Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Comorbidity-Adjusted Life Tables: A
Tool for Assessing Other Causes
Mortality in Cancer Patients
Angela Mariotto, Zhuoqiao Wang, Carrie Klabunde, Eric
J. Feuer
Methods and Applications for Population Based Survival
Frascati, September 20-21, 2010
Outline
Background motivation
Data: SEER, SEER-Medicare and 5% non-cancer sample
Methods
Step I: Estimating comorbidity index
Step II: Estimating survival by comorbidity index
Step III: Estimating health-adjusted age
Results
Discussion
Motivation
More accurate estimate of competing non-cancer survival taking into
account health status.
Tool to improve informed decisions regarding:
Treatment choices.
Age to stop screening.
SEER Data
The Surveillance, Epidemiology, and End Results (SEER)program
collects data on clinical, demographic, and cause of death information
for persons with cancer.
Data from 11 registries (1992-2005)
Representing 14 % of the US population
Medicare Program
Federal health insurance plan that offers health insurance for the 65
years and older US population.
Medicare data contains enrollment and “claims data” associated with
health care paid by Medicare plan.
Hospitalization, clinic visit, outpatient tests bills
Information on date, diagnosis codes, procedure codes, and cost.
94% of the 65 years and older US population has inpatient and
outpatient coverage
SEER-Medicare and the 5% Sample Data
SEER-Medicare: Medicare claims linked to Medicare eligible cancer
patients in the SEER database
There is a 93% match
5% sample (non-cancer): At the time of the linking, NCI creates a file
that contains claims, demographic characteristics and life status
information for a 5 % random sample of Medicare beneficiaries residing
in the SEER areas who do not have cancer.
The 5% non-cancer sample can be used as controls
Medicare claims data is the same for cancer and non-cancer cases
Measuring Comorbidity in SEER-Medicare: Cancer
Patients
SEER-Medicare: ICD-9-CM codes recorded in claims during the 12
months prior to the cancer diagnosis were used to identify 16
comorbid conditions used by Charlson et al. (J. Chronic Disease,
1987).
Algorithm similar to Klabunde et al. (Annals of Epidemiology, 2007)
Survival time
Cancer
diagnosis
X
1 year prior, claims
are evaluated to
indentify 16 comorbid conditions
Non-cancer
death
●
Measuring Comorbidity in the 5% Sample Data: NonCancer
Comorbidity identified prior to each birthday
Multiple records for each person but each record contributes to 1
survival curve
Same algorithm as for cancer patients
69 survival
…
66
Birthday
67
Birthday
68
Birthday
69
Birthday
X
X
X
X
Claims are evaluated to indentify 16
conditions prior to each birthday
67 survival
66 survival
End of follow-up
Data characteristics: Age, Sex, Race and Life
Status
SEER- Medicare Cancer
Patients
No.
%
Age
5% sample (non-cancer)
Multiple records
No.
%
66-69
70-74
75-79
80-84
85-89
90+
211,849
293,324
269,384
188,485
99,993
45,050
19
26
24
17
9
4
673,786
821,570
689,356
486,045
273,705
155,371
22
27
22
16
9
5
Sex Females
Males
524,625
583,460
47
53
1,966,271
1,133,562
63
37
978,633
79,921
49,531
88
7
4
2,639,759
223,353
236,721
85
7
8
81
19
100
2,249,854
849,979
3,099,833
73
27
100
Race
Life Status
White
Black
Other
Alive 897,368
Dead 210,717
Total 1,108,085
Comorbidities Frequencies
SEER-Medicare
Cancer Patients
Multiple records
%
1.3
0.0
5.9
2.1
9.6
15.3
1.5
15.5
3.0
0.6
0.2
2.0
0.7
2.0
1.8
4.3
No.
30,653
430
159,874
43,948
207,307
277,638
60,806
408,201
80,461
7,475
2,407
44,584
19,456
59,259
37,923
101,248
%
1.0
0.0
5.2
1.4
6.7
9.0
2.0
13.2
2.6
0.2
0.1
1.4
0.6
1.9
1.2
3.3
No Comorbidity
665,135 60.0
2,125,944
68.6
Total
1,108,085 100.0
3,099,833
100.0
Acute myocardial infarction
AIDS
Cerebrovascular disease
Chronic renal failure
Congestive heart failure
COPD
Dementia
Diabetes
Diabetes with sequelae
Liver disease mild
Liver disease mod/severe
Myocardial infarction
Paralysis
Rheumathologic disease
Ulcer disease
Vascular Disease
No.
