
apparently healthy male subjects served in the
after
fasting
overnight.
They
consumed,
per
kilogram of body weight, 0.72 g of ethanol as neat whisky
variables
within 20 mm. Triplicate capillary-blood samples and an
biological fluids and hence on calculation of the
unstimulated
mixed saliva secretion were taken concurrently
at 30-60 mm intervals for up to 7 h. Blood and saliva ethanol
concentrations
were determined with an automated enzymatic
blood-body-fluid alcohol ratios (1,2). The relationships found
method involving alcohol dehydrogenase (EC 1.1.1.1). Full
have been often used to estimate the blood-alcohol concentration from analysis of a more accessible biological material.
details
In experiments
concerned with the fate of alcohol in the
body, many studies have focused on ethanol determination
in different
In this context,
determinations
of alcohol in urine and expired
breath have found wide application
in medicolegal work
concerning
of alcohol. The urine
driving
under the influence
or breath specimens serve as substitutes for blood, and the
analytical
finding
is usually
translated
into the presumably
equivalent blood-alcohol concentration (3,4). The distribution
of ethanol between saliva and blood, i.e., the saliva/blood alcohol relationship,
does not appear to have been extensively
studied in this connection. In the past, analytical methods for
ethanol determination
in saliva were hampered by technical
difficulties.
The methods earlier reported involved chemical
oxidation procedures requiring relatively large sample volumes, which were often impractical to collect from intoxicated
subjects
(5, 6).
The recent introduction of a micromethod for ethanol determination in saliva samples (7) has enabled a detailed
of the test subjects;
1394 CLINICAL CHEMISTRY, Vol. 25, No. 8, 1979
storage, and treat-
end of drinking, were for some subjects abnormally
high because of a high concentration
of alcohol present in the oral
mucosa from the recent drinking session. At 420 mm from the
start of drinking, the alcohol dose (0.72 g/kg) had been completely metabolized in some individuals, and the saliva/blood
alcohol ratio at this time point was therefore indeterminable.
For these reasons, only the samples taken between 60 and 360
mm from the start of drinking
were used in the statistical
analysis.
Analytical Variance Component
Blood Alcohol Ratio
All ethanol determinations
experienced
blood and
Department
of Alcohol and Drug Addiction
Research, Karolinska
Institutet,
10401 Stockholm,
Sweden.
Received Feb. 23, 1979; accepted May 16, 1979.
the sampling,
ment of biological samples; and the method of analysis have
been recently reported (7, 8).
The saliva/blood alcohol ratios calculated for samples taken
at 30 mm from the start of drinking, i.e., just 10 mm from the
analyst
in the Saliva/
were performed by the same
in a total of 16 runs. Concurrently
taken
saliva samples from each subject were always analyzed within the same run. A new absorbance/concentration
relationship for standards of known strength was used to
calculate unknowns in each run. On this basis, minor varia-
2
‘-
eose
E*p.
1.0
-1
4
0.72gkg
Exp. 7859
EKp. 7930
0.72 g kj1
0.72 g
I.’.
0
12
1.0
>
S
0.8
I’,
0
I’
I’
E 1.00
E
-
I\\
_p_.
Z.-.#{149}.#{176}’
Saliva
-J
0
3:
0
U
-J
.4
‘/
ii
030
I
Blood
0
60
120
180
240
300
360
420
0
#{149}
60
S
iSO
-S
0
-S
-
-e
300
-S.
420
0
60
180
300
420
2012
TIME FROM START OF DRINKING (minI
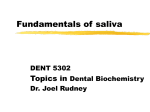
Fig. 1. Above, variations in the saliva/blood
alcohol ratio during ethanol metabolism; Below, the time course of ethanol metabolism
in three subjects after consuming ethanol (0.72 g/kg body weight) as neat whisky on a fasting stomach
tions in operating conditions betweenruns(e..g.,temperatures,
reagent
concentrations,
etc.) affect standards
and unknowns
equally and thus should not drastically influence analytical
precision between runs. Within-run precision was calculated
from the pooled variances of the duplicate or triplicate saliva
and blood ethanol determinations.
The variances within
each
of the 16 runs were not significantly different, as shown by
Bartlett’s test (12): chi-square (df = 15) was not significant
(p > 0.05).
Standard deviations of single determinations of ethanol in
samples of saliva and blood increased in relation to the ethanol
concentration, whereas the coefficients of variation
or less constant. This suggested that the standard
expressed in logs would be approximately constant.
ethanol concentration of 510mg/L, these standard
were more
deviations
At a mean
deviations
were 8 mg/L for saliva (7) and 12mg/L for blood (13). Calculation of a saliva/blood alcohol ratio was based on the mean
of a duplicate saliva-alcohol determination and the mean of
a triplicate
blood-alcohol
determination.
