Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
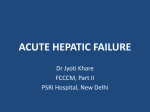
Gastroenterology Board Review Manual Statement of Editorial Purpose The Hospital Physician Gastroenterology Board Review Manual is a study guide for fellows and practicing physicians preparing for board examinations in gastroenterology. Each manual reviews a topic essential to current practice in the subspecialty of gastroenterology. PUBLISHING STAFF PRESIDENT, Group PUBLISHER Acute Liver Failure Contributors: Nicholas Agresti, MD Gastroenterology Fellow, Division of Gastroenterology and Hepatology, University of Florida, Jacksonville, FL Christopher O’Brien, MD, AGAF, FRCMI Chief of Clinical Hepatology and Research, Center for Liver Diseases, Professor of Clinical Medicine, Divisions of Liver and GI Transplantation, University of Miami School of Medicine, Miami, FL Bruce M. White Senior EDITOR Robert Litchkofski executive vice president Barbara T. White executive director of operations Jean M. Gaul Table of Contents NOTE FROM THE PUBLISHER: This publication has been developed with out involvement of or review by the Amer ican Board of Internal Medicine. Hospital Physician Board Review Manual Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Initital Evaluation. . . . . . . . . . . . . . . . . . . . . . . . . 1 Etiology and Management . . . . . . . . . . . . . . . . . . 2 Treatment of Acute Liver Failure. . . . . . . . . . . . 10 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Board Review Questions. . . . . . . . . . . . . . . . . . . 12 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 www.turner-white.com Acute Liver Failure Gastroenterology Board Review Manual Acute Liver Failure Nicholas Agresti, MD, and Christopher O’Brien, MD, AGAF, FRCMI Introduction Acute liver failure (ALF) is the rapid onset of severe liver injury, hepatic encephalopathy, and coagulopathy (international normalized ratio [INR] >1.5) in a patient without preexisting liver disease.1 The incidence of ALF in the United States is approximately 3000 cases per year, with the majority of ALF cases caused by drug-induced liver injury (DILI) followed by viral hepatitis.1–3 Identifying the etiology and managing the sequelae of liver failure, such as cerebral edema, encephalopathy, coagulopathy, hemodynamic instability, renal failure, metabolic disturbances, and infection, are the mainstays of treatment.4 Prior to the advent of liver transplantation, ALF was almost universally fatal, with a 15% survival rate. However, with liver transplantation the 1-year survival rate now ranges from 65% to 73%, and is higher yet with a living related donor transplant.5–7 The early management of patients should occur in the intensive care unit (ICU) with transfer to a liver transplant center as soon as possible. INITIAL EVALUATION A patient with ALF will typically present with laboratory data consistent with acute hepatitis, a prolonged prothrombin time of 6 seconds or more, an INR ≥1.5, and a change in mental status. A focused history and physical examination with attention to ingestion of toxins is important so that specific therapy can be initiated, as the natural history of ALF is impacted by its cause (Table 1).4,8 An accurate history is critical, since certain etiologies of ALF (ie, autoimmune hepatitis, hepatitis B, DILI, and those of indeterminate cause) have a dismal survival rate (<25%) without liver transplant. The initial laboratory studies are directed to determining the etiology and severity of the liver disease (Table 2). Blood studies should include a complete blood count, complete metabolic profile, arterial blood gas analysis, coagulation profile, blood type and screen, and diagnostic tests to rule out specific etiologies of ALF.4 The initial physical exam should include a mental status exam with documentation of grade of encephalopathy (Table 3) and a search for findings consistent with preexisting, chronic liver disease, such as bitemporal wasting, parotid gland enlargement, spider angiomata, gynecomastia, splenomegaly, and testicular atrophy. Although ascites is typically seen in chronic liver disease, it can present in ALF with etiologies such as veno-occlusive disease. Copyright 2013, Turner White Communications, Inc., Strafford Avenue, Suite 220, Wayne, PA 19087-3391, www.turner-white.com. