Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
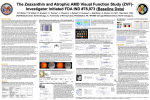
Reports Foveal Cone ERGs in Fellow Eyes of Patients With Unilateral Neovascular Age-Related Macular Degeneration Michael A. Sandberg, Sumiko Miller, and Alexander R. Gaudio Purpose. To determine whether fellow eyes with normal visual acuity of patients with unilateral neovascular agerelated macular degeneration (AMD) have retinal malfunction. Methods. Foveal cone electroretinograms (ERGs) were recorded from fellow eyes with visual acuities of 20/25 or better of 73 patients with unilateral neovascular AMD and from 28 normal volunteers of comparable age. Responses were elicited with a 4° stimulus flickering at 42 Hz presented by a stimulator-ophthalmoscope. Results. The study eyes of the patients were found to have foveal cone ERGs that, on average, were normal in amplitude but delayed in implicit (peak) time after adjustment of the data for age, sex, iris pigmentation, and refractive error by multiple linear regression. Based on all subjects, amplitude declined with increasing age and was smaller in eyes with darker irides; implicit time increased with increasing age. Conclusions. These findings suggest that fellow eyes with normal visual acuity of patients with unilateral neovascular AMD tend to have foveal cones that are normal in number but that function abnormally. In addition, foveal cone ERG amplitude should be adjusted for both age and iris pigmentation and implicit time should be adjusted for age when assessing retinal function of elderly patients. Invest Ophthalmol Vis Sci. 1993;34: 3477-3480. 1 he neovascular form of age-related macular degeneration (AMD) accounts for the majority of patients with severe visual loss from this disease.1 This form is characterized by choroidal neovascular membranes (CNVMs) that proliferate through breaks in Bruch's From the Berman-Gund Laboratory for the Study of Retinal Degenerations, Harvard Medical School, Massachusetts Eye and Ear Infirmary, Boston, Massachusetts. Supported by grants from the National Eye Institute (EY08398), the Retinitis Pigmentosa Foundation Fighting Blindness, and the Massachusetts Lions Eye Research Fund, Inc. Submitted for publication December 30, 1992; accepted March 29, 1993. Proprietary interest category: P (MAS, as inventor of the prototype instrument, receives royalties through Harvard Medical School based on sales of the Maculoscope). Reprint requests: Dr. Michael A. Sandberg, Berman-Gund Laboratory, Massachusetts Eye and Ear Infirmary, 243 Charles Street, Boston, MA 02114. membrane, resulting in detachment of the retinal pigment epithelium or neurosensory retina, formation of exudate, hemorrhage, and scarring. Patients with a CNVM in one eye are considered to be at approximately a 10% risk per year of developing a CNVM in the fellow eye.2 There is evidence that fellow eyes with normal visual acuity tend to have abnormalities of color matching and foveal dark adaptation that, when extreme, may be associated with an increased risk of neovascularization developing in those eyes.3 The purpose of the present study was to determine whether fellow eyes with normal visual acuity of patients with unilateral neovascular AMD also tend to have abnormal foveal cone electroretinograms (ERGs), an objective sign of outer retinal pathophysiology.4 METHOD. Foveal cone ERGs were recorded at baseline from the fellow eye of 73 patients (72.1 ± 0.8 years, mean ± SE) with unilateral neovascular AMD being followed prospectively to determine whether the foveal ERG can help predict which of these eyes develops a CNVM. These eyes had a corrected Snellen visual acuity of 20/25 or better, macular drusen ranging from hard and discrete in some patients to soft and confluent in others, and no evidence of a CNVM or other retinal disease. For comparison, we examined the eyes of 28 volunteers (69.7 ± 1 . 