14,466
279
65,711
22,952
106,067
169,780
16,305
171,688
33,743
6,430
2,171
22,270
8,000
22,606
20,218
47,195
5% sample (non-cancer)
Step I: Estimating the Comorbidity Index
SEER-Medicare data on cancer patients only
Cancer patients with more than one cancer are excluded
Comorbid conditions measured in the year prior to diagnosis
Cox proportional hazard method having sex, age, race and 16
conditions
Event: death for non-cancer causes
Censoring events: cancer death and lost or end of follow-up
Results from Cox proportional hazards model
Variable
Estimate
Std.Err.
Hazard
Ratio
0.09
0.000
1.1
Age
Female
Male
Race: White
Black
Other
0.23
0.004
1.3
0.15
-0.09
0.008
0.011
1.2
0.9
Acute myocardial infarction
AIDS
Cerebrovascular disease
Chronic renal failure
Congestive heart failure
COPD
Dementia
Diabetes
Diabetes with sequelae
Liver disease
Liver disease mod./severe
Myocardial infarction
Paralysis
Rheumathologic disease
Ulcer disease
Vascular Disease
0.15
0.54
0.35
0.68
0.74
0.56
0.72
0.34
0.24
0.87
0.66
0.06
0.38
0.26
0.09
0.31
0.015
0.154
0.008
0.012
0.006
0.006
0.013
0.006
0.012
0.026
0.042
0.014
0.020
0.014
0.014
0.009
1.2
1.7
1.4
2.0
2.1
1.8
2.1
1.4
1.3
2.4
1.9
1.1
1.5
1.3
1.1
1.4
Comorbidity Index Calculation (CI)
1. Diabetes + Congestive heart
failure
CI=0.34+0.74=1.08
2. Diabetes + COPD
CI=034+0.56=0.88
3. COPD+ Congestive heart failure
+ Liver:
CI= 0.56+0.74+0.87= 2.17
Step II: Estimating age- and sex- specific survival by
comorbidity index
Both data: SEER-Medicare and 5% non-cancer sample
For each age and sex we fit a Cox proportional hazard model using
comorbidity Index as cubic-spline linear at the tails, cancer status, and
race as covariates
People in the 5% sample are included once in each survival curve
Step II: Estimating age- and sex-survival by
comorbidity index (continued)
For each age and sex we fit a Cox proportional hazard model where z is a vector of
covariates
Sage,sex (t | z) Sage,sex (t )
exp( βz )
βz 00 01 cancer 02 black 03 Other race CI spline
Comorbidity index (CI) is modeled with a restricted cubic spline with 4 knots at the 5%,
35% , 65% and 95% percentile of each individual age : k1, k2 k3, and k4.
CI spline 10 CI 11 CI1 12 CI 2
where CI1 and CI2 are two function of CI and knots.
(CI k3 )3 (k4 k j ) (CI k4 )3 (k4 k j )
CI j (CI k j )
, j 1, 2. u
(k4 k3 )
(k4 k3 )
0 if u 0
u if u 0
Parameters Estimates
Set of 7 parameters for each age (66-95) and sex (males and females)
Summarize parameters graphically
Hazard ratios of dying of other causes by age due to:
Diabetes vs. healthy
Cancer vs. non cancer
Race
For selected ages we show the effect of comorbidity index on the risk of
dying of other causes for white women.
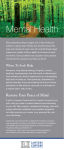
Hazard ratio estimates of dying of other causes than cancer due to
diabetes (CI=0.34)
3.0
3.0
Males
2.5
2.5
2.0
2.0
Relative Risk
Hazard Ratio
Females
Comorbidity:
Diabetes CI=0.34
1.5
1.0
1.5
1.0
0.5
0.5
0.0
0.0
65
75
85
Age
95
Comorbidity:
Diabetes CI=0.34
65
75
85
Age
Reference is whites, no-comorbidities and no-cancer: Hazard Ratio=1
95
Hazard ratio estimates of dying of other causes than cancer due to
diabetes (CI=0.34), race and cancer status.
3.0
3.0
Males
2.5
2.5
2.0
2.0
Relative Risk
Hazard Ratio
Females
Comorbidity:
Diabetes CI=0.34
Cancer
1.5
1.0
1.5
0.5
0.0
0.0
75
85
Age
95
Cancer
1.0
0.5
65
Comorbidity:
Diabetes CI=0.34
65
75
85
Age
Reference is whites, no-comorbidities and no-cancer: Hazard Ratio=1
95
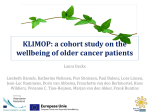
Hazard ratio estimates of dying of other causes than cancer due to
diabetes (CI=0.34), race and cancer status.
