Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
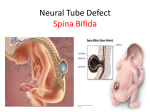
Spina Bifida: Where we have been and where we are now Sandra L. Whisler, MD, MS Visiting Professor of Pediatrics Special Care Clinic Children’s Hospital Colorado Denver, Colorado Pre-Test • 1. What is the most common type of Spina Bifida? • 2. List 2 common causes of death is Spina Bifida patients. • 3. List 2 things that can increase the incidence of Spina Bifida. • 4. List 3 co-morbidities that may be associated with Myelomeningocele (MMC) OBJECTIVES 1. Understand what Spina Bifida is 2. Understand the history of Spina Bifida treatment 3. Understand the comorbidities associated with spina bifida Spina Bifida Definition: • Neural tube defects which are congenital anomalies of neurodevelopment with a spectrum of clinical manifestations. (8) • They include the cranium and/or spine. History • Before 1940s: Most babies with spina bifida died of meningitis before the introduction of antibiotics in the 1940s. (1) • Late 1950s: Shunts were developed and revolutionized the treatment of Spina Bifida by treating hydrocephalus which had been a major cause of morbidity and mortality. (2) • Before 1960: the survival rate for spina bifida was only 10-20% and repairs were postponed until 2 years of age based on the belief that only the strongest would survive. (3) History Continued • 1960s: Urinary diversion techniques were developed which helped preserve urinary continence and allow patients to gain social continence (4) • Mid-1960s: The US and United Kingdom adopted the practice of operating on babies with Spina Bifida within 12-24 hours after birth who did not have other defects incompatible with life. (5) History Continued 1970s: • Shunting was effective, but these shunts needed frequent revisions and the long term effects of impaired renal function lead to renal failure. Renal failure became the leading cause of death for individuals with Spina bifida in the 1970s. (1) • More orthopedic surgeries were needed to facilitate walking, long hospitalizations occurred. These resulted in psychological and educational problems. (6) • A trans-Atlantic debate over whether to treat or not treat spina bifida erupted in the 1970s. This debate helped shape the emerging discipline of bioethics. (7) History Continued • 1984: Most children with Spina bifida were found to achieve independent mobility and social continence (utilizing intermittent catheterization) and most cases of intellectual disability could be prevented by early and aggressive treatment. (6) General Information • Occurs: <1-7/1000 live births (8) • Myelomeningocele (MMC) is the most common form of spina bifida. (9) • Rates of spina bifida has decreased since the Federal Drug Administration mandated folate supplements to enriched grain products in 1998. (10) General Information Continued • Neural tube defects (NTDs) are the 2nd most common congenital anomaly • Girls are more commonly affected than boys • Certain populations with increased risk – – – – – – English/Irish China India Pakistan Egypt Latino populations in the US Neural Tube defects are commonly diagnosed prenatally • Quad screen at 15-20 weeks: MS-AFP elevated • Level II Ultrasound can detect back lesions as well as brain abnormalities • Amniocentesis – AF-AFP, ACHE are both elevated Etiology • MULTIFACTORIAL INHERITANCE – AGE: increases with maternal age – SOCIOECONOMIC: increases with lower income – NUTRITION : folate/homocysteine metabolism, glucose and zinc – HYPERTHERMIA : hot tubs and saunas (temps >102, 2x risk) – MEDICATION: Valproate, Tegretol, alcohol, agent orange – GENETICS: multiple genes are now being studied. Also evidence that the neural tube closes at multiple closure sites (i.e. probably 5 zippers rather than just 2), which are each regulated by different genes and affected by different teratogens Risk Factors • Folic acid deficiency-has been clearly associated with open spinal dysraphism. (8) • Maternal insulin-dependent diabetesassociated with caudal regression or sacral agenesis. (11) • Maternal