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White Communications. The preparation and distribution of this publication are supported by sponsorship subject to written agreements that stipulate and ensure the editorial independence of Turner White Communications. Turner White Communications retains full control over the design and production of all published materials, including selection of topics and preparation of editorial content. The authors are solely responsible for substantive content. Statements expressed reflect the views of the authors and not necessarily the opinions or policies of Turner White Communications. Turner White Communications accepts no responsibility for statements made by authors and will not be liable for any errors of omission or inaccuracies. Information contained within this publication should not be used as a substitute for clinical judgment. www.turner-white.comGastroenterology Volume 14, Part 6 1 Acute Liver Failure Table 1. Etiology and Management Options in Acute Liver Failure Table 2. Initial Laboratory Studies Etiology Treatment Prothrombin time/INR Acetaminophen N-acetylcysteine Herpes simplex virus Cytomegalovirus Pregnancy associated Budd-Chiari syndrome Acyclovir Ganciclovir Delivery Thrombolysis, vascular shunt, treat underlying cause, hepatic venous angioplasty, stenting of inferior vena cava Decompressive vascular shunt, thrombolysis Inotropes Antibiotics, vasopressor support Liver transplantation Penicillin, silibinin Chemotherapy Veno-occlusive disease Cardiac failure Septic shock Wilson disease Amanita phalloides Lymphoma ETIOLOGY AND MANAGEMENT Complete metabolic profile Blood type and screen Complete blood count Toxicology screen Viral hepatitis serologies: anti-HAV IgM, HBsAg/HBcAb IgM, anti-HCV/HCV RNA PCR, anti-HEV, HSV1 IgM, VZV Ceruloplasmin level Pregnancy test Ammonia level Autoimmune markers: ANA, ASMA, immunoglobulin levels HIV-1, HIV-2 assays Amylase, lipase Arterial blood gas, arterial lactate Acetaminophen level Urine electrolytes ANA = antinuclear antibody; ASMA = anti-smooth muscle antibody; HAV = hepatitis A virus; HBsAg/HBcAb = hepatitis B surface antigen/ hepatitis B core antigen; HCV = hepatitis C virus; HEV = hepatitis E virus; HSV1 = herpes simplex virus 1; IgM = immunoglobulin M; PCR = polymerase chain reaction; VZV = varicella zoster virus. ACETAMINOPHEN Toxicity Accounting for approximately 40% of ALF cases, ingestion of more than 10 g of acetaminophen may cause severe liver injury and carries a high mortality rate.4,9–12 The standard acetaminophen toxicity nomogram may be useful to determine the likelihood of serious liver injury in a patient upon initial presentation. A low or absent level of acetaminophen does not rule out hepatotoxicity since the time of ingestion could be unknown or the ingestion could have occurred in multiple dosage intervals.13,14 The clinical features of acetaminophen hepatotoxicity are variable but usually occur over 12 to 72 hours and in 3 phases. The first phase (12 to 24 hours post ingestion) is characterized by nausea, vomiting, and anorexia. This is followed by a second phase, usually lasting 24 hours, of relative well-being, which can rapidly deteriorate to the third phase. The third phase, occurring 24 to 48 2 Hospital Physician Board Review Manual hours after ingestion, includes the onset of multisystem organ failure usually requiring admission to the ICU.4 Grading Severity and Transplant Referral The King's College Criteria provide objective criteria to predict the risk of death after an acetaminophen overdose or other causes of ALF (Table 4). In acetaminophen hepatotoxicity, there are 2 important criteria for risk of death: an arterial pH of less than 7.3, irrespective of grade of encephalopathy; or a prothrombin time greater than 100 seconds and a serum creatinine concentration greater than 3.4 mg/dL (301 mmol/L) in patients who have grade III or IV encephalopathy. In other causes of ALF, liver transplantation is indicated in patients who have either a prothrombin www.turner-white.com Acute Liver Failure time greater than 100 seconds, irrespective of the grade of encephalopathy, or any 3 of the following variables: age less than 10 or greater than 40 years, hepatitis of unknown origin, idiosyncratic drug reactions, duration of jaundice before development of encephalopathy greater than 7 days, prothrombin time greater than 50 seconds, or serum bilirubin greater than 18 mg/dL. Table 3. Encephalopathy Grades Grade of Encephalopathy Description I Minimal change in consciousness, altered mood Inappropriate behavior, drowsy, asterixis Disoriented, difficult to arouse, slurred or incoherent speech Comatose, posturing, no response to painful stimuli II III IV Acetaminophen Metabolic Pathways The biochemical pathways of acetaminophen metabolism and histological changes on liver biopsy in ALF are well known. The biochemical pathway is provided in the Figure. Acetaminophen is predominantly conjugated into glucuronate and sulfate moieties by phase II metabolism and excreted in the urine. Approximately 5% is metabolized by the cytochrome P450 pathway to the toxic metabolite NAPQI, which is conjugated by glutathione to nontoxic cysteine and mercapturic acid moieties. In acetaminophen toxicity, the phase II conjugation enzymes become saturated and a higher fraction of acetaminophen is converted to NAPQI. The conjugation of