3 years, mean ± SE) whose ocular examination was normal; 10 (36%) of these volunteers had an occasional hard, discrete druse in the macula. The mean ages of the patients and normal volunteers were not significantly different by Student's Mest (P = 0.106). All study eyes afforded a clear view of the macula through the dilated pupil. Because the foveal cone ERG has been reported to depend upon age5 and the full-field ERG has been reported to depend not only upon age, but also upon sex, ocular pigmentation, and refractive error,6 all four factors were taken into account when evaluating foveal cone ERG differences between the two groups of subjects. The sex distribution of our patients was not significantly different from that of the normal volunteers by chi-square analysis (P = 0.702): Among the patients, there were 36 females and 37 males; among the normal volunteers, there were 15 females and 13 males. Iris pigmentation, which is correlated with fundus pigmentation,7 was used as a measure of ocular pigmentation and was coded before ERG testing as "light" for blue, green, or hazel irides and "dark" for brown irides. The distributions for iris pigmentation were also not significantly different for the two groups of subjects by chi-square analysis (P = 0.621): Of the patients, 43 had light irides and 30 had dark irides; of Investigative Ophthalmology & Visual Science, November 1993, Vol. 34, No. 12 Copyright © Association for Research in Vision and Ophthalmology Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933171/ on 05/10/2017 3477 Investigative Ophthalmology & Visual Science, November 1993, Vol. 34, No. 12 l. Multiple Linear Regression of Log10 Foveal Cone ERG Amplitude on Diagnosis, Age, Sex, Iris Pigmentation, and Spherical Equivalent Term* Diagnosis (0-1) Age Sex (0-1) Iris pigmentation (0-1) Spherical equivalent Estimate^ SE-f 0.002 -0.006 -0.021 0.018 0.002 0.016 0.10 -2.43 -1.34 0.922 0.017 0.184 0.050 0.003 0.016 0.008 3.08 0.33 0.003 0.740 t Ratio P Value * For diagnosis, 0 = AMD and 1 = normal; for sex, 0 = female and 1 = male; for iris pigmentation, 0 = light (blue, green, or hazel) and 1 = dark (brown). f Regression model halves estimate and standard error for categorical variables (i.e., diagnosis, sex, and iris pigmentation). a • • -0.3, -0.4- 601; TABLE -v.z * • • An the normal volunteers, 18 had light irides and 10 had dark irides. Refractive error was coded as the spherical equivalent (i.e., sphere + 0.5 X cylinder). The patients were more hyperopic than the normal volunteers by Student's t-test (P = .012), consistent with previous reports for refractive error in AMD8: For the patients, the mean spherical equivalent ± SE was 1.47 ± 0.23 diopters; for the normal volunteers, the mean spherical equivalent ± SE was 0.37 ± 0.37 diopters. After the nature and possible consequences of the study had been explained, all subjects gave informed consent before examination. Foveal cone ERGs were recorded in a dimly lit room with a hand-held, dual-beam, stimulator-ophthalmoscope (Maculoscope, Doran Instruments, Littleton, MA). Responses were elicited with a 4° white stimulus flickering at 42 Hz centered within a 12° white, steady surround. These lights passed through the dilated pupil as a 1 mm diameter beam in maxwellian-view; the beam was positioned within the pupil so that the stimulus was visualized on the fovea by the examiner throughout testing. Responses were monitored with a Burian-Allen bipolar contact lens electrode on the topically anesthetized cornea and were differentially amplified, smoothed by a narrow bandpass filter tuned to 42 Hz, digitized, and summed. Waveforms, which appear sinusoidal, were quantified by Fourier analysis with respect to amplitude and phase; phase was then converted to implicit time (i.e., time interval from stimulus onset to the corresponding cornea-positive response peak) based on a previously established relationship.9 Testing involved at least three consecutive recordings until responses had stabilized. This research followed the tenets of the Declaration of Helsinki and had been approved by the internal review boards of the Massachusetts Eye and Ear Infirmary and Harvard Medical School. -0.5- •Do • • .": • = ' • " " "1 -0.6- • OQ •a Ampliti 3478 m D • • • • -0.7- • • • • 0 • -0.8-0.9-1.055 ( • — • patients a — 0 normals 1 1 60 65 • ) 1 • 1 • 1 1 75 80 Age (years) 85 70 1 9( FIGURE 1. Data and regression line for foveal cone ERG amplitude versus age for fellow eyes of patients with unilateral neovascular AMD and for normals. Data have been adjusted for the significant effect of iris pigmentation on amplitude. Foveal cone ERG amplitudes, which