The experimental
errors of these means are, respectively, 1/v’ and 1/v’ times
the standard deviations of single determinations
in saliva and
blood. An estimate of the analytical error inherent in a saliva/blood alcohol ratio was calculated from the square, sum,
and square root of the individual standard errors when expressed
V1.1072
as coefficients
of variation
(14). This
was
+ 1.3582 = 1.75%, implying a low analytical error.
and fixed effects for an added variance component for which
the error mean square is the denominator, one must assume
that interaction between sampling time and the individual is
zero; otherwise, only the fixed effects can be justifiably tested.
Evidence that the interaction is in fact negligible was obtained
from a covariance analysis (vide infra) in which the regression
of the saliva/blood ethanol ratio for each individual was shown
to be parallel through time. Regression equations were computed by the method of least squares, and regression lines were
compared by analysis of covariance (16). To convert a standard deviation (SD) expressed in log units to the corresponding relative SD or coefficient of variation, I used an
approximation given by Bliss (17), i.e., relative SD% = 230.26
X log SD. This method is accurate when variability
is less than
20%, as for the data evaluated
in this paper.
Results
Variation in Saliva/Blood
Ethanol Metabolism
Alcohol Ratios during
The saliva and blood alcohol time course during the entire
ethanol biotransformation
is shown in the lower part of Figure
1 for three individuals
who are representative
of the whole
group. These curves show a typical course for the drinking
error of the mean
conditions
in these experiments.
Note that saliva-alcohol
profiles follow the corresponding blood-alcohol profiles during
the absorption, distribution,
and elimination phases of ethanol
metabolism
(18).
Variations in the saliva/blood alcohol ratios are illustrated
in the upper part of Figure 1. No systematic variations
are
evident throughout
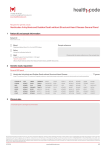
the sampling period. This is further illustrated in Figure 2, where the mean curve for 48 subjects is
shown. A statistical
analysis of the results is presented in
difference, thus overcoming the difficulties in estimating the
variance of a ratio computed directly (14). Variability between
and within individuals was determined by analysis of variance
Table 1. The consistency of the mean saliva/blood alcohol
ratios is striking and was confirmed by one-way ANOVA (F =
0.964, df = 6 and 329, p > 0.05). Confidence limits (95%) on
Statistical
Analysis
Because ratio variables tend to be skewed to the right and
highly peaked (leptokurtic)
(15), the calculation of saliva!
blood alcohol ratios in this work was based on log differences.
This technique offers the advantage that confidence limits
may be obtained
(AN0vA),
with
directly
from the standard
the log differences
as variates.
In the model
used, the subjects serve as random effects, and the time-to-
time variation
are the fixed effects. To test both the random
the mean saliva/blood
alcohol
ratios
at different
sampling
times and also for a new single observation are given in Table
1. These latter confidence limits provide the range of values
CLINICAL CHEMISTRY, Vol. 25, No. 8, 1979
1395
MEAN SALIVA! BLOOD ALCOHOL RATIOS
meant 95/.
confidence
limits
E
01
121-
E
1.0
I
101-
o-J
I
I
I
o
0
C.)
-J
.4
081MEAN ALCOHOL TIME COURSE
1.0
-J
.4
U)
F
-j
0l
F
C)
z
meoneSD(n48)
05
.0
C.)
0
0
I
0
0
1.0
0.5
1.5
BLOOD ALCOHOL. mg/mi
120
240
360
480
TIME FROM START OF DRINI<ING, mint.
Fig. 2. Above,
variations
alcohol ratios
for 48 subjects during ethanol metabolism; below, mean blood
and saliva alcohol profiles in the same subjects treated as in Fig.
1
gestion
in mean saliva/blood
within which 95 out of 100 single determinations
of the saliva/blood alcohol ratio would be expected to fall, given randomly selected subjects from the same population.
Variations in the Saliva/Blood
Different Subjects over Time
Alcohol
Ratio among
For each subject, the relationship
between saliva/blood
alcohol ratio and sampling time was determined by regression
analysis; the 48 individual regression lines were compared by
analysis of covariance. The slopes of the individual regression
lines (regression
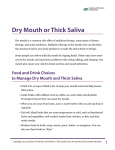
Fig. 3. Correlation between blood and saliva alcohol in concurrent samples taken between 60 and 360 mm after alcohol in-
coefficients),
which represented
the change
in saliva/blood ratio through time, were not significantly
different from zero. Furthermore, there were no statistically
significant differences between the slopes of regression lines
for the different subjects (F = 1.314, df = 47 and 240, p >
0.05), implying that there were parallel trends through time,
with no interaction between sampling time and the saliva!
blood ratio for different subjects.