NAPQI to glucuronide occurs until the hepatic reserves of glutathione are depleted, after which NAPQI accumulates and causes damage to the hepatocytes. The NAPQI binds to cellular proteins, inducing oxidation in thiol groups in mitochondria leading to formation of other toxic metabolites and overall mitochondria dysfunction. Damage occurs primarily in areas of the liver that are furthest away from the hepatic artery and thus relatively poorly perfused with oxygen, termed zone 3 of the hepatic lobule. Acetaminophen overdose is associated with zone 3 submassive (bridging) or panacinar (massive) necrosis.11 Treatment The basis of treatment for acetaminopheninduced liver failure focuses on early detection and proper administration of N-acetylcysteine (NAC). In ALF, the aminotransferase levels classically are in the 1000s, with the aspartate aminotransferase (AST) greater than the alanine aminotransferase (ALT) level; these findings are helpful in differentiating acetaminophen toxicity from other causes of ALF. Despite the severity of the presentation, the bilirubin concentration is only (relatively) mildly elevated in contrast to other etiologies of ALF. For patients with known or suspected acetaminophen overdose within 4 hours of presentation, activated charcoal should be given just prior to the start of NAC dosing.15 This administration of activated charcoal does not affect the metabolism of the intravenous form of NAC.16 Oral NAC can be administered to patients with no encephalopathy or grade 1 encephalopathy. However, patients with grade 2 and greater encephalopathy should receive intravenous NAC. Although NAC should be given as early as possible, it still may be of value up to 48 hours after ingestion. If the oral form is the only option, the recommended dosing is 140 mg/kg followed by 70 mg/kg by mouth every 4 hours for 17 doses. The intravenous form of NAC includes a loading dose of 150 mg/kg in 5% dextrose over 15 minutes; the maintenance dose is 50 mg/kg given over 4 hours followed by 100 mg/kg administered over www.turner-white.comGastroenterology Volume 14, Part 6 3 Acute Liver Failure Table 4. King’s College Hospital Criteria for Risk of Death in Fulminant Hepatic Failure Acetaminophen-induced disease All other causes of fulminant hepatic failure Arterial pH <7.3 after adequate fluid resuscitation (independent Prothrombin time >100 sec (INR >6.5) (independent of the grade of of the grade of encephalopathy) encephalopathy) OR OR Grade III or IV encephalopathy and Any 3 of the following variables are present (independent of the grade of encephalopathy): Prothrombin time >100 sec (INR >6.5) and 1. Age <10 years or >40 years Serum creatinine >3.4 mg/dL (300 mmol/L) 2. Etiology: non-A, non-B hepatitis, halothane hepatitis, idiosyncratic drug reactions 3. Duration of jaundice before onset of encephalopathy >7 days 4. Prothrombin time >50 sec (INR >3.5) 5. Serum bilirubin >18 mg/dL (308 mmol/L) 16 hours, or 6 mg/kg/hr.17,18 NAC should be given in cases of ALF in which acetaminophen ingestion is possible or when knowledge of circumstances surrounding admission is inadequate but aminotransferases suggest acetaminophen poisoning.15 There has been controversy in the literature regarding prolonged NAC administration for more than 72 hours. In a randomized study, NAC administration in nonacetaminophen ALF improved survival; this was shown during early administration in grade I and grade II encephalopathy.19 NAC has interestingly also been shown to improve transplant-free survival even in patients with ALF not due to acetaminophen. This has led to the recommendation that NAC be considered in all patients with ALF. DRUG-INDUCED LIVER Injury AND DRUGINDUCED ACUTE LIVER FAILURE An important part of determining the etiology of DILI or drug-induced acute liver failure (DILF) is a detailed medication profile including dietary and herbal supplements and length of therapy. DILI can be subclinical and chronic and progress to DILF20 4 Hospital Physician Board Review Manual and can appear solely as hepatocellular or cholestatic injury or as mixed injury.4 DILI is a diagnosis of exclusion; usually the AST and ALT levels are elevated 2 to 3 times the upper limit of normal. There are over 300 medications implicated in causing DILI and DILF. In a recent prospective study that excluded acetaminophen as a cause of ALF and evaluated 300 patients over 3 years, a single medication was implicated in 73% of DILI cases, dietary causes in 9%, and multiple agents in 18%.20 In this study, DILI was characterized as mild in 27%, moderate in 19%, moderate-hospitalized in 33%, and severe in 13%, and resulted in liver transplantation or death in 6%. The overall incidence of ALF secondary to drugs is approximately 13%.7 These implicated medications may be dose-dependent, and patients will have extrahepatic manifestations of failure