were positively skewed, were converted to common logarithms (log10) to approximate a normal distribution. Amplitude and implicit time were each regressed on age, spherical equivalent, and indicator variables for diagnosis, sex, and iris pigmentation by multiple linear regression. This approach allowed determination of the relationship of foveal cone ERG amplitude or implicit time to diagnosis after adjusting for the relationships of each ERG measure to age, sex, iris pigmentation, and spherical equivalent. Statistical analyses were performed with JMP, version 2.0.4 (SAS Institute Inc., Cary, NC) on a Macintosh computer (Apple Computer, Cupertino, CA). RESULTS. Foveal cone ERG amplitude was unrelated to diagnosis, sex, or equivalent sphere (Table 1). The patients and normal volunteers had identical mean amplitudes (0.26 /uV) after adjusting for age, sex, iris pigmentation, and spherical equivalent. On the other hand, amplitude was significantly related to both age and iris pigmentation, decreasing on average by 0.06 log unit (13%) for each increasing decade of age (P = .017) and by 0.10 log unit (21%) for eyes with dark irides compared to eyes with light irides (P - .003). However, when log amplitude was regressed upon both age and iris pigmentation separately for the patients and normal volunteers, the effects of age and iris pigmentation were significant only for the patients (although the normal volunteers showed similar trends). The relationships of amplitude to age are illustrated in Figure 1. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933171/ on 05/10/2017 3479 Report Table 2 shows that foveal cone ERG implicit time was significantly related to diagnosis and age, but not to sex, iris pigmentation, or spherical equivalent. The mean implicit time adjusted for age, sex, iris pigmentation, and spherical equivalent was more than 2 ms greater in the study eyes of the patients (37.2 ms) compared to that for the study eyes of the normal volunteers (35.1 ms). Implicit time also increased on average by 1.0 ms for each increasing decade of age for all subjects combined. However, when implicit time was regressed upon age separately for the patients and normal volunteers, the effect of age was significant only for the patients (although the normal volunteers again showed a trend in the same direction). The relationships of implicit time to age are illustrated in Figure 2. In addition to the regression lines, this graph shows the age-adjusted 95% confidence limits for normal implicit time based on these normal data. Fifteen patients (21%) had an implicit time that exceeded the upper normal confidence limit, whereas none had an implicit time that fell beneath the lower confidence limit. DISCUSSION. The results show that fellow eyes with normal visual acuity of patients with unilateral neovascular AMD had a mean foveal cone ERG implicit time that was slower than normal. In approximately one out of five patients, the implicit time exceeded the normal upper limit. Slowing of the foveal cone ERG indicates outer retinal malfunction, and this malfunction may be implicated in the abnormalities of color matching and/or foveal cone dark adaptation reported previously for fellow eyes with normal visual acuity of patients with unilateral neovascular AMD.3 However, it is not yet known whether an abnormal value of implicit time in our patients is related to an increased risk of developing a CNVM. The nor- 2. Multiple Linear Regression of Foveal Cone ERG Implicit Time on Diagnosis, Age, Sex, Iris Pigmentation, and Spherical Equivalent TABLE Std Term* Estimatef Errorf t-Ratio P-Value Diagnosis (0-1) 1.037 0.095 -0.202 0.211 0.028 0.183 4,.92 3,.42 - 1 .10 <0 .001 <0 .001 0 .274 -0.191 -0.061 0.189 0.096 - 1 .01 - 0 .64 0 .315 0 .525 Age Sex (0-1) Iris pigmentation (0-1) Spherical equivalent * For diagnosis, 0 = AMD and 1 = normal; for sex, 0 = female and 1 = male; for iris pigmentation, 0 = light (blue, green, or hazel) and 1 = dark (brown). f Regression model halves estimate and standard error for categorical variables (i.e., diagnosis, sex, and iris pigmentation). 