Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
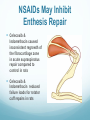
NSAID use in Athletes Gregory Cain, MD Activity, Exercise and Sports Medicine Group Health Physicians Credits to Trevor Bullock, DO my former mentor at Summa Disclosures I have no financial conflicts of interest A significant portion of this talk was borrowed with permission from Trevor Bullock, DO – former Summa staff sports medicine physician Dr. Bullock’s talk was updated with new relevant information post 2010 NSAIDs Overview NSAID History/Characteristics “Inflammation” Mechanism of Action COX enzymes NSAIDS vs Injuries of: Bone Ligament Muscle Tendon Side Effects Gastrointestinal Renal Cardiovascular Risk Prophylactic Misuse of NSAIDs Summary of Recommendations NSAIDs • NSAID’s are anti-inflammatory, analgesic, antipyretic • Aspirin has antithrombotic effects • NSAIDs are more efficacious than acetaminophen for OA across multiple recent trials • Previously Tylenol was recommended as first-line treatment for acute and chronic musculoskeletal pain, but recent evidence (NICE) shows it ineffective for back pain and no better than placebo for most knee osteoarthritis • NSAIDs and acetaminophen may be equivalent for the mildest forms of knee OA Inflammation Mechanism of Action Primarily inhibit the cyclooxygenase (COX) pathway COX-1 enzyme (constitutional) COX-2 enzyme (inducible) COX Enzymes • COX-1 – Found in most tissues and regulates normal cellular processes - constitutive • • • • • • • Gastric cell protection Vascular hemostasis Platelet aggregation Renal blood flow Ocular pressure Airway dilatation Parturition COX Enzymes • COX-2 – Undetectable in most tissues – Induced with an inflammatory response and is responsible for: • Sensitizing pain receptors • Elevating body temperature • Recruiting inflammatory cells toward areas of tissue injury • COX-3 (not functional in humans) – Active in dogs, not mice and humans due to a frame shift mechanism Broader Picture of the ARA Pathway Mechanism of Analgesia EFFICACY OF NSAIDS IN THE TREATMENT OF MUSCULOSKELETAL INJURIES Bone • Injury to bone causes an initial inflammatory response to begin fracture repair • Prostaglandins play a major role in bone formation and resorption and are critical in bone repair • Because fracture healing relies on inflammation and formation of PGs, and medication that blocks this process has the potential to impair fracture healing Bone • Several animal models suggest that NSAIDs negatively impact fracture healing • Studies in humans have associated NSAID uses with delayed healing in tibial fractures and increased risk for nonunion in various long bone fractures (Giannoudis et al) COX-2 in Fracture Healing COX-2 (not Cox-1) mediates the negative effect of NSAIDs Fracture healing is normal in COX-1 knockout mice Healing impaired in COX-2-selective, NSAID-treated Healing impaired in COX-2 knockout mice “Heterotopic ossification prophylaxis with indomethacin increases long-bone nonunion” Burd, et. al. in 2003– The best evidence to date in humans Looked at the concominant fx of surgicaly treated acetabular fractures that were prophylaxed with radiation or indomethacin 282 patients with 112 (40%) concomitant fx of femur, tibia, humerus, and/or forearm 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin No indomethacin – fractures with a non-union – 2.2% (no difference between radiation and no radiation patients) Indomethacin - fractures with a non-union – 15.3% Adverse effect mediated on chondrocyte differentiation Fracture healing mesenchymal cells differentiate into chondrocytes without COX-2. COX-2 required for chondrocytes to hypertrophy Hypertrophied chondrocytes secrete angiogenic and osteoclastogenic factors Endochondral vs. Primary Healing Primary Fracture Healing with internal fixation A form of intramembranous healing without a cartilage model akin to embryonic flat bone formation Unite by direct extenson of Haversian canals between fragments Forms lamellar bone later replaced by longitudinally oriented osteons Periosteal or endosteal mesenchymal cells not