Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
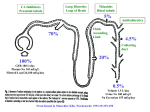
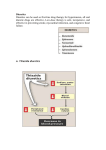
Diuretic Agents Carbonic Anhydrase Inhibitors Carbonic anhydrase is in the PCT, where it catalyzes the dehydration of H2CO3. By blocking carbonic anhydrase, drugs block NaHCO3 reabsorption and cause diuresis. Carbonic anhydrase inhibitors are now rarely used as diuretics They have several specific applications. The prototypical drug is acetazolamide. Carbonic Anhydrase Inhibitors the inhibition of enzyme causes HCO3– losses and metabolic acidosis the major clinical applications of acetazolamide involve sites other than the kidney. The ciliary body of the eye secretes HCO3– from the blood into the aqueous humor. formation of CSF by the choroid plexus also involves HCO3– secretion. Clinical Indications Glaucoma (dorzolamide, brinzolamide) Urinary Alkalinization Uric acid, cystine, and other weak acids are reabsorbed from acidic urine. renal excretion of cystine (in cystinuria) can be enhanced by increasing urinary pH. Metabolic Alkalosis Acute Mountain Sickness Toxicity Metabolic Acidosis Renal Stones Calcium salts are relatively insoluble at alkaline pH. Renal Potassium Wasting Drowsiness and paresthesias after large doses Contraindications alkalinization of the urine decreases urinary excretion of NH4+ (converts it to rapidly reabsorbed NH3) in patients with cirrhosis this contributes to hyperammonemia and hepatic encephalopathy. Loop Diuretics Loop diuretics selectively inhibit NaCl reabsorption in the TAL. Loop diuretics are the most efficacious diuretics because: large NaCl absorptive capacity of TAL The two prototypical drugs of this group are furosemide and ethacrynic acid. bumetanide and torsemide are also loop diuretics. The duration of effect for furosemide is 2–3 hours. Pharmacodynamics Loop diuretics inhibit NKCC2, the Na+/K+/2Cl– transporter in the TAL. They reduce both the reabsorption of NaCl and lumen-positive potential that comes from K+ recycling. This positive potential normally drives divalent cation reabsorption in the loop So loop diuretics cause an increase in Mg2+ and Ca2+ excretion. Pharmacodynamics Prolonged use can cause significant hypomagnesemia intestinal absorption of Ca2+ can be increased and Ca2+ is actively reabsorbed in the DCT So loop diuretics do not generally cause hypocalcemia in disorders that cause hypercalcemia, Ca2+ excretion can be usefully enhanced by loop diuretics combined with saline infusions Both furosemide and ethacrynic acid have also been shown to reduce pulmonary congestion and LVEDP in heart failure before diuretic effect. Clinical Indications Acute Renal Failure They increase urine flow and enhance K+ excretion. they can flush out pigment cast in the tubules. ???? Toxicity Hypokalemic Metabolic Alkalosis They increase salt delivery to the collecting duct. This leads to increased secretion of K+ and H+ Ototoxicity dose-related hearing loss may happen and is usually reversible. It is most common in diminished renal function or those who are using other ototoxic drugs. Toxicity Hyperuricemia They may cause hyperuricemia and precipitate attacks of gout. This is caused by hypovolemia-associated enhancement of uric acid reabsorption in the PCT. Hypomagnesemia Occurs in dietary magnesium deficiency. It can be reversed by oral magnesium. Toxicity Allergic & Other Reactions Most of the loop diuretics are sulfonamides. skin rash, eosinophilia, and interstitial nephritis are occasional adverse effects. This usually resolves rapidly after drug withdrawal. They can cause severe dehydration. thirst and increased water intake can cause severe hyponatremia. hypercalcemia can occur in volume-depleted patients who have another cause for hypercalcemia (carcinoma). Thiazides thiazides inhibit NaCl transport in the DCT. Thiazides All thiazides are secreted in the proximal tubule They compete with the secretion of uric acid So thiazides may elevate serum uric acid level. Thiazides block the Na+/Cl– transporter (NCC). thiazides actually enhance Ca2+ reabsorption. thiazides may rarely cause hypercalcemia They are useful for kidney stones caused by hypercalciuria. Thiazides Clinical Indications Hypertension heart failure nephrolithiasis due to idiopathic hypercalciuria, Toxicity Hypokalemia, Metabolic Alkalosis and Hyperuricemia Hyperglycemia due to impaired release of insulin. Hyperlipidemia as a 5–15% increase