Correlation between
Concentrations
The relationship
Saliva and Blood Alcohol
between saliva alcohol (y), g/L, and blood
alcohol (x), g/L, in the concurrent samples has been determined by regression analysis. A scatter diagram of this relais shown in Figure 3. The regression equation was y
0.003 + 1.075x (r = 0.962 ± 0.0148, p <0.001), and theyintercept
(0.003 ± 0.0102) was not significantly
different from
zero (t = 0.296, df = 334, p > 0.05). The regression line thus
tionship
=
passes through the origin, indicating that the saliva-alcohol
concentration
is zero when blood alcohol reaches zero, there
being no time-lag apparent. The standard error estimate (S)
was 64.2 mg!L, on the average, and increased with an increase
in blood-alcohol concentration;
i.e., the residual SD’s were not
constant (Figure 3). Therefore, the mean saliva/blood alcohol
ratio for all the data was calculated as the antilogarithm
[sum
(log saliva alcohol - log blood alcohol)!n], where n = number
of saliva-blood
pairs. The resulting ratio was 1.077 with 95%
confidence limits of 1.065 and 1.088.
Inter- and lntra-lndividual
Blood Alcohol Ratio
To separate
Variations
the components
in the Saliva/
of variance
attributable
to
was carried
The elevations of the different regression lines representing
the differences between adjusted means were, however, significantly different (F = 9.308, df = 47 and 287, p <0.001),
biological
sources of variation,
a two-way
ANOVA
out. Based on the ANOVA (Table 2), a significant
added vari-
indicating that the mean saliva/blood alcohol ratios differed
ance component was found between subjects (F
=
for different
subjects.
Table 1. Mean Saliva/Blood Alcohol Ratios and
95% Confidence Limits after Intake of Ethanola
Sampling
time, mln
Mean
ratio
95% confIdence limlis
Mean
New observation0
60
90
1.08
1.09
1.05-1.10
1.06-1.11
0.92-1.27
0.90-1.31
120
1.09
1.05-1.12
0.88-1.35
180
240
300
360
1.06
1.05
1.09
1.09
1.02-1.09
1.02-1.09
1.05-1. 12
1.06- 1. 12
0.85-1.31
0.84-1.32
0.87-1.36
0.90-1.32
ethanol intake = 0.72 g/kg of body weight. Computationsbasedon
the mean and variance of the difference (log saliva-alcohol - log blood-alcohol)
at each sampling time. Confidence limits are not symmetrical about the mean
=
48;
value in all cases when transformed from logs to absolute values.
b Separate new single determination estimated for the population.
1396 CLINICAL CHEMISTRY, Vol. 25, No. 8, 1979
9.72, df =
47 and 282, p <0.001).
This confirms the results from the
covariance analysis, in which the differences between adjusted
means, after allowing for regression through time, were statistically significant (p <0.001). The time-to-time variation
Table 2. Two-Way ANOVA Based on Variations in
the Saliva/Blood Alcohol Ratio between Subjects
(n = 48) and Between Sampling Times (n Variance
= 7)
Source of
variation
Subjects (s)
Times(t)
Error (e)
Total
Degrees of
freedom
47
6
Sums of
squares
Mean
squares (MS)
0.3933 1
0.00836
0.01113
0.00185
282
0.24240
0.00086
335
0.64684
ratio (F)
2.15c
Sampleswere taken between 60 and 360 mm after the subjects drank 0.72
g/kg ethanol.Variance component between subjects is given by (MS - MSe)/flt
8
=
0.00107.
bp
<0.001.
Cp
<0.05.
derived from the two-way ANOVA just
(F = 2.15, df = 6 and 282, p <0.05).
approached significance
This technique of statistical analysis is considerably more sensitive than the oneway ANOVA used earlier because the intersubject variation is
now removed from the error variance by the two-way de-
less alcohol than parotid saliva; this would support
the present
finding of a ratio of less than 1.17. In an extensive study by
Coldwell and Smith (5), in which venous blood and stimulated
whole saliva were used, a mean saliva/blood alcohol ratio of
1.12 was reported. In their experiments saliva and blood
samples were taken between 30 and 150 mm after subjects had
sign.
