Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
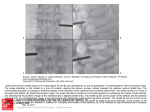
MORPHOLOGY OF MIDDLE AND LOWER CERVICAL PEDICLES *Shin, E; +*Panjabi, M (A-NIH); *Chen, N; *Wang, J +*Yale University School of Medicine, New Haven, CT. Yale University School of Medicine, Dept. of Orthopaedics and Rehabilitation, Biomechanics Research Laboratory, P.O. Box 208071, New Haven, CT 06520-8071, (203) 785-2812, Fax: (203) 785-7069, [email protected] Results Superior and inferior wall cortical thicknesses were found to be similar (mean value ranges for both: 1.5-2.4 mm). The medial cortical shell (mean value range: 1.2-2.0 mm) was measured to be 1.4 to 3.6 times as thick as the lateral cortical shell (mean value range: 0.4-1.1 mm) across all pedicle thin slices and vertebral levels (Fig. 1B). The external shape of the cervical pedicle was observed to be more elliptical than that of the cancellous core, which tended to be more circular (Fig. 2). Graphical comparisons of thin slices from C3 to C5 demonstrated that the cervical pedicle was semicircular, rectangular, or even triangular on cross section (Fig. 3). Large variability was observed not only between individual spines and vertebral levels, but also along the pedicle axis. The cancellous core in such specimens ranged from being finely trabeculated to nearly absent. These variabilities were reflected in the large standard deviations of our measurements. Thin slices from C6 and C7 exhibited greater uniformity in size and an ovoid shape, with the slices becoming narrower as the slices progressed antero-posteriorly along the pedicle long axis. Discussion The lateral cortex was significantly thinner than the medial cortex in all thin slices and at all vertebral levels. The lateral cortex of cervical pedicles is responsible for protecting the vertebral artery, with the exception of C7 pedicles. Thus, extreme caution must be exercised when inserting pedicle screws so as not to perforate the thin lateral cortex of the cervical pedicle. The extensive variability in pedicle morphometry must also be recognized as the standard deviations for measured pedicle dimensions were found to be large. Graphical representations of the pedicle demonstrated its complexity as a three-dimensional structure whose features, with respect to cortical thickness, orientation, and overall shape, changed as the slices progressed anteroposteriorly. Characteristics of the cervical pedicle at different spinal levels must be carefully noted prior to transpedicular screw fixation to avoid cortical wall violations. Our data shows that the effective diameter which would permit a given screw size is much less than one would expect on the basis of simple measurements of pedicle height and width. CCW CTM mm CTS CCH PDH PDW CCW CTL CTM 6.0 4.0 2.0 Cancellous Core 0.0 C3 Cortical Shell A C4 C5 C6 Vertebral Level C7 B Figure 1. Measured dimensions included: pedicle height (PDH) and width (PDW); cortical shell thicknesses for the superior (CTS), inferior (CTI), lateral (CTL), and medial walls (CTM); and the cancellous core height (CCH) and width (CCW). 2.5 1.58 1.59 2.0 Ratio Methods Twenty-six human cervical vertebrae (C3-C7) were secured to a thin sectioning machine to produce three 0.7 mm-thick pedicle slices along its axis. The first slice was made at the isthmus of the pedicle. To document variation along the pedicle axis, two additional slices were obtained: one anteriorly and another posteriorly to the first slice. Plain film radiographs of the pedicle slices were scanned and digitized to facilitate measurement of the internal dimensions. Computer software was specifically developed to determine the external dimensions (i.e. pedicle height and width) and the internal dimensions (i.e. cortical shell thicknesses of the superior, inferior, lateral, and medial walls, and the cancellous core height and width) of cervical pedicles (Fig. 1A). 8.0 PDW CTL CTI Introduction Transpedicular screw fixation is one of the most sophisticated procedures currently being used to stabilize the cervical spine. Anatomic studies have documented the external dimensions and angular parameters of the cervical pedicle, thereby providing the spinal surgeon with relevant information for accurate pedicle screw insertion [1,2]. Data is lacking, however, regarding its internal architecture and cortical shell thickness along the pedicle axis. It has been shown that screw stability and pull-out strength depend largely on the internal characteristics of the pedicle, not on its external dimensions [3]. The purpose of this study is two-fold: 1) To quantify the internal dimensions and cortical shell thicknesses of middle and lower cervical pedicles, and 2) To provide comparative graphical data which would document the variability in pedicle morphology. Our aim is to improve the percentage of successful surgical outcomes while minimizing risk to the patient. 1.33 1.28 1.23 1.5 1.0 0.5 CCH/ CCW 1.50 1.16 PDH/ PDW 1.03 1.05 C5 C6 1.05 0.0 C3 C4 C7 Vertebral Level Figure 2. Ratio of pedicle height to pedicle width and cancellous core height to cancellous core width. Elliptical shapes above and below the graph are proportional to the mean values shown at each vertebral level. Superior Lateral Medial Inferior Figure 3. Sample bitmapped digitized images of C5 left pedicle slices. The extensive variability in pedicle shape is observed in these slices. References 1. Karaikovic EE, Daubs MD, Madsen RW, Gaines RW. Morphologic characteristics of human cervical pedicles. Spine 1997:22:493-500. 2. Panjabi MM, Duranceau J, Goel VK, Oxland T, Takata K. Cervical human vertebrae: Quantitative three-dimensional anatomy of the middle and lower regions. Spine 1991;16:861-9. 3. Hirano T, Hasegawa K, Takahashi H, et al. Structural characteristics of the pedicle and its role in screw stability. Spine 1997;22:2504-10. Acknowledgement Funded by NIH Grant AR-42211. Poster Session - The Spine - VALENCIA FOYER 46th Annual Meeting, Orthopaedic Research Society, March 12-15, 2000, Orlando, Florida 0383