such as cerebral edema, encephalopathy, coagulopathy, hemodynamic instability, renal failure, and metabolic disturbances.7 Many drug classes have been implicated in DILI and DILF, and the current practice recommendations include cessation of medication, determining specific ingredients (in dietary www.turner-white.com Acute Liver Failure and herbal supplements), and considering NAC administration.15 Common medications leading to DILI and DILF are listed in Table 5. VIRAL HEPATITIS The viruses that mainly affect the liver and those associated with systemic infections that have liver involvement vary in incidence and geographic location. These viruses include hepatitis A, hepatitis B, hepatitis C, hepatitis D, hepatitis E, cytomegalovirus (CMV), Epstein-Barr virus, herpes simplex virus, parvovirus B19, varicella-zoster virus, enterovirus, and adenovirus. The viruses that affect the liver cause hepatocellular injury in 1 of 2 clinical settings: acute viral transmission or reactivation of latent virus in an immunosuppressed patient. Hepatitis A and E Hepatitis A virus (HAV) has an incubation period of 2 to 4 weeks, is self-limited in a healthy individual, and does not have cross-reactivity with the other hepatitis viruses.4 Approximately 5% of patients with acute hepatitis A and E requiring admission to a hospital will develop ALF.2 Hepatitis A and E are transmitted via the fecal-oral route and have a higher incidence in developing countries. One study of an urban outbreak of hepatitis A in Tennessee (1995) that included 256 patients in 15 acute care hospitals found that patients over 40 years of age had a higher risk of complications, which included death in 5 patients (2%).21 According to the Centers for Disease Control and Prevention, 20,000 to 36,000 cases of acute HAV infections were reported in the United States per year during the period 1980 to 1995; the incidence declined significantly (5683 cases in 2006) secondary to childhood vaccination introduced in 1995.22 A similar study performed in the United States found 3.1% of ALF cases were due to HAV infection.23 conjugation Glucuronide moiety (Nontoxic) conjugation Sulfate moiety P450 (Nontoxic) (2E1) Acetaminophen N-acetyl-p-benzo-quinone imine (NAPQI) (Toxic) NAC Glutathione Cysteine and mercapturic acid conjugates (Nontoxic) Figure. Metabolic pathways of acetaminophen. NAC = N-acetylcysteine. A prospective evaluation which followed patients with chronic hepatitis B and C who were seronegative for hepatitis A over a 7-year period suggested that once a superinfection with HAV occurred, there was an increase in ALF for patients with chronic hepatitis C. For this reason, hepatitis A vaccination is recommended in patients with chronic hepatitis C.24 In order to make a diagnosis of hepatitis A, immunoglobulin M (IgM) HAV antibodies must be identified in the serum on laboratory testing. Hepatitis E virus (HEV) is transmitted via the fecal-oral route and has a higher occurrence in developing countries, with a mortality of up to 54%.25 HEV is a leading cause of ALF in pregnant women in endemic areas of India and Southeast Asia. Various mechanisms to explain this increase in the severity of this disease in pregnancy have been proposed. One theory suggested that low levels of CD4 cells and high levels of CD8 cells in addition to high circulating steroid hormones contributed to the increase in mortality in pregnant women compared to nonpregnant women with ALF secondary to acute hepatitis E.26 www.turner-white.comGastroenterology Volume 14, Part 6 5 Acute Liver Failure Table 5. Drugs Classes Associated with Drug-Induced Liver Failure Chemotherapy Gemcitabine, carboplatin, flutamide Antihypertensive/antiarrhythmic NSAIDs and analgesics Antifungal/Antimicrobial/HAART Captopril, enalapril, lisinopril/amiodarone Acetaminophen, ibuprofen, diclofenac, oxaprozin Terbinafine, ketoconazole, cotrimoxazole/ciprofloxacin, ofloxacin, trimethoprim-sulfamethoxazole, rifampin-isoniazid, amoxicillin-clavulanate, minocycline, dapsone, lamotrigine/didanosine, efavirenz Valproic acid, carbamazepine, phenytoin Kava kava, he shou wu, ma huang, hydroxycut, germander Cocaine, ecstasy Psychiatric Herbal and dietary supplements Illicit drugs Hepatitis B, C, D The hepatitis B virus (HBV) can be reactivated in the setting of immunosuppressive therapy, chemotherapy, abrupt discontinuation of HBV antiviral therapy, and hepatitis D coinfection or superinfection of a patient with chronic hepatitis B. Hepatitis B is endemic to Southeast Asia, the Middle East, and sub-Saharan Africa. In these areas, age plays an important role in chronicity of disease. Chronic infection occurs in 90% of children younger than 5 years and 30% to 50% of those older than 5 but less than 18, while 90% of infected adults will clear the virus.27 In acute HBV infection, the nucleoside analog lamivudine may be