activated NSAIDs adverse effect on Primary Healing – indirect evidence in animals Effects of NSAIDs on primary bone healing less clear PGs produced by COX-1 or COX-2 promote osteoblast and osteoclast activity suggests NSAIDs can affect primary bone healing Bone ingrowth into porous metal implants impaired by NSAIDs in rabbits but not dogs Intramembranous bone formation inhibited in rabbits by treatment with COX-1 or COX-2 inhibitors COX-2 inhibition of intramembranous bone formation time dependent whereas even brief exposure to COX-2 disrupts endochondral bone formation Related Topic: Myositis Ossificans No RCT documenting efficacy of NSAIDs in the prevention or treatment of Myositis Ossificans (MO) Use for MO inferred from reduction of Heterotopic Ossification A 7-day course of indomethacin or other NSAID has been recommended for preventing MO after significant muscle contusions at risk Bone – Take Home Message • Difficult to draw definitive conclusions • Animal studies suggest that NSAIDs inhibit osteogenic activity • Majority of human studies support the negative effect of NSAIDs on fracture healing • Recommended that NSAIDs be avoided in the setting of bone injury Ligaments & Tendons Criteria for Successful Tendon & Ligament Healing 1) Mechanical strength must be reestablished 2) Tendons must glide freely through the tendon sheath 3) Ligament healing must prevent joint laxity Ligament • 3 Stages of healing 1. Initial inflammatory response to clear away damaged tissue 2. Proliferative phase during which new collagen is formed 3. Remodeling phase (may continue for up to 1 year) Ligament • Animal studies show conflicting results on ligament healing – studies on rat MCL sprains 1. Those treated with piroxicam were stronger than placebo at 14 days (Dahners, et al) 2. Separate study showed no difference with piroxicam from placebo at 21 days (Dahners, et al) 3. Celcoxib significantly weakened ligament healing at 14 days (Elder et al) – Other studies have shown no significant effect of ibuprofen, naproxen and rofecoxib on ligament strength as compared with placebo Tendon • The histopathology of tendinopathy is typically degenerative, with an absence of inflammatory cells or biochemical markers of inflammation In the lab - Tendon NSAIDs inhibit tenocyte proliferation & migration Increase protein synthesis in human tendon fibroblasts increasing collagen deposition Indomethacin or celecoxib increase strength of transected rat Achilles tendons, even though… cross-sectional area of the tendon was decreased NSAID treatment could minimize thickening of healed tendons, balanced by the positive effects of NSAIDs on collagen synthesis. Tendon Randomized study of Achilles tendinopathy found that piroxicam was no more effective than placebo (Astrom and Westlin) Tendon Glide Indomethacin (4 weeks) reduced adhesions post FDP tendon transection in rabbits Prevention of adhesion formation is a COX-1 mediated mechanism…. Occurs in the late healing stages COX-2 selective inhibitors lack this effect. Ankle Sprain • NSAIDs are effective at decreasing pain on weight bearing and swelling in short (<72h) and intermediate (<2wk) • No data to support faster return to activity • Piroxicam and diclofenac more effective than placebo for overall reduction of pain and inflammation after acute ankle sprains. (Moran) • Diclofenac and naproxin equivalent to celecoxib in pain relief and increasing functional ability after ankle sprains • Dyspepsia less with oral celecoxib than naproxin (Peter) Ankle Sprains – Piroxicam decreased pain and allowed army recruits with acute ankle sprains to return to training more rapidly than placebo (Slayter, et al). – Celecoxib was as effective as naproxen for pain reduction in treating acute ankle sprains (Petrella et al) • All of these studies are limited by lack of objective measure of ankle stability • On the basis of available evidence, a short course (3 to 7 days) of NSAIDs after a ligament sprain is likely beneficial Ligament Laxity Only one study of NSAIDs on joint laxity following ligament injury. Ketorolac for 6 wk after BPB autograft