in total serum cholesterol and LDL. Allergic Reactions (the thiazides are sulfonamides). Hyponatremia is an important adverse effect of thiazides. It is due to elevation of ADH and increased thirst. Potassium-Sparing Diuretics Potassium-Sparing Diuretics Spironolactone Eplerenone Amiloride Triamterene Potassium-Sparing Diuretics They antagonize the effects of aldosterone. Inhibition may occur by: direct antagonism of receptors (spironolactone, eplerenone) inhibition of Na+ influx (amiloride, triamterene). Eplerenone is more selective so has less side effects. They cause metabolic acidosis. Potassium-Sparing Diuretics Clinical Indications They are useful in primary and secondary hyperaldosteronism Use of thiazides or loop agents can exacerbate volume depletion and causes secondary hyperaldosteronism. eplerenone has been found to reduce myocardial perfusion defects after MI. eplerenone reduced mortality rate by 15% (compared with placebo) in heart failure after MI. Toxicity They can cause life-threatening hyperkalemia. This risk is greatly increased by: renal disease the use of drugs that inhibit renin (β blockers) the use of drugs that inhibit angiotensin II activity (ACEIs, angiotensin receptor blockers (ARBs)). Combinations of K+-sparing and thiazides ameliorate thiazide-induced hypokalemia and alkalosis. Toxicity Metabolic Acidosis Gynecomastia, impotence, and is reported with spironolactone but not with eplerenone. Patients with chronic renal insufficiency are especially vulnerable to hyperkalemia. Agents That Alter Water Excretion Osmotic Diuretics Antidiuretic Hormone (ADH) Agonists Antidiuretic Hormone (ADH) Antagonists Osmotic Diuretics Any osmotically active agent promotes a water diuresis. Such agents reduce intracranial and intraocular pressure The prototypic osmotic diuretic is mannitol. Oral mannitol causes osmotic diarrhea so for systemic effect, it is given parenterally. Osmotic Diuretics they also oppose the action of ADH. They reduce Na+ as well as water reabsorption. The natriuresis is of lesser magnitude than the water diuresis, leading to hypernatremia. Clinical indications They increase water excretion in preference to sodium excretion. This is useful when avid Na+ retention limits the response to conventional agents. It is used to prevent anuria from large pigment loads to the kidney. Reduction in ICP in neurologic conditions & IOP before ophthalmologic procedures. Toxicity Mannitol is rapidly distributed in the extracellular compartment and extracts water from cells. Prior to the diuresis, this leads to expansion of the extracellular volume and hyponatremia. This can complicate heart failure and may produce pulmonary edema. In diminished renal function, mannitol is retained and causes osmotic extraction of water from cells, leading to hyponatremia. ADH Agonists Vasopressin and desmopressin are used in the treatment of central diabetes insipidus. The renal action appears to be mediated primarily via V2. ADH Antagonists Syndrome of Inappropriate Antiduiretic Hormone (SIADH) secretion, causes water retention. conivaptan is an antagonist against both V1a and V2 ADH receptors. tolvaptan is an antagonist with more selectivity for V2 ADH receptors than V1a. Lithium & demeclocycline have anti-ADH effects, but have many side effects and are not used. Clinical Indications In SIADH when water restriction has failed. Toxicity Nephrogenic Diabetes Insipidus If lithium is used for a psychiatric disorder, nephrogenic diabetes insipidus can be treated with a thiazide. Summary In English Thank you Any question? Proximal Tubule Sodium bicarbonate (NaHCO3 ), sodium chloride (NaCl), glucose, amino acids, and other organic solutes are reabsorbed via specific transport systems in the early proximal tubule (proximal convoluted tubule, PCT). Potassium ions (K+) are reabsorbed via the paracellular pathway. Water is reabsorbed passively, Of the various solutes reabsorbed in the proximal tubule, the most relevant to diuretic action are NaHCO3 and NaCl. Of the currently available diuretics, only one group (carbonic anhydrase inhibitors, which block NaHCO3 reabsorption) acts predominantly in the PCT. PCT Because HCO3– and organic solutes have been largely removed from the tubular fluid in the late proximal tubule, the residual luminal fluid contains predominantly NaCl. Under these conditions, Na+ reabsorption continues, but the H+ secreted by the Na+/H+ exchanger can no longer