Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
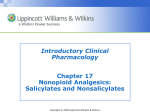
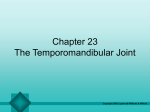
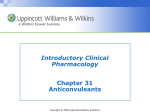
Chapter 22 The Ankle and Foot Copyright 2005 Lippincott Williams & Wilkins Osteology Talocrural Joint Distal fibula Tibia Talus Midfoot Navicular Cuboid 3 cuneiform bones Forefoot 5 metatarsals Phalanges Copyright 2005 Lippincott Williams & Wilkins Osteology of Foot and Ankle Copyright 2005 Lippincott Williams & Wilkins Ligaments of Talocrural (TCJ), Subtalar (STJ) and Midtarsal Joints (MTJ) Copyright 2005 Lippincott Williams & Wilkins Muscles of the Foot and Ankle Anterior Anterior tibialis Extensor hallucis longus Extensor digitorum longus Peroneus tertius Open Chain Action Dorsiflexion/inversion Extension of phalanges – 1st ray Extension of phalanges – toes Everts foot Copyright 2005 Lippincott Williams & Wilkins Muscles of the Foot and Ankle (cont.) Lateral Compartment Peroneus longus Peroneus brevis Posterior Open Chain Action Eversion Copyright 2005 Lippincott Williams & Wilkins Muscles of the Foot and Ankle Posterior Gastrocnemius Soleus Plantaris Deep Posterior tibialis Flexor hallucis longus Flexor digitorum longus Open Chain Action Plantar flexion Plantar flexion Plantar flexion Plantar flexion and inversion First ray flexion Flexion – Phalanges of toes Copyright 2005 Lippincott Williams & Wilkins Innervation (Superficial) Copyright 2005 Lippincott Williams & Wilkins Talocrural/Subtalar/Midtarsal Joints Function: Shock absorption Absorb lower extremity rotatory forces Provide lever for effective propulsion Copyright 2005 Lippincott Williams & Wilkins Pronation/Supination Pronation Movement in the direction of eversion, abduction and dorsiflexion. Supination Movement toward inversion, adduction, and plantar flexion. Copyright 2005 Lippincott Williams & Wilkins Pronation/Supination Copyright 2005 Lippincott Williams & Wilkins Talocrural – Pronates (dorsiflexion most dominant with eversion and abduction) – Supinates (dominated most by plantar flexion with inversion and adduction) Subtalar – Closed chain pronation (calcaneus everts, talus adducts and flexes) – Closed chain supination (calcaneus inverts, talus adducts and dorsiflexes) Copyright 2005 Lippincott Williams & Wilkins Midtarsal Joint (MTJ) Subtalar pronation – Promotes mobility in MTJ and forefoot. Subtalar supination – Promotes stability in MTJ and forefoot. Copyright 2005 Lippincott Williams & Wilkins Locking and Unlocking of Midtarsal Joint Copyright 2005 Lippincott Williams & Wilkins Kinetics and Kinematics of Gait Cycle Phase Joint ROM Moment Muscle Activity Contraction Type Initial TCJ O° DF Plantar flexion Dorsiflexors Isometric STJ Supination Everters Isometrics TCJ Plantar flexes from 0–15° PF Plantar flexion Dorsiflexors Eccentric Moving to valgus Inverters Eccentric Plantarflexors Inverters Eccentric Eccentric – Concentric PlantarEccentric – flexors concentric Evertors Isometric Copyright 2005 Lippincott Williams & Wilkins Loading response STJ Starts pronating Midstance Terminal Stance TCJ 10° DF STJ Begins supination Moving to DF ValgusVarus TCJ 15° DF Dorsiflexion STJ Supinating Varus Kinetics and Kinematics of Gait Cycle (cont.) Phase Joint ROM Moment Muscle Activity Contraction Type Pre-swing TCJ 20° PF Dorsiflex STJ Remains supinated Varus Initial swing TCJ Dorsiflexes to 10° PF Dorsiflexors Dorsiflexors Midswing TCJ Dorsiflexes to 0° Dorsiflexors Dorsiflexors Terminal swing TCJ Stays at 0° Dorsiflexors Dorsiflexors Copyright 2005 Lippincott Williams & Wilkins Alignment Must be assessed from subtalar neutral position (neither pronated nor supinated). Subtalar joint assessed in both prone and weight-bearing positions. Forefoot and rearfoot alignment are evaluated separately. Copyright 2005 Lippincott Williams & Wilkins Ideal Rearfoot