considered for treatment, but there have been conflicting studies of its efficacy.12,28–39 Hepatitis B incidence is on the decline, reflecting the vaccination initiative which was started in 1982 for people in endemic areas and in 1991 for all children.40 However, patients on active antiviral therapy for chronic hepatitis B can develop ALF secondary to noncompliance with their hepatitis B medication. This situation should prompt an evaluation of the current resistance profile of their medication with reinitiation of HBV antiviral therapy as soon as possible. It is currently recommended that patients undergoing immunosuppressive therapy be treated for at least 6 months after completion of im6 Hospital Physician Board Review Manual munosuppressive therapy.41 In the setting of newly diagnosed HIV along with acute hepatitis B, highly active antiretroviral therapy (HAART) should target both viruses and include a combination of lamivudine plus tenofovir or emtricitabine plus tenofovir.41 Hepatitis D virus (HDV) is a defective virus that is dependent on HBV for assembly and secretion. HDV superinfection of a patient with chronic hepatitis B can lead to ALF in endemic areas of the world, although the incidence has declined.42 Travel to areas of northern Europe, Asia, the Mediterranean, northern South America, or Africa should prompt testing for hepatitis D.43 Patients who acquire HBV and HDV simultaneously (co-infection) and survive to develop chronic liver disease have a higher risk of developing complications secondary to cirrhosis and hepatocellular carcinoma compared to monoinfected chronic hepatitis B patients. In either case, co- or superinfection, the risk of ALF is greater than that of acute hepatitis B monoinfection alone.44,45 Acute hepatitis C causing ALF remains controversial. However, a Taiwanese study showed that patients with chronic hepatitis B that are subsequently exposed to hepatitis C virus (HCV) have a higher risk of developing ALF.46 Despite this, other authors evaluating ALF in 308 patients reported by 17 tertiary care centers within a 41-month period found that a majority of the cases were attributed to www.turner-white.com Acute Liver Failure acetaminophen (39%) or hepatitis A and B (12%). This study did not report hepatitis C as a causative agent in any patient.7 Other Viruses Viruses such as parvovirus B19, varicella-zoster virus, enterovirus, and adenovirus are rare causes of ALF. Herpes virus–induced ALF usually presents in immunosuppressed or pregnant patients or in the setting of malignancy, and skin lesions are present in 57% of cases.47 Prompt administration of acyclovir 5 to 10 mg/kg every 8 hours is the recommended treatment.48 CMV infection can affect immunosuppressed patients, especially in the first 3 months following an allograft transplant; administration of ganciclovir should be considered in this population. The major risk factors in this patient population are medication noncompliance and CMV-seropositive donor and CMV-seronegative recipient.49 Lung and heart transplant patients are at the highest risk, followed by liver transplant patients; kidney transplant patients are at lower risk.50 WILSON DISEASE ALF secondary to Wilson disease primarily affects children or young adults without history of any underlying liver condition. The classical hallmarks of the disease are laboratory findings including low ceruloplasmin, uric acid, and alkaline phosphatase, increased urinary copper, and Coombsnegative hemolytic anemia with associated renal failure.51 Unfortunately, the diagnosis of Wilson disease is often one of exclusion. Most frequently, the serum ceruloplasmin can be normal or even high. In addition, it takes days to obtain the results of a 24-hour urinary copper test. Kayser-Fleischer rings are present in only 50% of patients. A serum albumin to alkaline phosphatase ratio less than 2.0 is 100% specific and sensitive to diagnose Wilson disease.52 Chelating therapy is not effective in the acute setting and has been shown to cause hypersensitivity reactions.52,53 A fulminant Wilson disease patient must be referred urgently for transplantation since survival without transplantation is approximately zero. In addition, the removal of the abnormal liver will cure Wilson disease. AUTOIMMUNE HEPATITIS Acute autoimmune hepatitis primarily affects young females (mean age 41) who are overweight (body mass index BMI ≥30) and do not have a preexisting liver condition.54 The majority of patients (70%) will have positive antinuclear and anti-smooth muscle antibodies, representing type I autoimmune hepatitis. Approximately 3% will be positive for the anti-liver/ kidney microsome (LKM) or anti-soluble liver antigen (SLA) antibodies, representing type II and III autoimmune hepatitis, respectively. The remainder are positive for anti-mitochondrial antibody, representing a potential