bind to HCO3–. Free H+ causes luminal pH to fall, activating a poorly defined Cl–/base exchanger (Figure 15–2). The net effect of parallel Na+/H+ exchange and Cl–/base exchange is NaCl reabsorption. PCT Organic acid secretory systems are located in the proximal tubule (S2 segment). These systems secrete organic acids (uric acid, NSAIDs, diuretics, antibiotics) into the luminal fluid. These systems thus help deliver diuretics into the tubule. Henle loop Water is extracted from the descending limb of this loop by osmotic forces. The thin ascending limb is relatively waterimpermeable. The thick ascending limb (TAL) actively reabsorbs NaCl from the lumen TAL is impermeable to water so Na reabsorption dilutes the tubular fluid, hence, diluting segment. Henle loop The NaCl transport system in TAL is a Na+/K+/2Cl– cotransporter (NKCC2 or NK2CL) (Figure 15–3). This transporter is selectively blocked "loop" diuretics. the action of the transporter contributes to excess K+ accumulation within the cell. inhibition of salt transport by loop diuretics, also causes an increase in excretion of divalent cations. DCT DCT is relatively impermeable to water and NaCl reabsorption further dilutes the fluid. NaCl transport is by an thiazide-sensitive Na+ and Cl– cotransporter (NCC, Figure 15–4). Ca2+ is actively reabsorbed Ca2+ channels and a Na+/Ca2+ exchanger (Figure 15–4). This process is regulated by parathyroid hormone. Collecting Tubule The cortical collecting tubule (CCT) is the most important site of K+ secretion by the kidney It is the site at which all diuretic-induced changes in K+ balance occur. there is an important relationship between Na+ delivery to the CCT and the resulting secretion of K+. Diuretics that act upstream of the CCT increase Na+ delivery to this site and enhance K+ secretion. Collecting Tubule If an anion that cannot be reabsorbed readily (eg, HCO3–), is present the negative potential is increased, and K+ secretion is enhanced. This mechanism and enhanced aldosterone secretion is the basis for most diuretic-induced K+ wasting. ADH, also called arginine vasopressin (AVP) controls the permeability of this segment to water. A new class of drugs, the vaptans, are ADH antagonists. Diuretic Combinations Loop Agents & Thiazides Since these agents have a short half-life (2–6 hr.), refractoriness may be due to an excessive interval between doses. Loop agents and thiazides in combination often produce diuresis when neither agent alone is effective. Metolazone is the thiazide-like drug used in patients refractory to loop agents alone The combination of loop diuretics and thiazides can mobilize large amounts of fluid, even in patients who have not responded to single agents. close hemodynamic monitoring is essential and outpatient use is not recommended. K+-wasting is extremely common and may require parenteral K+ Diuretic Combinations Potassium-Sparing & Loop Agents or Thiazides Hypokalemia develops in many patients taking loop diuretics or thiazides. This can be managed by NaCl restriction or taking KCl supplements. If not treated, addition of a K+-sparing diuretic can lower K+ excretion. This should be avoided in renal insufficiency and in those receiving angiotensin antagonists in whom lifethreatening hyperkalemia can develop. Clinical Pharmacology Edematous States excessive diuretic therapy may lead to further compromise of the effective arterial blood volume the use of diuretics requires an understanding of the pathophysiology of the underlying illness. Heart Failure Edema associated with heart failure is generally managed with loop diuretics. In some instances, salt and water retention may become so severe that a combination of thiazides and loop diuretics is necessary. In treating the heart failure patient with diuretics, it must always be remembered that cardiac output in these patients is being maintained in part by high filling pressures. Therefore, excessive use of diuretics may diminish venous return and further impair cardiac output. This is especially critical in right ventricular heart failure. Heart Failure diuretic use becomes necessary to reduce the accumulation of edema, particularly in the lungs. Reduction of preload can reduce the size of the heart, allowing it to work at a more efficient fiber length. Edema associated with heart failure is generally managed with loop diuretics. In some instances, salt and water retention may become so severe that a combination