Alignment Copyright 2005 Lippincott Williams & Wilkins Alignment of Tibia, Foot, Ankle Sagittal Plane Plumbline alignment is slightly anterior to midline through knee and lateral malleolus. Navicular tubercle, line from medial malleolus to where MTP joint of great toe rests on floor. Frontal Plane Distal one third of tibia is in sagittal plane. Great toe is not deviated toward midline of foot. Toes are not hyperextended. Copyright 2005 Lippincott Williams & Wilkins Anatomic Impairments First ray hypermobility – Dorsal translation with soft endpoint. Subtalar varus – Inverted twist within body of calcaneus. Forefoot varus – Inversion deviation of forefoot relative to bisection of posterior calcaneus. Forefoot valgus – Eversion deviation of forefoot relative to bisection of posterior calcaneus. Copyright 2005 Lippincott Williams & Wilkins Forefoot Varus Copyright 2005 Lippincott Williams & Wilkins Forefoot Valgus Copyright 2005 Lippincott Williams & Wilkins Examination and Evaluation Patient/client history Balance Joint integrity and mobility Muscle performance Pain Posture Copyright 2005 Lippincott Williams & Wilkins ROM and Muscle Length Examination of knee, hip, ankle, and spine is essential! Hip and knee ROM and muscle length Calcaneal inversion and eversion ROM Midtarsal joint supination and pronation ROM First ray position and mobility Hallux dorsiflexion ROM 1st–5th ray mobility Ankle dorsiflexion and plantar flexion ROM with knee flexed and extended Copyright 2005 Lippincott Williams & Wilkins Therapeutic Exercise Intervention for Common Physiologic Impairments Balance Impairment Restoration requires positional sense (proprioception). Balance machine, balance board, external perturbation. Home Exercises Balancing on one leg with eyes open, progress to eyes closed in door frame. Standing on one leg on a pillow or couch cushion with eyes open, progress to eyes closed. Copyright 2005 Lippincott Williams & Wilkins Muscle Performance Intrinsic Muscles Patient flexes at proximal MTP joint before distal MTP joint. Draw towel under foot, pick up marbles. Using resistant bands to resist proximal MTP joint flexion. Extrinsic Muscles Resisted talocrural plantar flexion with slow eccentric return to talocrural dorsiflexed position. Closed chain exercises (double leg heel rises, etc.). Copyright 2005 Lippincott Williams & Wilkins Intrinsic Muscles/Extrinsic Muscles Copyright 2005 Lippincott Williams & Wilkins Pain Exercise initiated in pain-free range Soft tissue mobilization Cryotherapy NMES/TENS Exercise for neighboring regions Copyright 2005 Lippincott Williams & Wilkins Posture and Movement Impairment Excessive pronation and supination most common. Exercises developed from components of gait. Goal is to control motions in/out of static positions at varying speeds. Static weight shifting on bathroom scale. Forward/backward stepping. Circular weight-shifting drill. Functional drills (retrowalking, sidestepping, etc.). Copyright 2005 Lippincott Williams & Wilkins ROM, Muscle Length, Joint Integrity, Mobility Acute Phase Hypermobile segment should be protected (taping, bracing, casting, etc.). Adjacent hypomobile segments should be mobilized with manual therapy or mobility exercise. Dynamic stabilization exercise should be initiated at the hypermobile segment. Copyright 2005 Lippincott Williams & Wilkins ROM, Muscle Length, Joint Integrity, Mobility – Talocrural Joint Talocrural Dorsiflexion Gastrocnemius and soleus stretching (prevent subtalar pronation). TCJ dorsiflexion ROM (soleus stretch with talar joint in neutral or slightly supinated position. Step-down training to facilitate eccentric control of dorsiflexion. Copyright 2005 Lippincott Williams & Wilkins Subtalar Joint Full active/active-assisted supination can be performed. Pronation mobility active/active-assisted. Progressions involve