exposure to certain medicationsvalproate, carbamazepine. (12, 13) Recurrence Risks • 2-3% in future pregnancies • 1-2% for sibs of parents and sibs of patient • Can reduce risks by 50-75% by use of Folate prophylaxis 4 mg/day taken for minimum of 3 months prior to conception and first month of pregnancy Types and Definitions • Syringomyelia: Fluid outside of the central spinal canal. (8) • Hydromyelia: Fluid within the central spinal canal. May be asymptomatic. (14) • Spina bifida occulta: Failure of fusion of the vertebral bodies dorsal to the spinal cord. Overlying skin is intact but have minor overlying abnormalities such as nevi, dimple, dermal sinus, hemangiomas, tuft of hair, or an underlying lipoma. (15) • Spina bifida aperta: meninges and/or spinal cord herniate through a defect in skin. (8) Types and Definitions • Meningocele: only the meninges have herniated through a cleft in the spinal column . (8) • Myelomeningocele (MMC): meninges and spinal cord both herniate through defect in skin. (8) -Almost all patients have a Chiari II malformation and most have hydrocephalus -80% are in the lumbar and sacral regions -97% with bowel and bladder involvement • Tethered cord Syndrome (TCS): caused by attachment of the filum terminale to inelastic structures caudally resulting in stretchinduced dysfunction of the caudal spinal cord and conus. (8) • Sacral agenesis or caudal regression syndrome: spectrum of defects including incomplete development of the sacrum and sometimes of the lumbar vertebrae. It may be associated with spinal dysraphism and is usually associated with a tethered cord. (16) Types and Definitions Continued • Spinal lipomas and teratomas: often contain multiple types of tissues and may impinge on spinal cord later in life and cause progressive neurologic dysfunction. (17) • Terminal Diplomyelia: duplication or splitting of the terminal spinal cord and patients may be asymptomatic. (8) -May see marked asymmetry of involvement of the lower extremities • Spinal dysraphism: failure of fusion of the vertebral bodies. (8) Types and Definitions Continued Types of Spinal Dysraphism (8): • Occult spinal dysraphism: usually abnormalities occur in the overlying skin such as such as nevi, dimple, dermal sinus, hemangiomas, tuft of hair, or an underlying lipoma. • Open spinal dysraphism: spina bifida aperta-cleft in the spinal column with herniation of the meninges (meningocele) or meninges and spinal cord (myelomeningocele) through the defect. • Closed Spinal Dysraphism: spina bifida occultaunexposed neural tissue Myelomeningocele (9) • Myelomeningocele (MMC) is the most common form of spina bifida. • MMC can be diagnosed in the first trimester • Prenatal MMC repair reduces the need for shunting. • With prenatal repairs, improved motor outcomes are seen at 30 months as compared with repair after birth. • In utero repairs have been associated with maternal and fetal risks including preterm delivery, fetal death, and uterine dehiscence. • Improvement in mental development was also noted. MMC General Information (18) • Most newborns have evidence of neurological impairment at birth suggesting that neurological injury occurs during gestation or at delivery. • Evidence that the neurological deficits associated with MMC are not just caused by incomplete neurulation but by prolonged exposure of the vulnerable neural elements to the intrauterine environment. • MMC is the first non-lethal anomaly considered for fetal surgical intervention. • Surgical intervention before 26 weeks of gestation may preserve motor function, reverse hindbrain herniation, and reduce the need for ventriculoperitoneal shunting. MMC Comorbidities (8) Life-long disabilities including: 1. Paraplegia 2. Hydrocephalus 3. Chiari II malformation 4. Bladder and bowel dysfunction 5. Skeletal deformities 6. Neurocognitive impairments. MMC Comorbidities Orthopedic abnormalities: 1. Caused by unbalanced action of muscles around joints, paralysis, and decreased sensation in the lower extremities. (8) 2. May be chronic or slowly progressive, and others arise