The error mean square, 0.00086, represents the error vari-
ance per observation and corresponds to a relative standard
deviation
(CV) of 6.75% (Table 2). This estimate is a com-
posite of within-subject
subject/time
interaction,
variance, analytical
variance, and
with the latter assumed to be in-
consumed alcohol immediately after a meal. Because the alcohol concentration in venous blood is less than that of capillary blood until onset of the post-absorptive phase of ethanol
metabolism, this may explain, at least in part, the higher ratio
of 1.12 they report, compared with the 1.077 I found.
significant. The within-subject variance has also been estimated in another way, viz., by pooling the variances of the
In a recent paper (23), ethanol in human parotid saliva and
in plasma was determined in five subjects between 15 and 120
seven determinations
on each subject. This result, 0.00088,
corresponds to a CV of 6.83%, with the range for the 48
subjects at 2.3-12.7% of the mean. The 6.83% is only slightly
greater than the error variance based on ANOVA, 6.75%. The
difference is not significant (F = 1.02, df = 288 and 282, p>
mm after they consumed neat whisky (1 mL/kg). The mean
saliva/plasma
ratios at the different
sampling times ranged
0.05), which independently confirms that the interaction effect
is negligible.
The true intra-individual
variation may be found by correcting the error variance (Table 2) for the analytical variance
inherent in the saliva/blood alcohol ratio. The analytical
variance was estimated at 1.75% and the within-subject
variance based on ANOVA at 6.75%; the true within-subject
variance is therefore V’6.752 - 1.752 = 6.51%. In the same way,
the intersubject variance component (Table 2) was found to
be 0.00107, CV = 7.53%, which after allowance for analytical
error reduces to 7.32%.
The biological
variation
in the saliva/blood
alcohol ratio is
derived more from intersubject than intrasubject sources; the
ratio of inter/intra is 7.32/6.51, or 1.12, with the inter- component contributing 53% and the intra- component 47% of the
total. The relative SD of the saliva/blood alcohol ratio determined once in a single subject between 60 and 360 mm after
ethanol intake is V’7.322 + 6.512 = 9.79%, and may be attributed
to biological
variations
In contrast to both the urine/blood and breath/blood alcohol ratios, which vary according to the phase of ethanol
metabolism (19,20), the mean saliva/blood alcohol ratio shows
no such variation. The applicability of saliva as a biological
specimen for ethanol determination
in clinical and medicolegal work should perhaps be reconsidered
in view of this
finding. The saliva samples analyzed throughout
these ex-
periments were of mixed whole saliva ejected directly from
after a few seconds of tongue and lip movements
by the subject. For practical purposes, obtaining a saliva
specimen, although a noninvasive procedure, requires a certain amount of cooperation from the subject, and therefore
mixed resting saliva (as used in these experiments) or perhaps
a stimulated sample (e.g., by having the subject chew Parafilm
before ejection) would seem to be the most appropriate medium for analysis. The relative alcohol concentrations of
mixed
whole
saliva,
parotid
saliva,
and samples
results of saliva-ethanol
determinations,
then a low biological
variation in the saliva/blood relationship is a necessary and
critical factor. At a 1.0 g/L saliva-ethanol concentration, the
corresponding blood-ethanol concentration will be either 850
mg/L or 930 mg/L, based on the theoretical ratio of 1.17 or the
experimentally
observed
ratio of 1.077. Given this small ab-
solute difference in blood-ethanol concentration (80 mg/L),
the pharmacologic effects of ethanol elicited should be indistinguishable. For medicolegal or clinical applications, an
upper confidence limit, depending on the degreeof probability
required, could be used for converting from saliva ethanol to
the estimated blood concentration instead of the mean ratio.
This would ensure that an overestimate of the true bloodethanol concentration would be highly improbable.
This study was supported
by grants to Prof. L. Goldberg
from the
Swedish Medical Research Council and the National Swedish Police
Board (Rikspolisstyrelsen). Jan Buijten and Aldo Neri provided
technical assistance in this study.
in this relationship.
Discussion
the mouth
from 0.95 to 1.13 (overall mean, 1.04), and the coefficients of
variation ranged from 14 to 28%, indicating considerable intersubject variation.
If blood-ethanol concentrations are to be estimated from
from
the
submaxillary or sublingual glands remain to be studied.
The mean saliva/blood ethanol ratio determined in these
experiments
was 1.077, with 95% confidence limits of 1.065 and
1.088. This is lower than that expected on the basis of relative
water contents of blood and saliva specimens. If whole blood
and saliva contain 850 and 994 g of water, respectively, per
liter (21), the theoretical saliva/blood ethanol ratio should be
1.17. The reasons for the lower ratio observed in this study are
not completely clear. Dilution of saliva specimen with mucus
secretions from the oral cavity that perhaps have less water
than saliva, or even evaporation of ethanol during the sampling procedure, may partly account for this observation.