3.0
3.0
Males
2.5
2.5
2.0
2.0
Relative Risk
Relative Risk
Females
Comorbidity:
Diabetes CI=0.34
Cancer
1.5
Black
1.0
Other race
0.5
Comorbidity:
Diabetes CI=0.34
1.5
Cancer
1.0
Other race
0.5
0.0
Black
0.0
65
75
85
Age
95
65
75
85
Age
Reference is whites, no-comorbidities and no-cancer: Hazard Ratio=1
95
Estimating Health-Adjusted Age or Physiologic Age
Motivation: usually doctors subjectively assign a physiological age to
patients depending on their health status and health behaviors
People in good health and with healthy: lower physiological age
People in poor health: higher physiological age
By comparing each age and comorbidity specific survival curve with US
life tables we will more “objectively” try to calculate physiological age
Life tables represent all causes mortality in the US population.
Estimating health-adjusted age: physiologic age
Example: White women age 66 with no comorbidity
S66,CI 0 (t )
P(t | x)
is the estimated cumulative probability of surviving age t for a white
women diagnosed with cancer at age 66 and no comorbidities
P (t )
is the cumulative probability of surviving age t obtained from the 2000
life tables for white women in the US
P(t )
P( x)
is the cumulative probability of surviving age t, conditional on being
alive at age x.
Health- Adjusted age is the age x that minimizes distance between S66,CI 0 (t ) and P(t | x)
10
min{ 50 x75 } | S66 ,CI 0 ( t ) P( t | x )| .
t 1
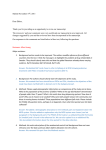
White women diagnosed with cancer at 70 years of age and selected
comorbidity indexes (solid) to the best fitted US life table (dashed lines).
1
US LT Age=65
Age=70, Comorb.=0
0.8
Proportion surviving
US LT, Age=70
Age=70, Comorb.=0.2
0.6
US LT Age=76
Acute myocardial
infarction
COPD
Age=70, Comorb.=0.5
0.4
US LT, Age=83
Age=70, Comorb.=1.0
Diabetes + COPD,
Diabetes+ CHF
0.2
US LT Age=88
Dementia + COPD +CHF
US LT Age=92
Age=70, Comorb.=1.5
Age=70, Comorb.=2.0
0
0
2
4
6
Years
8
10
Diabetes + COPD
+ CHF
Limitations
Comorbidities measured from claims data
Estimates for ages 66+ only
2 step analysis:
Cancer patients to estimate comorbidity index
Cancer patients + cancer free people to estimate survival by
comorbidities
In one analysis we would have to take into account of the correlation
of comorbidities before consecutive birthdays on the cancer free
population
Discussion and Conclusions
Comorbidity, cancer status, sex and race are important predictors of
other cause mortality, however their effect is attenuated as age
increases.
Not clear why cancer status is a predictor of worse other causes
survival
Misclassification of cause of death?
Future analysis: restrict analysis to women with early breast cancer
and do matching with 5% cancer random sample to investigate if
their other causes survival is still worse.
Discussion and Conclusions
This tool will paired with cancer prognosis (net cancer survival) to
provide more individualized probabilities of dying from cancer and of
dying of other causes
Inclusion of other cause mortality in decision of cancer treatment
and screening are particularly important for patients diagnosed at
older ages and with more indolent tumors (e.g. prostate cancer)
Health-adjusted age might be a useful tool for clinicians in general
One Dataset
Cox
Model 1
Net probability
of dying of
Cancer
Cox
Model 2
Net probability
of dying of
Other Causes
Dataset 1
Cancer Patients
Cox
Model 1
Net probability
of dying of
Cancer
Dataset 2
Non-cancer
Cox
Model 2
Net probability
of dying of
Other Causes
Equations are the same
Crude probabilities dying of Cancer
and Other Causes
No need for independence assumption
Minjung used a continuous time model where
estimates are computed using counting
process*
Estimates and SE’s of cumulative incidence
are identical if independence is assumed or
not (Nonidentifiability: Tsiatis,1975)
*Cheng SC, Fine JP, Wei LJ, “Prediction of the Cumulative
Incidence Function under the Proportional Hazards Model”,
Biometrics, 54, 1998.
Crude probabilities dying of Cancer
and Other Causes
Needs independence assumption of
competing risk and that populations are
similar*
Can take advantage of the richness of
alternative different data sources.
Use discrete time model – CI’s of cumulative
incidence computed using delta method
Thank you!!!
Villa Mondragone