acutely from progressive neurologic dysfunction such as shunt malfunction or tethered cord. (19) Sexuality • Most female fertile: pregnancy complicated by prolapse of uterus and perineum • Fertility in males: 15-20% (varies with level, recurrent UTIs, epididymitis, prostatitis) ADULTHOOD • Most complete high school • 50% go onto further education • 30 - 60% live independently • 25-50% are employed • Many go on to have families but they have a 5% risk of having children with NTD TREATMENT (20) • Treatment is multidisciplinary with needed expertise in pediatric neurosurgery, urology, orthopedics, and rehabilitation medicine. • Access to physical therapists, occupational therapists, social workers, nutritionists, and psychologists is also helpful. Neurological Management • Newborn 1. Closure of defect 2. Shunt placement for hydrocephalus 3. Relieve brain stem compression • Ongoing Problems 1. Shunt malfunctions 2. Symptomatic tethered cord Orthopedic/Rehabilitation Management • Function depends on level • Problems -Flexion contractures -Club feet -Dislocated hips -Scoliosis • Management -PT: Prevention/correction/improvement of function -Surgery: Tendon releases/casting/bracing Tendon transfer/bone fusion/spine fusion Urologic Management • Newborn -Study bladder function and upper tracts -Ensure complete bladder emptying -Treat reflux/hydronephrosis -Prevent/treat symptomatic UTIs • Ongoing: -Prevent renal compromise -Maintain urinary continence: Crede/timed voidings, CIC with or without medications, surgery to expand bladder capacity and/or prevent urethral leakage -Prevent/treat symptomatic UTIs Bowel Management • Bowel continence is a life long problem • Management strategies include: -Diet -Medications/suppositories -Manual evacuation: digital and enemas -Surgical Cognitive Difficulties in Spina Bifida • Large heterogeneous group: Most with intelligence in normal range but almost all have significant learning disabilities. • Higher lesions, CNS infections: correlated with lower IQ • Verbal abilities are superficially better than visual-spatial or quantitative abilities Cognitive Difficulties in Spina Bifida • Impairment in mental flexibility, efficiency of processing, conceptualization and problem solving • Inability to generalize or apply past experiences • Poor executive skills, attention deficits, and memory issues Other Problems • • • • • • • • • • Latex allergy Fine motor dysfunction Seizures Hearing loss Pulmonary compromise Intestinal obstruction Rectal prolapse Impotence Pathologic fractures Chronic cellulitis/thrombophlebitis Prognosis • Often physical and neurologic function deteriorate over time and become severe in adulthood. (20) • Bowman et, al studied outcomes for spina bifida in patients 20-25 years of age and found that there was a 24% overall mortality which continued to increase as the patients aged. (22) • 86% had undergone CSF diversion and 95% of these had at least 1 shunt revision. (22) • Associated anomalies may include club feet, flexion contractures at the hips, knees, and ankles, kyphosis, DDH, and/or structural anomalies of the airway, heart, GI tract, ribs, and kidneys. (20) Prognosis Continued • 85% attended or had graduated from high school or college. (22) • Many patients will have neurogenic bladders and may develop progressive deterioration of the upper urinary tract and chronic renal disease. (20) • Most patients will need lifelong treatment with CIC, medications, and/or surgery to be continent and preserve urological function. (20) • In almost all patients with MMC, innervation to the bowel and anus is affected which leads to dysmotility, poor sphincter control, and fecal incontinence. (20) Prognosis Continued (20) Progressive disability can be caused by : 1. Shunt malfunction 2. Progression of Chiari II symptoms related to compression to the cervical canal, hydromyelia, tethered cord 3. Orthopedic issues 4. Urologic issues. Mortality (21) Mortality is especially high inpatients with lesions above the T11 region. Most Common Causes of Death: • • • • Epilepsy Pulmonary embolus Acute hydrocephalus Acute renal sepsis References 1. Pruitt LJ, Living with Spina Bifida: A Historical Perspective, Pediatrics 130(2): 181-183, 2012 2. Macnab GH . The development of the knowledge and treatment of hydrocephalus. Dev Med Child Neurol. 