Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
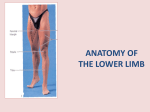
Visualização do documento Lower extremity-I.doc (97 KB) Baixar 22  TOPOGRAPHIC ANATOMY OF THE LOWER LIMB - I The lower limb includes: the gluteal region, the thigh reÂgion, the knee region, the leg region, the ankle region, the foÂot region and joints. THE GLUTEAL REGION The gluteal region, or buttock, is bounded: superiorly – by the iliac crest, inferiorly – by the fold of buttock, medially – by median sacral crest, laterally – by the line connecting the superior anterior iliac spine and greater trochanter. The osteoligamentous tela of this region is composed by hip bone, sacrotuberous ligament, sacrospinous ligament, capsule of hip joint, neck of femur, greater trochanter. The sacrotuberous ligament and sacrospinous ligament convert the greater and lesÂser sciatic notches into foramina, the greater and lesser sciaÂtic foramina. The two ligaments also prevent the lower end of the sacrum and the coccyx from being rotated upward at the sacÂroiliac joint by the weight of the body. Surface landmarks. The iliac crest are easily palpable along their entries length. Each crest ends in front at the anÂterior superior iliac spine and behind at the posterior superior iliac spine. The posterior superior iliac spine lies beneath a skin dimple at the level of the second vertebra and the middle of the sacroiliac joint. The ischial tuberosity can be palpated in the lower part of the buttock. In standing position the tubeÂrosity is covered by the gluteus maximus. In the sitting positiÂon the ischial tuberosity emerges from beneath the lower border of the gluteus maximus and supports the weight of the body; in this position, the tuberosity is separated from the skin by only a bursa and a pad of fat. The greater trochanter of the femur can be felt on the laÂteral surface of the thigh and moves beneath the examining finÂger as the hip joint is flexed and extended. It is important to verify that, in the normal hip joint, the upper border of the greater trochanter lies on a line connecting the anterior superior iliac spine to the ischial tuberosity (line of Rozer- NelaÂton). The spinous processes of the sacrum are fused with each other to form the median sacral crest. The crest can be felt beÂneath the skin in the upper part of the cleft between the butÂtock. The tip of the coccyx can be palpated beneath the skin in the cleft between the buttock about 2,5 cm behind the anus. The anterior surface of the coccyx may be palpated with a gloved finger in the anal canal. The fold of the buttocks is most prominent in the standing position: its lower border does not correspond to the lower borÂder of the gluteus maximus muscle. Layers. The skin is thick and dense and contains many sebaÂceous glands. The skin of the upper part of the buttock is suppÂlied by the subcostal and iliohypogastric nerves and by cutaneous branches of lumbar dorsal rami (nerves of clunes superior, middle, inferior). Below it is supplied by branches of the posterior cutaneous nerve of the thigh. Beneath the skin there lies subcutaneous tissue. This layer is thick, especially in women, and is impregnated for the promiÂnence of the buttock. The subcutaneous tissue has lobate strucÂture as the fibrous septa divide it into many lobules. The fibÂrous septa connect the skin with the underlying gluteal fascia or deep fascia. By this we can complain that pyo-inflammatory process of subcutaneous fat has local character. The deep fascia is continuous below with the deep fascia, or fascia lata of the thigh. In the gluteal region it splits to enclose the gluteus maximus muscle, gives partial origin to it, and sends septa into it to divided it into coarse bundles. The pyoinflammatory process within the gluteal maximus muscle has local character and causes strong pain (violent pain, throc). Above the gluteus maximus the deep fascia continues as a single layer that covers the outer surface of the gluteus medius and is attached to the iliac crest. On the lateral surface of the thigh, the fascia is thickened to form a strong, wide bent, the iliotibial tract. This is attached above to the tubercle of the iliac crest and below to the lateral condyle of the tibia. The iliotoboal tract form a sheath for the tensor fasciae latae muscle and receives the greater part of the insertion of the gluteus maximus. The buttock is commonly used as a site for intramuscular injections and to eliminate any risk of damaging the sciatic nerÂve, the upper outer quadrant should be used for this purpose. Under deep fascia the muscles are located within the gluteÂal region. These are three layers of muscles. First layer of muscles consists of gluteus maximus muscle and upper part of gluteus medius muscle. The gluteus maximus is a large muscle that arises from the outer surface of the ilium, from the adjacent posterior surface of the sacrum and coccyx, and from the sacrotuberous ligament. The fibers pass downward and laterally and the majority are inÂserted into the iliotibial tract; some of the deeper fibers are inserted into the gluteal tuberosity of the femur. As the muscle crosses the greater trochanter it is separated from this by a large bursa. The gluteus maximus is a powerful extensor of the thigh on the trunk, a uniquely human action. It little used in walking, but brought into play in running and climbing, or, when the limb is fixed raising the trunk as from a aretonial bow. Gluteus maÂximus is supplied by the inferior gluteal nerve. Beneath the sheath of the gluteus maximus muscle the next layer of the muscles is located. The succession of the muscles of second layer from above downward is: the lower part of gluteus