46" • patients ] a normals J 44- 30" 55 I 60 65 I 1 70 75 80 Age (years) 85 90 2. Data and regression line for foveal cone ERG implicit time versus age for fellow eyes of patients with unilateral neovascular AMD and for normals. Top and bottom dashed lines represent upper and lower 95% confidence limits for normal implicit time. FIGURE mal mean amplitude for the study eyes of our patients is consistent with their normal visual acuities which, presumably, signify normal numbers of cones, at least in the foveola. Their normal amplitude to 42 Hz flicker is also consistent with a report that fellow eyes with good visual acuity of patients with unilateral neovascular AMD had, on average, a normal foveal psychophysical sensitivity to 40 Hz flicker.10 Our findings suggest that the study eyes of our patients generally had a normal complement of foveal cones for their age, although these cones tended to function abnormally with respect to response kinetics. The data analyses also bear upon whether age, sex, ocular pigmentation, or refractive error affect the foveal cone ERG. We observed that foveal cone ERG amplitude tended to fall and implicit time tended to increase with increasing age, based on our combined sample of patients and normal volunteers and with respect to the patients alone. These effects of age, however, were not statistically significant for our normal volunteers alone. We suspect that this resulted from a lack of power (i.e., sample size), because the normal volunteers showed trends in the same directions as the patients and because significant relationships between amplitude and age and between implicit time and age have been reported previously for the foveal cone ERG of normal subjects.5-6 We also noted that amplitudes tended to be higher in eyes with light pigmented irides than in eyes with dark pigmented irides, reminiscent of the effect of ocular pigmentation on the full- Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933171/ on 05/10/2017 3480 Investigative Ophthalmology & Visual Science, November 1993, Vol. 34, No. 12 field ERG 6 and possibly indicative of differences in photoreceptor illumination. We did not observe an increase in amplitude in females relative to males or in hyperopes relative to myopes, as have been described for the full-field ERG. 6 These observations indicate that amplitude should be adjusted for age and iris pigmentation and that implicit time should be adjusted for age when assessing the foveal cone ERG of elderly patients. Key Words macular degeneration, choroidal neovascularization, electroretinography, age, ocular pigmentation References 1. Ferris FL III, Fine SL, Hyman LG. Age-related macular degeneration and blindness due to neovascular maculopathy. Arch Ophthalmol. 1984; 102:1640-1642. 2. Teeters VW, Bird AC. The development of neovascularization of senile disciform macular degeneration. Am J Ophthalmol. 1973;76:1-18. 3. Eisner A, Klein ML, Zilis JD, Watkins MD. Visual function and the subsequent development of exudative age-related macular degeneration. Invest Ophthalmol VisSci. 1992;33:3091-3102. 4. Jacobson SG, Sandberg MA, Effron MH, Berson EL. Foveal cone electroretinograms in strabismic amblyopia: Comparison with juvenile macular degeneration, macular scars and optic atrophy. Trans Ophthal Soc UK. 1979; 99:353-356. 5. Birch DG, Fish GE. Focal cone electroretinograms: Aging and macular disease. Doc Ophthalmol. 1988;69: 211-220. 6. Sandberg MA. Technical issues in electroretinography. In: Heckenlively JR, Arden GB, eds. Principles and Practice of Clinical Electrophysiology of Vision. St. Louis: Mosby Year Book; 1991:371-383. 7. Weiter JJ, Delori FC, Wing GL, Fitch KA. Relationship of senile macular degeneration to ocular pigmentation. Am J Ophthalmol. 1985;99:185-187. 8. Goldberg J, Flowerdew G, Smith E, Brody JA, Tso MOM. Factors associated with age-related macular degeneration: An analysis of data from the first National Health and Nutrition Examination Survey. Amf Epidemiol. 1988; 128:700-710. 9. Sandberg MA, Jacobson SG, Berson EL. Foveal cone electroretinograms in retinitis pigmentosa and juvenile macular degeneration. Am] Ophthalmol. 1979; 88: 702-707. 10. Mayer MJ, Spiegler SJ, Ward B, Glues A, Kim CBY. Mid-frequency loss of foveal flicker sensitivity in early stages of age-related maculopathy. Invest Ophthalmol VisSci. 1992; 33:3136-3142. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933171/ on 05/10/2017