ACLreconstruction had significant increased in anterior-posterior laxity at 6 wk post-op compared to controls Suggests that NSAID therapy may increase joint laxity after a ligament injury or repair NSAIDs May Inhibit Enthesis Repair Celecoxib & Indomethacin caused inconsistent regrowth of the fibrocartilage zone in acute supraspinatus repair compared to control in rats Celecoxib & Indomethacin reduced failure loads for rotator cuff repairs in rats Cartilage/Joint Intra-articular ketorolac – 2004 Dogan Can induce minimal to moderate articular cartilage inflammation in rabbit knee joints Can induce synovial membrane inflammatory cell infiltration Can induce synovial membrane cell hyperplasia Can induce synovial membrane cell hypertrophy Authors recommended caution when injecting ketorolac into the joint space Cartilage/Joint Intra-articular tibiofemoral injection of ketorolac has no detrimental effects on joint mechanics in a rat model – 2014 64 rats injected withsaline or ketorolac Animals euthanized at 2, 7, 28, and 84 days postinjection for histological & mechanical analyses No differences at any time point NSAID injection could be considered for clinical application in humans Intra-articular ketorolac reduces pain following ACL surgery Ketorolac + morphine & ropivacaine better postop analgesia than morphine + ropivacaine without ketorolac – 2005 And after Arthroscopic Shoulder Surgery Ketorolac + fentanyl + ropivacaine better postop analgesia than ropivacaine alone or fentanyl + ropivacaine – 2009 Bursa NSAID Intrabursal Injection Superior to Cortisone for Shoulder Pain – 2013 DBRCT 32 patients external shoulder impingement 40 mg triamcinolone vs. 60 mg ketorolac (both w lido) UCLA Shoulder Asses Score – 2.13 vs. 7.15 at 1 mo Ketorolac inc forward flexion strength (0.26 vs −0.07; P = .04) Improved patient satisfaction over the steroid group; P = .03. Muscle • Muscle injury can be caused by strain, contusion, or laceration. • Heals similar to ligaments: 1. Destruction (inflammatory cell reaction) 2. Repair 3. Remodeling Muscle • Initial inflammatory response initiates macrophage action – Subsequent phagocytosis of necrotic tissue and stimulation of new capillary formation • Inflammation also causes edema with resultant anoxia and further cell death • Modulation of the inflammatory response with low-dose NSAID in the subacute phase, may have beneficial effects in limiting edema Muscle • NSAIDs can decrease eccentrically induced muscle soreness (Altman, et al) • NSAID patches can be beneficial in early management of contusion type injuries (Predel, et al) Exercise Induced Muscle Damage NSAIDS hurt muscle development if you’re a mouse; No problem if your human Rodent studies show NSAIDS reduce muscle growth after chronic overload NSAIDS have a negative effect on satellite cell activity in rodents and humans (satellite cells are myogenic stem cells that respond to prostaglandin by proliferating and fusing to existing muscle cells and donating their nuclei) NSAIDS do not reduce human muscle hypertrophy in short term use and may increase it in the untrained Gout Moderate quality evidence - NSAIDS and systemic glucocorticoids (GC) effective as NSAID but GCs are safer. – review 2014 Low quality evidence (1 trial) showed no difference between NSAID and placebo with regard to pain or inflammation No NSAID was superior to another Low quality evidence (1 trial) showed that both high- and low-dose colchicine more effective than placebo & low-dose colchicine is safe as placebo & safer than high dose colchicine Adverse Effects • More frequent when used on a chronic basis than on an acute intermittent administration • GI Toxicity – Contribute to an estimated 100,000 hospital admissions and 16,500 deaths each year from GI complications • Reduce risk with short dosing periods, take medication with food, use of PPI or misoprostol • Use Selective COX-2 inhibitor (Celebrex) NSAID Adverse Effects • May have adverse cardiovascular, neurovascular and renal effects – most concern involves long-term use – Increasing incidence of hypertension with greater NSAID