Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
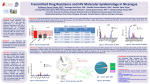
Prevalence and clinical implications of NRTIand NNRTI-associated minority variant drugresistance mutations in ARV-naïve patients with and without transmitted drug resistance IDWeek October 29th, 2016 Dana Clutter Stanford University School of Medicine Division of Infectious Diseases and Geographic Medicine Financial disclosures D Clutter: Bristol-Myers Squibb Virology Fellows Research Program Co-investigators: R Swanstrom: Co-inventor of Primer ID R Shafer: Research funding from Gilead Sciences, BristolMyers Squibb, Merck, and Vela Diagnostics Background Minority variants Limit of detection for drug resistance mutations (DRMs) by Sanger sequencing is 15-20% Additional low-abundance HIV-1 variants below Sanger threshold are “minority variants (MVs)” MVs require ultrasensitive methods for detection (allele-specific PCR, NGS) Clinical implications of pre-therapy MVs Prevalence of transmitted drug resistance (TDR) is ~10-20% An additional 10-20% of ART-naïve individuals harbor MVs bearing DRMs (MV-DRMs) MV-DRMs associated with increased virological failure (VF) Li et al. JAMA 2011; Panichsillapakit et al. JAIDS 2016; Rhee et al. PLOS Med Are patients with isolated NNRTI TDR at high risk of having MV-DRMs? NRTI DRMs occur commonly in combination with NNRTI DRMs during VF Following transmission of multiple DRMs, low-fitness DRMs decay M184V >> NNRTI DRMs > 215 revertants Several small uncontrolled studies have shown that patients with TDR frequently have MV-DRMs Jain et al. JID 2011; Castro et al. JID 2013; Toni et al. AAC 2009; Varghese et al. JAIDS 2009 Aim Determine if NRTI and NNRTI MVDRMs occur more commonly in individuals with isolated NNRTI TDR compared to those without Methods Study population ART-naïve Kaiser Permanente Northern California Baseline genotype (Sanger): 2004 – 2012 Cryopreserved plasma sample available HIV RNA >10,000 copies/mL Groups: TDR: consecutively sampled, isolated NNRTI DRM(s) Wild type (WT): matched by HIV RNA level, CD4 count, sampling year, and ART regimen where possible Primer ID-Illumina MiSeq sequencing Accurate quantification of MV-DRMs Distinguish MV-DRMs from technical artifact Zhou et al. J Virol 2015; Jabara et al. PNAS 2011; Keys et al. AIDS Res Hum Retrovirus 2015 Statistical analysis Definitions: MV-DRM: NNRTI or NRTI surveillance DRM detected only by Primer ID Illumina sequencing VF: HIV RNA > 50 copies/mL at week 48 Analysis: Compare proportions with MV-DRMs between groups Compare outcomes (VF, regimen change) between groups Describe outcomes when MV-DRMs conferred resistance to ART regimen (HIVDB v 7.0) Bennett et al. PLOS ONE 2009; HIVDB Results Baseline characteristics Characteristic WT n = 49 TDR n = 33 Age, median (IQR) Male, n (%) Race/ethnicity, n (%) White Black Hispanic Other Baseline log viral load, median (IQR) Baseline CD4 count, median (IQR) Initial anchor drug, n (%) RAL ATVr Other Initial NRTIs, n (%) FTC/TDF 3TC/ABC Other Sample year, median (IQR) 42 (35-49) 46 (94) 42 (34-46) 28 (85) 25 (51) 10 (20) 8 (16) 6 (12) 4.8 (4.3-5.2) 339 (128-403) 20 (61) 5 (15) 6 (18) 2 (6) 4.7 (4.5-5.1) 339 (218-466) 21 (43) 16 (33) 12 (24) 20 (61) 13 (39) 0 41 (84) 4 (8) 4 (8) 2010 (2006-2010) 31 (94) 1 (3) 1 (3) 2009 (2007-2011) MV-DRM prevalence and between-group comparisons P = 0.82 Overall 60% had MV-DRMs Abundance: 0.2 (0.1-0.6)% No between-group differences MV-DRMs conferred resistance to ART regimen in 10 individuals: P = 0.25 P = 0.65 Proportion P = 0.06 M184V/I: 7 G190E: 2 K65R: 1 Any NNRTI NRTI MV-DRM Pattern Both Group WT TDR Clinical outcomes Outcome Regimen change VF VF with emergent resistance WT n = 49 n (%) 13 (27) 5 (10) 1 (2) TDR n = 33 n(%) 3 (9) 3 (9) 0 P 0.09 1.00 1.00 1 of 10 with MV-DRMs conferring resistance to ART regimen developed VF: MV-DRM: M184V Regimen contained 3TC and ABC No repeat genotype available at VF Conclusions MV-DRMs common in this Northern California cohort MV-DRMs were not associated with isolated NNRTI TDR Despite high prevalence of MV-DRMs, responses to ART were favorable Acknowledgments Participants UNC Kaiser Permanente Northern California Shuntai Zhou Ronald Swanstrom Daniel Klein Jeffrey Fessel Leo Hurley Michael Silverberg Stanford Vici Vargese Soo-yon Rhee Robert Shafer Benjamin Pinsky This work was conducted with support from a KL2 Mentored Career Development Award of the Stanford Clinical and Translational Science Award to Spectrum (NIH KL2 TR 001083) and (UL1 TR 001085) Questions? Thank you!