overlap of disease states.54 Occasionally, these markers are negative, and if clinical suspicion for autoimmune hepatitis is high, a liver biopsy should be performed.53 Corticosteroids should be initiated promptly (40–60 mg/day) and should be continued while awaiting liver transplantation.55 Autoimmune hepatitis, unlike Wilson disease, may recur after liver transplantation, and these patients may have higher rates of acute and chronic rejection compared to patients who undergo liver transplantation for other diseases.56,57 PREGNANCY AND ALF Acute Fatty Liver of Pregnancy (AFLP) AFLP is a condition which occurs in the third trimester of pregnancy and is potentially fatal.58 The initial presentation is similar to flu-like illness with nausea, fatigue, anorexia, and abdominal pain which progresses to fever and jaundice.59 Patients www.turner-white.comGastroenterology Volume 14, Part 6 7 Acute Liver Failure with AFLP may develop altered mental status, disseminated intravascular coagulopathy, gastrointestinal bleeding, and acute renal failure, and thus prompt stabilization of the mother and delivery of the fetus are required.60 Although liver biopsy is rarely performed, a stain with oil red O is specific to detect fat molecules.61 The characteristic pattern on liver biopsy consists of a microvesicular fatty infiltration of the liver without any microscopic evidence of inflammation or necrosis. Liver transplantation should be considered in patients who do not improve post delivery. Hemolysis, Elevated Liver enzymes, Low Platelet (HELLP) Syndrome HELLP is an obstetric emergency, and it can present before or after delivery.62 The presenting symptoms of this entity include malaise, nausea and vomiting, and right upper quadrant pain. The largest retrospective study to date examined 442 patients with HELLP and found a maternal mortality rate of 1.1% in patients with hypertension and proteinuria.62 The elevations in AST and ALT do not correlate with the severity of disease. The mainstay of treatment includes supportive care and prompt delivery. There are reports of complications in subsequent pregnancies, but no increase in risk of developing HELLP syndrome a second time.63 ACUTE ISCHEMIC INJURY Acute ischemic injury, or “shock liver,” causes diffuse hepatic changes which occur in the setting of cardiac arrest, heart failure, and hypotension and is characteristically seen in the intensive care setting.64 Levels of lactate dehydrogenase, AST, and ALT are markedly elevated, reaching up to 25 to 200 times the upper limit of normal, and usually peak at the third day and return to normal between 7 and 10 days.65 The distinguishing factor of this entity is that synthetic function is generally well preserved and mental status changes may be related to underlying hypotension and cerebral hypoperfusion rather than hepatic encephalopathy. The prognosis in patients with acute ischemic injury is determined by the treatment of the underlying cause, most notably cardiac function or systemic infection leading to hypotension.66 BUDD-CHIARI SYNDROME Budd-Chiari syndrome is characterized by outflow obstruction of the liver by thrombosis of one or more of the hepatic veins or inferior vena cava.67,68 Underlying causes such as a hypercoagulable state, malignancy, use of oral contraceptives, and infiltrative liver diseases such as abscesses have been reported in the literature.69–71 Patients who develop this syndrome along with ALF can be diagnosed either on Doppler ultrasound, magnetic resonance imaging, or computed tomography. Unfortunately, these patients tend to have a poor prognosis. The treatment options for acute BuddChiari include anticoagulation, thrombolysis, vascular intervention, and liver transplantation.72–75 MUSHROOM POISONING Ingestion of amatoxin-producing mushrooms, most commonly Amanita phalloides, can lead to ALF in approximately 72 hours.76 The early symptoms (hours) after ingestion include abdominal pain, nausea, vomiting, and diarrhea; activated charcoal may be effective within this timeframe. Progression to ALF occurs rapidly, and the administration of intravenous penicillin G and intravenous and oral silibinin are currently accepted as antidotes.77,78 Intravenous silibinin is not available in the United States, but an expedited application for this drug can be approved. www.turner-white.comGastroenterology Volume 14, Part 6 9 Acute Liver Failure MALIGNANCY Malignancies such as lymphoma, breast cancer, small cell lung cancer, melanoma, myeloma, and metastatic disease can infiltrate the liver.79–82 When malignancy infiltrates in the liver, it rarely causes ALF except in the setting of acute outflow obstruction such as in Budd-Chiari syndrome. Unfortunately, imaging of the liver in a patient who has a diffuse infiltrative pattern suggestive of ALF can be nondiagnostic. Prompt biopsy to tailor chemotherapy is