Linde (22) reported that mixed saliva contained about 10%
References
1. Harger, R. N., and Forney, R. B., Aliphatic
alcohols. In Progress
in Chemical Toxicology, 3, A. Stolman, Ed., Academic Press Inc., New
York,
1967, pp 1-61.
2. Dubowski, K. M., Alcohol determination-Some
physiological and
metabolic considerations.
In Alcohol and Traffic Safety, B. H. Fox
and J. H. Fox, Eds., Public Health Service Pub. No. 1043, U.S. Government Printing Office, Washington,
DC, 1963, pp 91-115.
3. Mason, M. F., and Dubowski, K. M., Breath-alcohol
analysis: Uses,
methods and some forensic problems - review and opinion. J. Forensic Sci. 21,9-41(1976).
4. Robinson, A. E., Practical scientific problems associated with
drinking and driving legislation
in England.
In Alcohol, Drugs and
Traffic Safety, proceedings of the 6th International
Conference, S.
Israelstam and S. Lambert, Eds., Addiction Research Foundation,
Toronto,
Canada,
1975, pp 573-578.
5. Coldwell, B. B., and Smith, H. W., Alcohol levels in body fluids
after ingestion of distilled spirits. Can. J. Biochem. Physiol.
37,43-52
(1959).
6. Friedemann, T. E., Motel, W. G., and Necheles, H., The excretion
of ingested ethyl alcohol in saliva. J. Lab. Clin. Med. 23, 1007-1014,
(1938).
7. Jones, A. W., Assessment of an automated enzymatic method for
ethanol determination
in microsamples
of saliva. Scand. J. Clin. Lab.
Invest.
39, 199-203 (1979).
8. Jones, A. W., Distribution of ethanol between saliva and blood in
man. Clin. Exp. Pharmacol. Physiol. 6,53-59 (1979).
9. Horning, M. G., Brown, L., Nowlin, J., et al., Use of saliva in therapeutic drug monitoring.
Clin. Chem. 23, 157-164 (1977).
10. Dvorchik, B. H., and Vesell, E. S., Pharmacokinetic
interpretation
of data gathered during therapeutic drug monitoring. Clin. Chem. 22,
868-878 (1976).
CLINICAL CHEMISTRY, Vol. 25, No. 8, 1979
1397
11. Danhof, M., and Breimer, D. D., Therapeutic drug monitoring
in saliva. Clin. Pharmacokinet.
3, 39-57 (1978).
12. Bartlett, M. S., Properties of sufficiency and statistical tests. &oc.
R. Soc. London
A. 160,268-282(1937).
13. Buijten, J. C., An automatic ultra-micro distillation technique
for determination
of ethanol in blood and urine. Blutalkohol
12,
393-398 (1975).
14. Finney, D. J., Statistical
Methods
in Biological
Assay. Charles
Griffin and Co. Ltd., London, 1952, pp 21-57.
15. Anderson, D. E., and Lydic, R., On the effect of using ratios in the
analysis of variance. Biobehav. Rev. 1, 225-229 (1977).
16. Snedecor, G. W., and Cochran, W. G., Statistical Methods. 6th
ed., Iowa State University Press, Ames, IA, 1967, chap. 6 and 14.
17. Bliss, C. I., Statistics
in Biology, 1, McGraw-Hffl, New York, NY,
1967, pp 137-138.
1398 CLINICAL CHEMISTRY, Vol. 25, No. 8, 1979
18. Wallgren, H., and Barry, H., III, Actions of Alcohol 1, Elsevier
Publishing Co., Amsterdam, 1970, chap. 2.
19. Payne, J. P., Hill, D. W., and King, N. W., Observations on the
distribution of alcohol in blood, breath and urine. Br. Med. J. i,
196-202 (1966).
20. Jones, A. W., Variability of the blood:breath alcohol ratio in-vivo.
J. Stud. Ak. 39, 1931-1939 (1978).
21. Scientific Tables, 7th ed., K. Diem and C. Lentner, Eds., Geigy,
Basle, 1973, p 651 and p 643.
22. Linde, P., Der Ubergang des Athylalkohols in den Parotsspeichel
beim Mensehen. Arch. Exp. Pathol. Pharmakol.
167, 285-291
(1932).
23. Digregorio,
G. J., Piraino, A. J., and Ruch, E., Correlations of
blood ethanol concentrations. Drug Ak. Depen-
parotid saliva and
dence 3,43-50
(1978).