of thiazides and loop diuretics is necessary. In treating the heart failure patient with diuretics, it must always be remembered that cardiac output in these patients is being maintained in part by high filling pressures. Therefore, excessive use of diuretics may diminish venous return and further impair cardiac output. This is especially critical in right ventricular heart failure. Heart Failure Diuretic-induced volume contraction predictably reduces venous return and can severely compromise cardiac output Diuretic-induced metabolic alkalosis is another adverse effect that may further compromise cardiac function. This complication can be treated with replacement of K+ and restoration of intravascular volume with saline; however, severe heart failure may preclude the use of saline even in patients who have received excessive diuretic therapy. In these cases, adjunctive use of acetazolamide helps to correct the alkalosis. Another serious toxicity of diuretic use, particularly in the cardiac patient, is hypokalemia. Hypokalemia can exacerbate underlying cardiac arrhythmias and contribute to digitalis toxicity. This can usually be avoided by having the patient reduce Na+ intake, thus decreasing Na+ delivery to the K+-secreting collecting tubule. Patients who are noncompliant with a low Na+ diet must take oral KCl supplements or a K+-sparing diuretic. Kidney Disease Although some renal disorders cause salt wasting, most kidney diseases cause retention of salt and water. When renal failure is severe (GFR < 5 mL/min), diuretic agents are of little benefit, because glomerular filtration is insufficient to generate or sustain a natriuretic response. However, a large number of patients, and even dialysis patients, with milder degrees of renal insufficiency (GFR of 5–15 mL/min), can be treated with diuretics when they retain excessive volumes of fluid between dialysis treatments. Certain forms of renal disease, particularly diabetic nephropathy, are frequently associated with development of hyperkalemia at a relatively early stage of renal failure Kidney Disease Patients with renal diseases leading to the nephrotic syndrome often present complex problems in volume management. These patients may exhibit fluid retention in the form of ascites or edema but have reduced plasma volume due to reduced plasma oncotic pressures. This is very often the case in patients with "minimal change" nephropathy. In these patients, diuretic use may cause further reductions in plasma volume that can impair GFR and may lead to orthostatic hypotension. Most other causes of nephrotic syndrome are associated with primary retention of salt and water by the kidney, leading to expanded plasma volume and hypertension despite the low plasma oncotic pressure. In these cases, diuretic therapy may be beneficial in controlling the volume-dependent component of hypertension. Kidney Disease In choosing a diuretic for the patient with kidney disease, there are a number of important limitations. Acetazolamide must usually be avoided because it can exacerbate acidosis. Potassium-sparing diuretics may cause hyperkalemia. Thiazide diuretics were previously thought to be ineffective when GFR falls below 30 mL/min. More recently, it has been found that thiazide diuretics, which are of little benefit when used alone, can be used to significantly reduce the dose of loop diuretics needed to promote diuresis in a patient with GFR of 5–15 mL/min. Thus, high-dose loop diuretics (up to 500 mg of furosemide/d) or a combination of metolazone (5–10 mg/d) and much smaller doses of furosemide (40–80 mg/d) may be useful in treating volume overload in dialysis or predialysis patients. Finally, there has been some interest in the use of osmotic diuretics such as mannitol, because this drug can shrink swollen epithelial cells and may theoretically reduce tubular obstruction. Unfortunately, there is no evidence that mannitol can prevent ischemic or toxic acute renal failure. Mannitol may be useful in the management of hemoglobinuria or myoglobinuria. Lastly, although excessive use of diuretics can impair renal function in all patients, the consequences are obviously more serious in patients with underlying renal disease. Hepatic Cirrhosis When ascites and edema become severe, diuretic therapy can be very useful. However, cirrhotic patients are often resistant to loop diuretics because of decreased secretion of the drug into the tubular