use • Coxibs and non-selective NSAIDs associated with increased likelihood of cardiovascular events; naproxen has lowest risk – Minimal side effects with short-term use in a typical sports medicine population NSAID Renal Effects in Elderly NSAID use in Elderly with Co-morbidity Congestive heart failure Liver cirrhosis Chronic kidney disease May develop acute renal failure NSAIDs Possible Renal Effects Interstitial nephritis Nephrotic syndrome Acute renal failure Acute tubular necrosis Severe renal impairment with Combination with ACE inhibitor (AI) & diuretic NSAID inhibits prostaglandin production removing its vasodilitation effect on the afferent arteriole AI removes angiotensin II's vasoconstriction of efferent arteriole Diuretic drops plasma volume, and thereby RPF The so-called “Triple Whammy Effect” NSAID Renal Effects on Potassium in compromised Kidneys NSAIDS decrease nephron’s distal sodium delivery by reducing glomerular filtration. Less sodium available for potassium exchange NSAIDS inhibit macula densa PGs production they reduce renin release. Less renin results in decreased potassium excretion. Effects on Sodium later in talk Reducing Risks of Adverse Effects Prescribe at the lowest possible dose for short courses Long term use only for those who cannot tolerate other forms of analgesia and use regularly reviewed Selective COX-2 inhibitors (coxibs) offer greater UGI safety Concurrent low-dose ASA Tx increases GI side effect risk – avoid unless absolutely necessary Coxibs and non-selective NSAIDS increase cardiac risk; naproxen appears to have the lowest risk Reducing Risks of Adverse Effects Co-Rx of a PPI with the “Safest Possible” non-selective NSAID or coxib is effective in reducing GI toxicity with long-term use. But, PPI may increase risk of C. diff, and Fx’s or hip, wrist and spine Limited evidence supports H2 blocker at double dose “Safest Possible” Risk – ibuprofen (lowest) < indomethacin, diclofenac, naproxin (intermed) < piroxecam, ketoprofen, ketorolac (higher) < azopropazone (highest – UK only, now DC’d) Misoprostol is alternative but use may be limited by side effects (abdominal pain, nausea, flatulence, headache, dyspepsia, vomiting, and constipation) Arthrotec is diclofenac/misoprostol Testing and eradicating H. pylori in first time NSAID patients with hx of dyspepsia or ulceration (no benefit if already taking an NSAID) Prophylactic Misuse of NSAIDs • Athletes have relatively unrestricted access to NSAIDs – 25% of athletes at Sydney 2000 Olympic Games reported using NSAIDs 3 days prior to random drug testing - 10% of Soccer players at the 2006 World Cup tournament took NSAIDs before every match - Players take NSAIDS daily because of perceived benefits in terms of blocking pain before it occurs Prophylactic Misuse of NSAIDs • Adverse GI and cardiovascular effects become more pronounced with increased duration of use. • NSAIDs taken before activity may mask pain and cause athletes to allow pathology to progress • NSAIDs’ inhibitory effects on the COX isozymes and prostaglandins may impede the synthesis of the extracellular matrix (ie collagen) that confers strength to the tissue Prophylactic Misuse of NSAIDs- Danger for the Marathoner Intrarenal PGs inhibit vasopressindependent transtubularwater movement. NSAIDS remove the inhibitory effect of PGs on antidiuretic hormone (ADH) activity. NSAIDS also block the PGs increase of medullary blood flow increasing medullary interstitial osmotic drive. Free water excretion reduced producing hyponatremia. Summary/Recommendations • NSAID use in sports injuries continues to be controversial • Effects are mediated through inhibition of prostaglandin synthesis in the COX pathway of inflammation • NSAIDs may adversely affect healing in some sports-related injuries • Conclusive support for NSAID use is limited due to numerous animal studies, but few randomized clinical trials in humans • Use simple analgesia when analgesia is the desired outcome • Minimize risks of adverse effects in long term use Summary/Recommendations • No clinical evidence to suggest that regular use of