functional training of new mobility in appropriate phase of gait cycle. Copyright 2005 Lippincott Williams & Wilkins Subtalar Pronation/Supination Copyright 2005 Lippincott Williams & Wilkins Therapeutic Exercise Intervention for Common Ankle and Foot Diagnoses Plantar Faciitis Overuse caused by excessive pronation. Treatment Decrease pain and inflammation, reduce tissue stress, restore muscle strength. NSAIDs, US, iontophoresis, massage – for pain. Taping, orthoses, modified footwear to reduce tissue stress. Copyright 2005 Lippincott Williams & Wilkins Plantar Faciitis – Treatment (cont.) If pronated Mobilize TCJ Stretch gastrocnemius and soleus Strengthen tibialis anterior and extensor digitorum Initiate functional and proprioceptive activities Copyright 2005 Lippincott Williams & Wilkins Posterior Tibial Tendon Dysfunction Usually excessive subtalar joint pronation and results in acquired foot deformity. Treatment NWB short leg casting may be necessary for 4–6 weeks (patients with partial tears). Medication and modalities for inflammation. Arch strapping to control end-range pronation. Pain-free, low-intensity, high-repetition open kinetic chain plantar flexion. Copyright 2005 Lippincott Williams & Wilkins Achilles Tendinosis Overuse pathology of Achilles tendon. Treatment Restore TCJ mobility Stretching is essential after TCJ mobility is restored. Strengthening exercises following inflammation recovery. Copyright 2005 Lippincott Williams & Wilkins Functional Nerve Disorders Assessment should include spine and hip involvement. Nerve involvement may resolve with shoe changes, orthotics, alteration of impairments in alignment, mobility, and movement pattern exercises. Affected nerves include: 1. 2. Tibial nerve Peroneal nerve Copyright 2005 Lippincott Williams & Wilkins Ligament Sprains 70–80% involve anterior talofibular ligament (ATFL), calcaneal fibular ligament (CFL), posterior talofibular ligament (PTFL). Grade III sprains are further classified: First degree – Complete rupture of ATFL Second degree – Complete rupture of ATFL and CFL Third degree – Dislocation in which ATFL, CFL, and PTFL are ruptured Copyright 2005 Lippincott Williams & Wilkins Ligament Sprains – Treatment Grade I–II, 1st 4 days – R.I.C.E. Severe grade I/II may need crutches in early stage. Open kinetic chain inversion ROM as tolerated. Progress as pain and swelling are controlled and weight-bearing tolerance increases. Grade III rehabilitation is similar to that of I and II. Copyright 2005 Lippincott Williams & Wilkins Ankle Fractures Supination adduction injury Supination external rotation injury Pronated abduction injury Pronated external rotation injury Treatment Edema massage, scar mobilization, edema reduction AROM begins mid-range, low intensity/high reps As function normalizes, ROM exercise is generally more tolerable Copyright 2005 Lippincott Williams & Wilkins Adjunctive Interventions Adhesive strapping Wedges and pads Biomechanical foot orthotics Heel and full sole lifts Copyright 2005 Lippincott Williams & Wilkins Summary Three main joints of ankle and foot are TCL, ST, MTL and subdivided into calcaneocuboid and talonavicular. Extrinsic muscles consist of anterior, lateral, posterior groups. Anterior-dorsiflexion, lateral – everters, posterior – plantar flexors. Functions of foot during gait are shock absorption, surface adaptation, and propulsion. Copyright 2005 Lippincott Williams & Wilkins Summary (cont.) Foot and ankle exam must be thorough and include relationships of lower joint extremities. Common anatomic impairments include subtalar varus, forefoot varus/valgus. Common physiologic impairments include loss of mobility, force, torque, balance, impaired balance, and posture. Adjunctive agents may be necessary to treat primary or secondary impairments. Copyright 2005 Lippincott Williams & Wilkins