the mainstay of management, and such patients are not considered liver transplant candidates.83 TREATMENT OF ACUTE LIVER FAILURE Management of a patient with ALF, after identifying the cause and initiating appropriate treatment, consists of supportive care in the ICU followed by expeditious transfer to a liver transplant center. Management of the multisystem organ failure with specific treatment tailored to addressing the changes in the central nervous system, systemic infection, coagulopathy, renal failure, and metabolic derangements, along with liver transplant considerations are the basis of care. CENTRAL NERVOUS SYSTEM The incidence of cerebral edema is approximately 50% to 85%, with cerebral herniation as a cause of death reported in 30% to 50% of patients.84–88 The cause of the cerebral edema is multifactorial, with eventual astrocyte dysfunction and increased permeability of the blood-brain barrier.89 A computed tomography (CT) scan of the head cannot reliably detect cerebral edema, especially early in the disease state, and a negative CT of the head does not exclude elevated intracranial pressure (ICP).84 The grade of hepatic encephalopathy in the setting of ALF correlates with worsening cerebral edema. 10 Hospital Physician Board Review Manual In one study, cerebral edema was not observed in grade I or II encephalopathy, but was found in 35% of those with grade III and 75% of those with grade IV encephalopathy.90 Grades of encephalopathy are defined in Table 3. In addition, the serum ammonia concentration is a very important predictor of the presence of cerebral edema (rare with levels <100 µmol/L, but often present with levels >150 µmol/L).91 The goal directed therapy in response to a change in mental status secondary to cerebral edema and increased ICP is important to minimize long-term cognitive defects in survivors. Grade I encephalopathy patients can be managed on a quiet medical ward with frequent neurologic exams performed. When there is progression to grade II encephalopathy, patients should be transferred to the ICU and sedatives avoided.15 Elevation of ICP due to frequent movement is a major concern,92 and endotracheal suction, tactile stimulation, and frequent patient turning should be avoided. Progression to grade III and IV encephalopathy warrants intubation, elevation of the head of the bed to 30 degrees, use of short-acting sedatives such as propofol or paralytics, and seizure precautions as indicated. Lactulose administration is used with caution as it may cause abdominal distention, lead to intravascular volume depletion, and may be a causative agent in development of toxic megacolon. In one study, the administration of lactulose may have increased survival time but had no impact on overall outcomes.93 Direct monitoring of the ICP is rarely performed since it has not been shown to lead to an overall increase in survival.94,95 If these devices are present to measure ICP and cerebral perfusion pressure (CPP = mean arterial pressure [MAP] – ICP), then the values should demonstrate an ICP ranging from 20 to 25 mm Hg with the CPP maintained above 50 to 60 mm Hg.96 www.turner-white.com Acute Liver Failure The specific treatment modalities to consider in treating an elevated ICP that is ≥25 mm Hg include mannitol, hyperventilation, barbiturates, and hypothermia. Once the diagnosis of elevated ICP is made, mannitol 0.5 to 1.0 g/kg via intravenous bolus is recommended as first-line therapy.97 Serum osmolarity should be measured every 6 hours and repeat boluses should be administered if the serum osmolarity is less than 320 mOsm/L.97 When the ICP continues to rise despite maximal medical therapy with mannitol, other modalities can be considered. The use of hyperventilation and hypertonic saline showed no survival benefit in patients with ALF.98,99 Despite having no survival benefit, hypertonic saline has been shown to reduce the risk of intracranial hypertension (ICH) in a randomized, controlled study.99 Barbiturate use in ALF has been shown to decrease ICH, but its side effects related to decreased hepatic clearance of the drug, such as hypotension, hypokalemia, and prolonged neurological suppression, may worsen the clinical condition of a septic patient.96,100 Inducing hypothermia has not been used widely in the setting of ALF, as this may also precipitate infection and coagulopathy.101,102 INFECTION One of the absolute contraindications to liver transplantation is bacterial, fungal, or viral infection.103 However, empiric antibiotic administration has not been shown to improve outcomes or survival in ALF.104 Practicing universal health precautions and screening for multidrug resistant organisms should be part of the routine care for patients with ALF. At the onset of infection based on surveillance cultures or worsening grade of encephalopathy with a suspected systemic inflammatory