Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
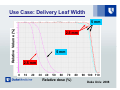
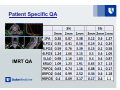
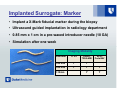
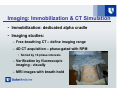
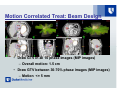
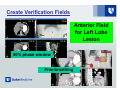
Treatment Quality Assurance for Linac Based SRS/SBRT Fang-Fang Yin, PhD Duke University Medical Center SEAAPM 2011, Myrtle Beach, SC Acknowledgements • SEAAPM Symposium Organization Committee – especially to J. Daniel Bourland, PhD • SRS/SBRT Team at Duke • Duke University has a research agreement with Varian Medical Systems SRS and SBRT Radiation therapy with a single fraction high dose or a few hypo-fractionated prescription doses to lesions. The challenge for SRS and SBRT is to accurately and precisely deliver conformal high dose radiation to the target and minimize normal tissue damage. Process for Image-Guided SRS/SBRT Case selection Assessment Immobilization Onboard imaging 3/4-D simulation Treatment N 3/4-D planning Onboard vs. Reference Correction? Patient setup Onboard imaging Y General Processes for SRS/SBRT • Patient process – – – – – – – – – Consultation Immobilization/imaging Planning/prescription Patient specific QA Localization Delivery Motion management Real-time verification Treatment assessment • Physics process – – – – – – – Beam data QA: Safety QA: daily, radiation / IGRT W-L testing Dose calculation QA device QA Beam calibration An Integrated Treatment Process SBRT Practice Guidelines: AAPM TG 101 Process QA: Quality/Risk Factors • Program development – Infrastructure • Equipment: hardware and software • Instrumentations – Procedures and policies (what and how to do from patient in to out) • The team untrained/unqualified – Physician – Physicist – Other staff: therapists, nurses, … QA Programs for a SRS/SBRT Unit Duke Center for SRS/SBRT (Novalis Tx) • Procedures and policies for SRS/SBRT • QA for delivery system • QA for imaging system • QA for planning system • QA for immobilization device • QA for patient specific plan (i.e., IMRT/VMAT) • QA for record & verifying system • QA for match software • QA for gating system • QA for 6D couch • …… Use Case: Delivery Leaf Width Relative Volume (%) 5 mm 2.5 mm 5 mm 2.5 mm 0 10 20 30 40 50 60 70 Relative dose (%) 80 90 100 110 Duke Univ. 2008 Process QA: Quality/Risk Factors • Skip some procedures – Consultation: case was not discussed between physician and physicist. At the time of imagng, not sure how to position patient … • Not properly immobilized and not enough anatomy was included in images. As a result, patient resim and suboptimal positioning • Rushing to get patient treated and to be told QA may be done after first treatment AAPM TG 101 Recommendation: SBRT Patient Selection Criteria • • The most effective way: participation in formal group trials; whether single-institutional or multi-institutional trials sponsored by the NCI or other sources, or through NCIsponsored cooperative group trials such as those of the RTOG. When appropriate protocols are not available, clinicians must decide whether they will treat patients in accordance with published guidelines or develop new SBRT guidelines. At a minimum, an institutional treatment protocol or set of guidelines should be developed by radiation oncologists and physicists. General QA Guidelines • • • • • • • • • • AAPM TG 40 AAPM TG 56 SRS, 58 EPID AAPM TG 101 AAPM TG 104 AAPM TG 119 AAPM TG 142 AAPM TG 75, 76 ASTRO TGs, reports ACR guidelines …. Performance QA: Physics Process Daily machine warmup Daily, Monthly, annual QA (TG142) Additional: WL test (combined with daily IGRT) Patient specific QA chart checking MU calculation IMRT/VMAT QA Time-out at machine Physicist/physician presence check list and sign off sheet Patient Specific QA IMRT QA Patient Specific QA VMAT QA Performance QA: Quality/Risk Factors – W-L testing: what if BB is off center? QA Consideration for QA Phantoms How to select: Daily QAphantom phantom Imaging Block Tray Dosimetry phantom CT phantomIMRT phantom 4D motion phantom Tissue phantom • Purpose • Multiple purposes • Accuracy • Ease of use • Simplicity • Size and weight • Quality • Cost • ….. • Maintenance QA Considerations for QA Devices Films Detectors Electrometers and cables Analysis software Beam data scanner How to • Acceptance testing • Functionality • Calibration • Maintenance • ….. Clinical Needs of QA Phantoms • For existing QAs: – – – – Accurate and simple Multi-task with analysis tool Proper size and efficient Easy to do and analysis • For emerging QAs: – – – – 4D MRI Proton 4D gated treatment …… Process QA: Immobilization – – – – – – – – – Patient movement Organ motion Patient comfort Reproducibility Effort to positioning Accuracy Simulation time Beam orientation Localization Imaging Head and Body Immobilization “Frameless” SRS/SBRT? • Immobilization – Invasive frame: pins, metal devices, etc. – Non-invasive frame: Bodyframe, BodyFix – Constraints: alpha cradle, vacuum bag, etc. • Geometric correlation between patient and machine coordinates – On-board imaging and fusion (IGRT) – Mechanical (Constraints): Localization rods and distance measures – Visual: Measurements, laser, skin marks Recommendation for Patient Positioning, Immobilization, Localization and Delivery • For SBRT, image-guided localization techniques shall be used to guarantee the spatial accuracy of the delivered dose distribution with a high confidence level. • Body frames and associated fiducial systems may be used for immobilization and coarse localization; however, they shall not be used as a sole localization technique. • To maintain the spatial accuracy throughout the treatment delivery through either integrated image-based monitoring systems or through aggressive immobilization of appropriate targets, such as the spine. AAPM TG101 AAPM TG 101 Recommendation: Simulation imaging Regardless of imaging modality, simulation of the patient should take place with the patient in the treatment position. The simulation study should cover the target and all organs at risk to obtain geometric and dosimetric information for the treatment setup. Slice thickness: < 3 mm near clinically important organs Process QA: Planning • Planning/prescription – Delivery technique, choose after simulation, KISS – Targets and organ at risk volumes, skin, chestwall, lung low dose volume – Previous treatment • Contour accuracy – Image fusion, positioning difference, imaging system accuracy – Contour deviation – Margin for SRS, GTV-PTV: 1 mm, 2 mm, 3 mm…. Treatment Planning Recommendation • The adequacy of target margins i.e., GTV, CTV, ITV, in SBRT should be based on – understanding of how the steep dose gradients – high fractional doses of SBRT affect the accuracy of traditional margin recipes – the natural history of the tumor – the limitations of in-house localization capabilities to reduce random and systematic treatment uncertainty – from information in the current literature • Simultaneously, centers should make systematic efforts to gather and analyze clinical results to improve margin design in the future AAPM TG101 Normal Tissue Dose Tolerance TG 101 Recommendation: Normal tissue dose tolerances in the context of SBRT are still evolving and only a limited experience exists from which to draw recommendations. Except in the setting of IRB approved Phase I protocols, critical organ tolerance doses based on the SBRT experience in the evolving peer-reviewed literature must be respected. Dose Calculation Algorithm • Recommendation: Algorithms that account for 3D scatter integration such as convolution/superposition have been found including by the RPC study to perform adequately in most clinical situations, including in many cases circumstances where there is a loss of electronic equilibrium such as the lung tissue interface or tumor margin in low-density medium. • Calculation algorithms accounting for better photon and electron transport such as Monte Carlo would be ideal for the most demanding circumstances, such as a small lesion entirely surrounded by a low-density medium. AAPM TG101 AAPM TG 101: Motion Management AAPM Task Group 76 describes the various tumor-motion strategies in detail. Techniques to image moving targets include slow CT breath-hold techniques, gated approaches, 4DCT used in conjunction with MIP, minimum intensity projection and respiration-correlated PET-CT. If target and radiosensitive critical structures cannot be localized on a sectional imaging modality with sufficient accuracy because of motion and/or metal artifacts, SBRT should not be pursued as a treatment option. Recommendation for Moving Target For all SBRT patients with targets in the thorax or abdomen, a patient-specific tumor-motion assessment should be available. This serves to quantify the motion expected during the respiratory cycle. This data may then be used a) To determine if the patient’s treatment would likely benefit from techniques such as respiratory gating; b) To quantify the residual motion expected during the respiratory gated delivery if such delivery is used; C) To design margins for treatment planning; and D) To quantify and account for any phase shift between Process QA: Discrepancy of Contours from Different Images ITV discrepancy Performance QA: Quality/Risk Factors Physics dosimetry measurement: – Beam data – Profile – PDD – Output factor Detector 2 Detector 1 Small Field Dosimetry Error From 0.65Æ0.32 Ion chamber Yin et al Med. Phys. 2002 Special Dosimetry Recommendation Due to the small dimensions and steep dose gradients of photon beams used in SRS/SRT and IMRT, an appropriate dosimeter with a spatial resolution of approximately 1 mm or better stereotactic detectors is required to measure the basic dosimetry data, e.g., the total scatter factor or relative output factor, tissuemaximum ratio, and off-axis ratios. Even with stereotactic detectors, careful detector-phantom setup, and detailed dose corrections, one might still find more than 10% discrepancies among the measurements of very small fields (<10 mm in diameter) AAPM TG101 Process QA: Quality/Risk Factors • Verification procedures – – – – Patient position Target localization Motion checking …. • Image guidance – Method – technique IGRT Case: Intra-Fraction Imaging Example of dual x-ray imaging IGRT Case: 2D and 3D for Liver Tumor CBCTs 2-D Images On-Board Imaging IGRT Case: 3-D CBCT Free-Breath ITV CBCT images after correction CBCT images prior to correction Planning CT with target contours Post-treatment CBCT Wang et al Ref J 2007 IGRT Case: Image Analysis Tool Bladder in planning CT as contour overlay Daily Bladder as image In-room CT Hardware and software application and verification Bony Structure is off Variable rectal filling observed In-room CT Prostate target is aligned with the CT image Reference CT TG 104 2008 IGRT Case: CBCT for Brain Onboard verification Plan Imaging Device Inaccuracy 5 mm shifts Yin Risk Factors in IMRT/VMAT/IGRT Original 2 cm Mis-P 2 cm Mis-P 2 cm Mis-P 5% U-Dose Original 5% U-Dose Original 5% U-Dose PTV54: 7mm from CTV PTV76: 5mm from CTV Yin Anatomic Surrogate Imaging: Soft Tissue Organ and Isodose Planning CT 50Gy 40Gy CBCT Recommendation for Treatment • At least one qualified physicist be present from the beginning to end of the first treatment fraction. • For subsequent fractions, it is recommended that a qualified physicist be available, particularly for patient setup in order to verify immobilization, imaging, registration, gating, and setup correction. • Radiation therapists be well-trained in SBRT procedures. • A radiation oncologist approve the result of the image guidance and verify the port films before every fraction of the SBRT treatment. AAPM TG101 A Clinical Case for Integrated Respiratory Gated Treatment Verification for Liver Cancers What Critical Information Is Needed for Verifying Gated Treatment of Liver? • Target to be verified • Tumors • Surrogate to the target • • • • • Anatomical marker Implanted marker Verification of surrogate Imaging Motion correlated signal Liver case: Target-Surrogate Implanted marker Rt lobe PTV 112.1 cm3 Lt lobe PTV 35.3 cm3 Anatomical surrogate (diaphragm) Implanted Surrogate: Marker • Implant a X-Mark fiducial marker during the biopsy • Ultrasound guided implantation in radiology department • 0.85 mm x 1 cm in a pre-waxed introducer needle (18 GA) • Simulation after one week Imaging Modality CT-kV FluoroTRUS-MRI 0.45 mm Y Y 0.85 mm Y Y Y Y Y Diameter 1.15mm EPIDPortal-MV Imaging: Immobilization & CT Simulation • Immobilization: dedicated alpha cradle • Imaging studies: – Free-breathing CT – define imaging range – 4D CT acquisition – phase-gated with RPM • Sorted by 10 phase intervals – Verification by fluoroscopic imaging - visually – MRI images with breath-hold Motion Correlated Treat: Beam Design • Draw GTV in all 10 phase images (MIP images) – Overall motion: 1.5 cm • Draw GTV between 30-70% phase images (MIP images) – Motion <= 5 mm Localization Techniques • OBI orthogonal images – within phase window • CBCT images – ITV – not in phase window • Real-time portal imaging – tracking of markers • Verification surrogates: – Rt lobe lesion – implanted marker – Lt lobe lesion - diaphragm Create Verification Fields Rt Lat Field for Right Lobe Lesion 50% phase window Free-breathing Create Verification Fields Anterior Field for Left Lobe Lesion 50% phase window Free-breathing Target Localization – Orthogonal Imaging Right lob lesion Phase-gated OBI images Target Localization for ITV– CBCT Right lobe lesion Free-breathing CBCT Verification of Gating Windows – Fluoroscopic Imaging Gating window Right lobe lesion Verification of Gating Windows – Fluoroscopic Imaging Left lobe lesion Rt Lat Setup Field Ant Setup Field Treat Verification of Implanted Surrogate – Cine Portal Imaging Right lobe lesion Treat Verification of Anatomical Surrogate – Cine Portal Imaging Left lobe lesion Clinical Implementation of SRS/SBRT • • • • • • • Establish the scope of the program including a selection of treatment sites and the clinical goals for each site. Determine a treatment modality, dose-fractionation scheme, and treatment planning goals target definition, target coverage, conformity index, etc. that support the clinical goals for each treatment site. For each treatment modality and treatment scheme, determine the equipment requirements for patient positioning, treatment delivery, and verification. Determine personnel needs for implementation and maintenance. Establish and perform acceptance and commissioning test procedures for the equipment. Establishing simulation, treatment planning, delivery and verification guidelines, reporting methodology and routine QA procedures, and Conducting personnel training. Summary • Each SRS/SBRT deserve special attention • Accuracy and precision is critical • QAs should be implemented as an integrated process • Both individual and systematic factors should be considered for the QA process • End-to-end test is a critical procedure Thank you! Quality Assurance Program • A program that is designed to control and maintain the standard of quality set for that program • In radiation oncology, it is essentially a set of policies and procedures to maintain the quality of patient care • The general standards and criteria of QA are usually set collectively by the profession