fluid and because of high aldosterone levels. In contrast, cirrhotic edema is unusually responsive to spironolactone and eplerenone. The combination of loop diuretics and an aldosterone receptor antagonist may be useful in some patients. It is important to note that, even more than in heart failure, overly aggressive use of diuretics in this setting can be disastrous. Vigorous diuretic therapy can cause marked depletion of intravascular volume, hypokalemia, and metabolic alkalosis. Hepatorenal syndrome and hepatic encephalopathy are the unfortunate consequences of excessive diuretic use in the cirrhotic patient. Nonedematous States Hypertension The diuretic and mild vasodilator actions of the thiazides are useful in treating virtually all patients with essential hypertension and may be sufficient in many. Loop diuretics are usually reserved for patients with renal insufficiency or heart failure. Moderate restriction of dietary Na+ intake (60–100 mEq/d) has been shown to potentiate the effects of diuretics in essential hypertension and to lessen renal K+ wasting. A recent very large study (over 30,000 participants) has shown that inexpensive diuretics like thiazides result in similar or superior outcomes to those found with ACE inhibitor or calcium channel-blocker therapy. This important result reinforces the importance of thiazide therapy in hypertension. Although diuretics are often successful as monotherapy, they also play an important role in patients who require multiple drugs to control blood pressure. Diuretics enhance the efficacy of many agents, particularly ACE inhibitors. Patients being treated with powerful vasodilators such as hydralazine or minoxidil usually require simultaneous diuretics because the vasodilators cause significant salt and water retention. Nephrolithiasis Approximately two thirds of kidney stones contain Ca2+ phosphate or Ca2+ oxalate. Many patients with such stones exhibit a defect in proximal tubular Ca2+ reabsorption that causes hypercalciuria. This can be treated with thiazide diuretics, which enhance Ca2+ reabsorption in the distal convoluted tubule and thus reduce the urinary Ca2+ concentration. Salt intake must be reduced in this setting, since excess dietary NaCl will overwhelm the hypocalciuric effect of thiazides. Calcium stones may also be caused by increased intestinal absorption of Ca2+, or they may be idiopathic. In these situations, thiazides are also effective, but should be used as adjunctive therapy with other measures. Hypercalcemia Hypercalcemia can be a medical emergency. Because loop diuretics reduce Ca2+ reabsorption significantly, they can be quite effective in promoting Ca2+ diuresis. However, loop diuretics alone can cause marked volume contraction. If this occurs, loop diuretics are ineffective (and potentially counterproductive) because Ca2+ reabsorption in the proximal tubule would be enhanced. Thus, saline must be administered simultaneously with loop diuretics Potassium chloride may be added to the saline infusion as needed. Diabetes Insipidus Diabetes insipidus is due either to deficient production of ADH (neurogenic or central diabetes insipidus) or inadequate responsiveness to ADH (nephrogenic diabetes insipidus). Administration of supplementary ADH or one of its analogs is effective only in central diabetes insipidus. Thiazide diuretics can reduce polyuria and polydipsia in both types of diabetes insipidus. This seemingly paradoxic beneficial effect is mediated through plasma volume reduction, with an associated fall in GFR rate, enhanced proximal reabsorption of NaCl and water, and decreased delivery of fluid to the downstream diluting segments. Thus, the maximum volume of dilute urine that can be produced is lowered, and thiazides can significantly reduce urine flow in the polyuric patient. Dietary sodium restriction can potentiate the beneficial effects of thiazides on urine volume in this setting. Lithium (Li+), used in the treatment of manic-depressive disorder, is a common cause of nephrogenic diabetes insipidus and thiazide diuretics have been found to be helpful in treating it. Serum Li+ levels must be carefully monitored in these patients, because diuretics may reduce renal clearance of Li+ and raise plasma Li+ levels into the toxic range (see Chapter 29). Lithium-induced polyuria can also be partially reversed by amiloride, which blocks Li+ entry into collecting duct cells, much as it blocks Na+ entry.