medius, piriformis, obturator internus with the gemelli muscles and quadratus femoris. The gluteus medius arises from the ilium. It is largely overlapped by the gluteus maximus posteriorly. Its fibers converge on a tendon which is attached to the lateral aspect of the greater trochanter of the femur. Here a bursa separates the tenÂdon from the upper part of the trochanter. It is supplied by the superior gluteal nerve. Acting with the gluteus minimus and the tensor fasciae latae, the thigh is powerfully abducted at the hip joint. Its most important action takes place in walking or running; the three muscles contract and steady the pelvis on the lower limb. When the foot of the opposite side is taken off the ground and thrust forward, the pelvis is held in position and does not tilt downward on the unsupported side. The anterior fibers also medially rotate the thigh; posterior fibers rotate laterally. The piriformis arises from the middle three pieces of the sacrum and leaves the pelvis through the greater sciatic notch still as a fleshy belly. It is inserted by a tendon into the upÂper border of the greater trochanter. It acts as a lateral rotaÂtor of the thigh and is supplied in the pelvis by branches of the first and second sacral nerves. The obturator internus arises from the inner aspect of the pelvic bone and here has important relations to the pelvis caviÂty and perineum. Its fleshy belly is replaced by a tendon as it passed over the lesser sciatic notch. Here the tendon makes a rightanglen turn to reach the medial surface of the greater trochanter above the trochanteric fossa. Where this sudden chanÂge in direction is made the tendon is separated from the bone by a bursa and a layer of hyaline cartilage. Obturator internus is supplied by the nerve to obturator internus which reaches the perineal surface of the muscle through the lesser sciatic foraÂmen. The gemelli muscles are two small bellies which arise from the ischium above and below the lesser sciatic notch and accomÂpany, and often hide, the extrapelvic course of the tendon of obturator internus with which they gain insertion. The action of obturator internus and the gemelly is to rotate the thigh lateÂrally. The superior gemellus is supplied by the nerve to obturaÂtor internus and the inferior by the nerve to quadratus femoris. Quadratus femoris arises from the ischium just anterior to the ischial tuberosity and extends to the intertrochanteric crest and quadrate tubercle of the femur. It adducts thigh and rotates it laterally. It is supplied by the nerve to quadratus femoris. The fat space is located between gluteus maximus muscle and second layers of muscles. The loose aredar tissue occupies this fat space. Beneath the second layer of muscles the third layer of muscles is located. This layer consists of two muscle: superiorÂly – gluteus minimus, inferiorly – obturator externus. The gluteus minimus arises from the ilium and lies deep to gluteus medius. It tendon also finds attachment to the lateral aspect of the greater trochanter of the femur and again a bursa lies between the tendon and the underlying trochanter. It is supplied by the superior gluteal nerve. Acting with the gluteus medius and the tensor fasciae latae, the thigh is powerfully abÂducted at the hip joint. The anterior fibers also medially rotaÂte the thigh. Obturator externus arises from the front of the pelvis, and winds backward below the hip-joint to enter the gluteal region, where it passes upwards and in a lateral direction over the back of the neck of the femur under cover of quadratus femoris and tapers to be inserted by tendon into the floor of the trochanteÂric fossa. It is a lateral rotator of the thigh. Foramina of the gluteal region. There are two important foramina in the gluteal region: the greater sciatic foramen and the lesser sciatic foramen. Greater sciatic foramen is formed by the conversion of the greater sciatic notch of the hip bone into a foramen by the preÂsence of the sacrotuberous and sacrospinous ligaments. It proviÂdes an exit from the pelvis into the gluteal region. The folloÂwing structures pass through the foramen: piriformis, sciatic nerve, posterior cutaneous nerve of the thigh, superior and inÂferior gluteal nerves, pudendal nerve, superior and inferior gluteal arteries and veins, internal pudendal artery and vein. Lesser sciatic foramen is formed by the conversion of the lesser sciatic notch of the hip bone into a foramen by the preÂsence of the sacrotuberous and sacrospinous ligaments. It proviÂded an entrance into the perineum from the gluteal region. Its presence enables nerves and blood vessels, that have left the pelvis through the greater sciatic foramen above the pelvic floÂor to enter the perineum below the pelvic floor. The following structures pass through the foramen: tendon of obturator interÂnus muscle, pudendal nerve, internal pudendal artery and vein. The piriformis muscle passing through greater sciatic foraÂmen divides it and forms two small foramina: above – suprapiriÂformis , below – infrapiriformis. The suprapiriformis foramen is limited superiorly – by infeÂrior border of gluteus medius muscle and inferiorly – by superior border of the piriformis muscle. It transmits the superior glu... Arquivo da conta: gblnetto Outros arquivos desta pasta: Amputations and exarticulations.doc (621 KB) Perineum.doc (139 KB) Operations on the large intestine.doc (2323 KB) Pelvis.doc (104 KB) Thoracic cavity.doc (90 KB) Outros arquivos desta conta: Lecture Mad Alla majors OS BASE ANSWERS (all majors) Relatar se os regulamentos foram violados Página inicial Contacta-nos Ajuda Opções Termos e condições PolÃtica de privacidade Reportar abuso Copyright © 2012 Minhateca.com.br