1966;8(suppl 11):1–9 3. Lorber J. Results of treatment of myelomeningocele. An analysis of 524 unselected cases, with special reference to possible selection for treatment. Dev Med Child Neurol. 1971;13(3):279–303 4. Kirkland I. Urinary tract problems in spina bifida. Dev Med Child Neurol. 1962;4:314–319 5. Sharrard WJW, Zachary RB, Lorber J. Survival and paralysis in open myelomeningocele with special reference to the time of repair of the spinal lesion. Dev Med Child Neurol. 1967;9(suppl 13):35–50. 6. Johnson PR. Selective nontreatment and spina bifida: a case study in ethical theory and application. Bioethics Q. 1981;3(2):91–111 7. McCormick RA. To save or let die. The dilemma of modern medicine. JAMA. 1974;229(2):172–176 8. Khoury, C. Pathogenesis and types of occult spinal dysraphism. www.uptodate.com.libproxy.unm.edu/contents/pathogenesis-and-types-of -occult -spinaldysraphism 8/22/12, pp1-26 9. Adcock, NS, Thom, EA, Spong, CY, et al., A Randomized Trial of Prenatal versus Postnatal Repair of Myelomeningocoele, N Engl J Med 364: 993-1004, 2011 References 10. Boulet SL, Yang Q, Mai C, et al. Trends in the post fortification prevalence of spina bifida and anencephaly in the United States. Birth Defects Res A Clin Mol Teratol 2008;82:527-53 11. Wender-Ozegowska E, Wróblewska K, Zawiejska A, Pietryga M, Szczapa J, Biczysko R, Threshold values of maternal blood glucose in early diabetic pregnancy--prediction of fetal malformations. Acta Obstet Gynecol Scand. 2005;84(1):17. 12. Ceylan S, Duru S, Ceylan S, Valproic acid sodium-induced spina bifida occulta in the rat, Neurosurg Rev. 2001;24(1):31 13. Rosa FW, Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med. 1991;324(10):674 14. Jinkins JR, Sener RN, Idiopathic localized hydromyelia: dilatation of the central canal of the spinal cord of probable congenital origin, J Comput Assist Tomogr. 1999;23(3):351 15. Guggisberg D, Hadj-Rabia S, Viney C, Bodemer C, Brunelle F, Zerah M, Pierre-Kahn A, de Prost Y, Hamel-Teillac D, Skin markers of occult spinal dysraphism in children: a review of 54 cases. Arch Dermatol. 2004;140(9):1109. References 16. Estin D, Cohen AR, Caudal agenesis and associated caudal spinal cord malformations, Neurosurg Clin N Am. 1995;6(2):377 17. Pierre-Kahn A, Zerah M, Renier D, Cinalli G, Sainte-Rose C, Lellouch-Tubiana A, Brunelle F, Le Merrer M, Giudicelli Y, Pichon J, Kleinknecht B, Nataf F. Congenital lumbosacral lipomas, Childs Nerv Syst. 1997;13(6):298. 18. Danzier E, Johnson MP, Adzick NS, Fetal Surgery for myelomeningocoele: progress and perspectives, Dev Med Child Neurol 54(1): 8-14, 2012 19. Swaroop V and Dias L. Orthopedic issues in myelomeningocoele (spina bifida) www/uptodate.com.libproxy.unm.edu/contents/orthopedic-issues-myelomeningocele 8/22/12 (Updated 2/11/10) 20. McLone DG and Bowman RM Overview of the management of myelomeningocoele (spina bifida) www/uptodate.com.libproxy.unm.edu/contents/overview-of-the-management-ofmyelomeningocoele-(spina bifida) 8/22/12 pp. 1-10. 21. Mouetzinos MD and Stoffel JT, Management Goals for the Spina Bifida Neurogenic Bladder: A review from infancy to adulthood, Urologic Clinics of North America Vol 37(4) 2010 9copyright 2010 W.B. Saunders Company) References 22. Bowman RM, McLone DG, Grant JA, Tomita T, Ito JA, Spina bifida outcome: a 25-year prospective, Pediatr Neurosurg. 2001;34(3):114 Post-Test • 1. What is the most common type of Spina Bifida? (Myelomingocele) • 2. List 2 common causes of death in Spina Bifida patients. (Acute renal sepsis, epilepsy, pulmonary embolism, acute hydrocephalus) • 3. List 2 things that can increase the incidence of Spina Bifida. (Folate deficiency, certain drugs used for seizures: valproate, carbamazepine) • 4. List 3 co-morbidities that may be associated with MMC. (Paraplegia, bladder dysfunction, neurocognitive deficits)