Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
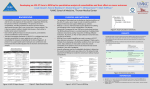
KLIMOP: a cohort study on the wellbeing of older cancer patients Laura Deckx Liesbeth Daniels, Katherine Nelissen, Piet Stinissen, Paul Bulens, Loes Linsen, Jean-Luc Rummens, Doris van Abbema, Franchette van den Berkmortel, Hans Wildiers, Vivianne C. Tjan-Heijnen, Marjan van den Akker, Frank Buntinx Klimop • Klimop was conceptualised by Prof. Buntinx and Dr. Bulens after a study performed by LIKAS in 2007 among stakeholders • “Cancer in Limburg: Challenges and strategic options for a coordinated approach “ • This study showed that the challenges in cancer care will be: – The psychosocial aspects of cancer care – Scientific research for older cancer patients Survival: quantity or quality? • Survival: quantity – Survival of cancer patients increases – Not for older cancer patients: EUROCARE project (Quaglia 2009) • Survival: quality – The fear to loose autonomy > the fear to die (Jolly 2006) – Macmillan Listening Study: To study the impact of cancer on everyday life was defined as the top priority area for cancer research (Okamoto 2011) Klimop-study To assess the impact of cancer, ageing and their interaction on subsequent wellbeing of older cancer patients Comorbidity Functional status Depression Quality of life Inclusion (January 2011) Baseline 6 months 1 year Younger cancer patients 168 84 30 Older cancer patients 100 44 7 Older patients without cancer 157 84 25 Total interviewed 425 212 62 Lost to follow-up / 40 4 Deceased / 14 3 ... Comorbidity Functional status Depression Quality of life Comorbidity • Comorbidity: the co-occurence of different diseases • Comorbidity is an enormous problem (Marengoni 2011) – Highly prevalent (55% - 98%) – Cause of disability, functional impairment, low Qol, high health care costs – Survival Comorbidity Number of chronic diseases (additional to cancer) 30 25 20 % 15 10 5 0 0 1 Cancer patients (60+) 2 3 ≥4 Non-cancer patients (60+) Guidelines to for the treatment of cancer patients with comorbidity are lacking! (Signaleringscommissie Kanker van KWF Kankerbestrijding 2011) Comorbidity Functional status Depression Quality of life Functional status • Maintenance of independence is very important • Associated with survival • Cancer patients have more functional problems (Hewitt 2003, Keating 2005) • Little prospective studies that investigate the risk factors for functional decline in older cancer patients → Cave! Selection of participants Functional status* : Baseline ~ 6 months Worse Idem Better Baseline N (%) N (%) N (%) Impaired 16 (10%) 39 (46%) 37 (44%) 8 (10%) Not impaired 152 (90%) 12 (27%) 21 (48%) 11 (25%) 17 (20%) 53 (63%) 14 (17%) Younger cancer patients Older cancer patients Impaired 23 (23%) Not impaired 77 (77%) Older patients without cancer Impaired 45 (19%) Not impaired 112 (71%) *Functional status (ADL en IADL): Computed as described by Kellen et al. 2010 Baseline Functional status* ~ Loneliness Impaired Not impaired N N OR 95% CI 2.2 0.6 – 7.8 4.4 1.4 – 14.0 1.2 0.6 – 2.5 Younger cancer patients Lonely 27 (18%) 4 23 Not lonely 124 (82%) 9 115 Lonely 26 (35%) 10 16 Not lonely 48 (65%) 6 42 Lonely 56 (38%) 17 39 Not lonely 91 (62%) 24 67 Older cancer patients Older patients without cancer *Functional status (ADL en IADL): Computed as described by Kellen et al. 2010 Comorbidity Functional status Depression Quality of life Depression • Depression is important: – Leading cause of disability worldwide – Commonly coexists – Predicts overall survival (Kanesvaran 2011 JCO) • Depression decreased – overall survival increased! (Giese-Davis 2011 JCO) • Results are inconclusive Depression: Baseline ~ 6 months Worse (>10%) Idem Better (>10%) Baseline N (%) N (%) N (%) 12 (8%) 11 (15%) 44 (59%) 20 (27%) 5 (18%) 18 (64%) 5 (18%) 8 (11%) 51 (71%) 13 (18%) Younger cancer patients Depressive feelings No depressive feelings 139 (92%) Older cancer patients Depressive feelings 11 (14%) No depressive feelings 66 (86%) Older patients without cancer Depressive feelings 18 (12%) No depressive feelings 133 (88%) Baseline Depression ~ Loneliness GDS-15 ≥5 GDS-15 <5 N N OR 95% CI 4.8 1.3 – 17.1 8.6 1.6 – 45.2 9.9 2.7 – 36.4 Younger cancer patients Lonely 25 (17%) 5 20 Not lonely 120 (83%) 6 114 Lonely 25 (35%) 7 18 Not lonely 46 (65%) 2 44 Lonely 55 (38%) 14 41 Not lonely 90 (62%) 3 87 Older cancer patients Older patients without cancer Comorbidity Functional status Depression Quality of life Quality of life • What is the impact of cancer, cancer treatment, ageing and their interaction on Qol? – Results are inconclusive • Methodological shortcomings (Joly 2007) – Cross-sectional – Presentation of mean values! – Prospective but Qol measured only once – Selection of patients Global Qol: Baseline ~ 6 months Worse (>10%) Idem Better (>10%) N (%) N (%) N (%) 31 (38%) 15 (19%) 35 (43%) 18 (55%) 8 (24%) 7 (21%) 17 (21%) 35(43%) 30 (37%) Younger cancer patients Global Qol Older cancer patients Global Qol Older patients without cancer Global Qol Comorbidity Functional status Depression Quality of life Wellbeing Little is known about the Comorbidity Functional status interaction between the co-occurrence of - Comorbidity Depression Quality of life - Functional impairment - Geriatric syndromes (Koroukian 2011 JCO) Preliminary conclusions • Results are preliminary and cross-sectional! The longer the duration of the study, the more valuable the results will be • Loneliness and depression are frequent and important factors that can be influenced • Guidelines for care of cancer patients with multimorbidity are needed, taking into account: – Co-morbidity/functional impairment/… – Consequences of cancer treatment – Collaboration between different disciplines in primary and secondary care Take home message • Be critical! – Was the study population appropriate? – Cross-sectional design versus prospective design? • Older cancer patients – Heterogeneous group – Specific health care needs • Quality rather than quantity of survival – Which factors determine maintenance or decline of wellbeing? “Knowing is not enough; we must apply. Willing is not enough; we must do.” Goethe KLIMOP is funded by VLK, the Flemisch League against Cancer and Interreg IV cross-border region Flanders – the Netherlands Contact: [email protected] [email protected] [email protected] www.ouderenenkanker.be Deckx L, Van Abbema D, Nelissen K, Daniels L, Stinissen P, Bulens P, Linsen L, Rummens JL, Van den Berkmortel F, Robaeys G, De Jonge E, Houben B, Pat K, Walgraeve D, Spaas L, Verheezen J, Verniest T, Goegebuer A, Wildiers H, Tjan-Heijnen V, Buntinx F, Van den Akker M. Study protocol of KLIMOP: a cohort study on the wellbeing of older cancer patients in Belgium and the Netherlands. BMC Publ Health 2011; 11: 825