NSAIDs reduces injury risk or improves function in the typical athlete • Avoid NSAIDs in the treatment of completed fractures, stress fractures or in the setting of chronic muscle injuries • NSAID use should always be coupled with appropriate physical rehabilitation • Judicious short-term uses of NSAIDS, with consideration of the specific type of injury, level of dysfunction, and pain, may be useful in the management of acute ligament sprains, muscle strains, tendinitis, and eccentric muscle injury References • • • • • • • • • • • Mehallo,DO, Christopher J., Jonathan A. Drezner,MD, and Jeffrey R. Bytomski. "Practical Management: Nonsteroidal Antiinflammatory Drug (NSAID) Use in Athletic Injuries." Clinical Journal of Sports Medicine 16.2 (2006): 170-74 Print Paoloni, J. A., C. Milne, and J. Orchard. "Non-steroidal anti-inflammatory drugs in sports medicine: guidelines for practical but sensible use." British Journal of Sports Medicine 43 (2009): 863-65 Print Scott, A., K. M. Khan, and C. R. Roberts. "What do we mean by the term "inflammation"? A contemporary basic science update for sports medicine." British Journal of Sports Medicine 38 (2004): 372-380. Print Solomon,MD, Daniel H. "NSAIDs: Mechanism of action." UpToDate. Ed. Daniel E. Furst,MD and Paul L. Romain,MD. 7 Dec. 2006. Web. 16 Nov. 2009. <http://utdol.com/online/content/topic.do?topicKey+tx_rheum/6887> Warden, Stuart J. "Prophylactic misuse and recommended use of non-steroidal anti-inflammatory drugs by athletes." British Journal of Sports Medicine 43 (2009): 548-49 Print Silberman MD, Marc. "Non-steroidal anti-inflammatory drugs in sports: Take them or leave them?" Web. 01 Feb. 2010. http://njsportsmed.com/Hot_Topics_NSAID.html Bailey, Su and O’Connor, JP. “NSAID therapy effects on healing of bone, tendon and the enthesis.” Journal of Applied Physiology (1985). 2013 Sept 15; 115(6): 892-899 Print “Reducing NSAID-induced gastrointestinal complications” Drug and Therapeutics Bullitin 2011 Feb;49(2):18-21 Print T. A. Burd, M. S. Hughes, J. O. Anglen. “Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion” J Bone Joint Surg [Br] 2003;85-B:700-5 Walter H. Hörl. “Nonsteroidal Anti-Inflammatory Drugs and the Kidney” Pharmaceuticals 2010, 3, 22912321 Print Schoenfeld, Brad J. “The Use of Nonsteroidal Anti-Inflammatory Drugs for Exercise-Induced Muscle Damage” Sports Medicine 2012: 42(12): 1017-1028 References • • • • • • American Orthopaedic Society for Sports Medicine (AOSSM) 2011 Annual Meeting: Abstract 34. Presented July 10, 2011. “A double-blind randomized controlled trial comparing the effects of subacromial injection with corticosteroid versus NSAID in patients with shoulder impingement syndrome. J Shoulder Elbow Surg. 2013 May;22(5):595-601 Kim IS, Shin KM, Kang SS, Jang JS, Hong SJ, Yoon YJ, Lee HJ. “A comparative study on the analgesic effect of continuous intraarticular infusion with ropivacaine, ropivacaine/fentanyl and ropivacaine/fentanyl/ketorolac after arthroscopic shoulder surgery” Korean J Anesthesiol. 2009 Mar;56(3):303-308 Vintar N, Rawal N, Veselko M. “Intraarticular patient-controlled regional anesthesia after arthroscopically assisted anterior cruciate ligament reconstruction: ropivacaine/morphine/ketorolac versus ropivacaine/morphine.” Anesthesia & Analgesia Journal 2005 Aug;101(2):573-8 Riggin CN1, Tucker JJ, Soslowsky LJ, Kuntz AF. “Intra-articular tibiofemoral injection of a nonsteroidal anti-inflammatory drug has no detrimental effects on joint mechanics in a rat model.” Journal of Orthopaedic Research 2014 Nov;32(11):1512-9. Dogan N, Erdem, AF, Gundogdu C, Kursad H, Kizilkaya M. “The effects of ketorolac on articular cartilage and synovium in the rabbit knee joint.” Canadian Journal of Physiology and Pharmacology 2004 Jul;82(7)502-5 Wechalekar MD, et al. “The efficacy and safety of treatments for acute gout: results from a series of systematic literature reviews including Cochrane reviews on intraarticular glucocorticoids, colchicine, nonsteroidal antiinflammatory drugs, and interleukin-1 inhibitors. “ Journal of Rheumatology Supplement 2014 Sep;92:15-25