Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Behçet's disease wikipedia , lookup
Chagas disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Typhoid fever wikipedia , lookup
Globalization and disease wikipedia , lookup
Kawasaki disease wikipedia , lookup
Germ theory of disease wikipedia , lookup
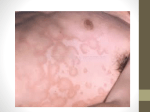
Fifth stage خليل.د Pediatric Lec-4 23/11/2016 Acquired Heart Diseases Acute rheumatic fever; cardiomyopathies; cardiovascular infections, including myocarditis and infective endocarditis; and non congenital valvular heart disease are the most common acquired heart diseases among the pediatric age group patients. Rheumatic Fever Definition Rheumatic fever is a delayed autoimmune reaction in genetically predisposed individuals to group A, β-hemolytic, streptococcal pharyngitis. It is a self-limited disease that may involve joints, skin, brain, serous surfaces, and the heart Despite the dramatic nature of the acute episode, ARF leaves no lasting damage to the brain, joints or skin. Epidemiology The incidence of acute rheumatic fever is 3 to 61 per 100,000 school children. ARF is predominantly a disease of children aged 5-14 years and generally does not affect children less than 3 years old or adults. Acute rheumatic fever is most common during winter and spring, a seasonal variation similar to that of streptococcal pharyngitis. Clinical manifestation • Acute rheumatic fever is diagnosed using the revised Jones criteria, which consist of clinical and laboratory findings. • The presence of either two major criteria or one major and two minor criteria, along with evidence of an antecedent streptococcal infection, confirm a diagnosis of acute rheumatic fever. • The infection often precedes the presentation of rheumatic fever by 2 to 6 weeks. 1 Supporting evidence of a preceding streptococcal infection 1. 2. 3. 4. Elevated or rising antistreptolysin-O or other streptococcal antibody, or Rapid antigen test for group A streptococci, or A positive throat culture, or Recent scarlet fever. Laboratory Findings 1. High ESR. 2. Anemia, leucocytosis . 3. Elevated C-reactive protein. 4. ASO titre >200 Todd units 5. Anti-DNAse B test . 6. Throat culture-GABH streptococci. 2 7. ECGprolonged PR interval, 2nd or 3rd degree blocks , ST depression or T inversion. 8. 2 D Echo cardiography – valve edema ,mitral regurgitation, LA & LV dilatation ,pericardial effusion ,decreased contractility. Management 1. Benzathine penicillin G, 0.6 to 1.2 million units intramuscularly, is given to eradicate streptococci. This serves as the first dose of penicillin prophylaxis as well . In patients allergic to penicillin, erythromycin, 40 mg/kg per day in two to four doses for 10 days, may be substituted for penicillin. 2. Bed rest of varying duration is recommended. The duration depends on the type and severity of the manifestations and may range from a week (for isolated arthritis) to several weeks for severe carditis. Bed rest is followed by a period of indoor ambulation of varying duration before the child is allowed to return to school. 3. Therapy with anti-inflammatory agents should be started as soon as acute rheumatic fever has been diagnosed as follows. Prednisone, 2 mg/kg/24 hours in 4 divided doses. Aspirin, 100 mg/kg/d in4-6 divided doses. 3 4. Treatment of CHF includes the following: a. Complete bed rest with O2. b. Prednisone for severe carditis of recent onset c. Digoxin, used with caution, beginning with half the usual recommended dose, because certain patients with rheumatic carditis are supersensitive to digitalis. d. Furosemide,1 mg/kg every 6 to 12 hour. 5. Management of Sydenham's chorea: a. Reduce physical and emotional stress. b. For severe cases, any of the following drugs may be used: phenobarbital , haloperidol ,valproic acid, chlorpromazine (Thorazine), diazepam (Valium), or steroids. Prevention (prophylaxis) A patient who has had acute rheumatic fever is susceptible to recurrent rheumatic fever for the rest of his life. Recommended Duration of Prophylaxis for Rheumatic Fever Category Rheumatic fever without carditis Rheumatic fever with carditis but without residual heart disease (no valvular disease) Duration At least for 5 yr or until age 21 yr, whichever is longer At least for 10 yr or well into adulthood, whichever is longer Rheumatic fever with carditis and residual heart disease (persistent valvular disease) At least 10 yr since last episode and at least until age 40 yr; sometimes lifelong prophylaxis 4 Cardiomyopathies Primary myocardial disease, or cardiomyopathy, is a disease of the heart muscle itself, not associated with congenital, valvular, or coronary heart disease or systemic disorders. Cardiomyopathy has been classified into three types based on anatomic and functional features: hypertrophic, dilated (or congestive), and restrictive Features of different types Feature Hypertrophic Dilated Restrictive Etiology Inherited (AD in about 50%) Sporadic (new mutation ±) Pluricausal (e.g., toxic, metabolic, infectious, alcohol, doxorubicin) Myocardial fibrosis, hypertrophy, or infiltration (amyloid, hemochromatosis) Hemodynamic dysfunction Diastolic dysfunction (rigid ventricular walls impede ventricular filling) Systolic contractile dysfunction (↓ cardiac output, ↓ stroke volume, ↑ LVEDP) Diastolic dysfunction (with normal systolic function) (abnormally stiff LV with impaired ventricular filling) Symptoms Infants, frequently present with signs of CHF . Older children may be asymptomatic, with sudden death as the initial presentation. Dyspnea, fatigue, chest pain, syncope or nearsyncope, and palpitations may be present. signs and symptoms Exercise intolerance, of inadequate cardiac weakness and dyspnea, output and CHF. or chest pain. 5 Feature On examination Hypertrophic Dilated Restrictive A murmur is heard in Features of CHF. Rales more than 50% of may be audible on children. pulmonary auscultation. Heart sounds may be muffled, and S3 is often present. Concurrent infectious illness may result in circulatory collapse and shock in children with dilated cardiomyopathies Thickened LV (and Biventricular dilatation occasionally RV) wall and ↓ EF% Jugular venous distention, gallop rhythm, and a systolic murmur of AV valve regurgitation may be present. Electrocardiography (LVH), ST-T changes, and abnormally deep Q waves (owing to septal hypertrophy) Sinus tachycardia, LVH, and ST-T changes are the most common findings. Atrial hypertrophy. It may show atrial fibrillation and paroxysms of supraventricular tachycardia. Chest x ray Mild left ventricular enlargement with a globular-shaped heart. Generalized cardiomegaly is usually present, with or without signs of pulmonary venous hypertension or pulmonary edema. cardiomegaly, pulmonary venous congestion, and occasional pleural effusion. Treatment -β-Adrenoreceptor blockers -Vasodilator therapy -Diuretics -Digitalis plus diuretics -Anticoagulants (±) -β-Adrenoceptor blockers (±) Antiarrhythmics (±) Cardiac transplantation (±) -Corticosteroids (±) Echocardiography -Calcium antagonists -(Digitalis/catechols ,Diuretics and nitrates are contraindicated). Biatrial enlargement -Permanent pacemaker for advanced heart block (±) -Cardiac transplantation (±) 6