response syndrome (SIRS), antibiotics and antifungal therapy should be initiated.105–109 COAGULOPATHY AND BLEEDING Despite an often marked elevation of the INR, patients rarely bleed.90 The INR is an important marker for prognosis and should not be corrected unless clinically significant bleeding ensues.109 In addition, thrombocytopenia of a mild to moderate severity is typically seen. Based upon experience in patients with chronic liver disease (no studies are available for patients in ALF), expert opinion suggests 2 units of fresh frozen plasma should be transfused without a specific target INR value when planning an invasive procedure. In contrast, platelet transfusions should be given to target a platelet count greater than 60,000/mL.110,111 It is recommended to administer either an H2 blocker or proton pump inhibitor as prophylaxis against gastrointestinal bleeding in the presence of coagulopathy.112–114 HEMODYNAMICS Hypotension and renal failure are major concerns in patients with ALF. The infusion of norepinephrine to maintain a MAP of ≥65 mm Hg is currently recommended in patients with hypotension refractory to isotonic volume expansion.115 Low-dose dopamine has not shown any decrease in the incidence of renal failure in the setting of SIRS, and epinephrine can cause a decrease in blood flow to the mesenteric regions and potentially decrease hepatic blood flow; neither is a recommended treatment modality.116–118 Adrenal insufficiency occurred in approximately 62% of patients with ALF in one study regardless of etiology.119 One should consider hydrocortisone use as it may augment the effect of norepinephrine.120 RENAL FAILURE Approximately 80% of patients will develop 1 of 3 types of renal failure (prerenal, functional, or acute tubular necrosis) in the setting of ALF.121 The initial laboratory data (Table 2) should include evaluation of urine www.turner-white.comGastroenterology Volume 14, Part 6 11 Acute Liver Failure Table 6. UNOS Transplant Requirements for Adult in Acute Liver Failure to be Listed as Status 1A Age >18 Life expectancy <7 days Onset of encephalopathy within 8 weeks Absence of preexisting liver disease One of the following 3 criteria must be met while in the intensive care unit: Ventilator dependent On hemodialysis INR >2.0 electrolytes to determine an etiology and appropriate therapy should be initiated. Continuous hemodialysis rather than intermittent has been shown to improve oxygen tissue delivery and does not increase ICP.122 METABOLIC IMBALANCE AND NUTRITION Metabolic imbalance with concurrent acidosis and alkalosis along with hypoglycemia, hyponatremia, hypophosphatemia, and hypomagnesemia that occur in the setting of ALF must be corrected. In one report, hypophosphatemia correlated with higher survival rates in patients with acetaminophen toxicity; phosphate is taken up in the regenerating liver and used to make adenosine triphosphate, and thus hypophosphatemia may be a positive indicator.123 ALF is a state of negative nitrogen balance. Administration of enteral feeds via high caloric regimen is essential,124 with careful attention to resulting hyperglycemia, which may increase ICP.125 TRANSPLANT AND ARTIFICIAL SUPPORT The selection of patients for liver transplantation should be based on the King's College Criteria (Table 4).126,127 The positive predictive value, sensitivity, and specificity of these criteria for a poor out12 Hospital Physician Board Review Manual come were greater than 90% in multiple studies, but the criteria do not predict survival.128 In a retrospective study of 177 patients with ALF,128 49% underwent liver transplantation, 14% recovered with medical management, and the remainder died without liver transplantation. When placed on the United Network for Organ Sharing (UNOS) waiting list, patients with ALF are designated as status 1, which is the highest priority level for liver transplant (Table 6).129 Calculation of the MELD score, which encompasses serum creatinine, total bilirubin, and INR, will provide a 3-month mortality for patients with chronic liver disease. The MELD estimate of 3-month mortality has not been validated for patients with ALF. The 1- and 5-year survival for patients transplanted in a retrospective study that evaluated over 200 patients with fulminant hepatic failure were 73% and 63% with deceased donor transplant and 75% with living donor transplant.4,8 Artificial support such as the molecular adsorbents recirculation system (MARS) and bioartificial support systems are currently in clinical trials and require future studies to establish their efficacy. CONCLUSION ALF is a medical emergency and warrants intensive care management and transfer to a tertiary center for evaluation for liver transplantation. Etiology of the acute insult must be determined for more focused management. Multisystem organ failure, cerebral edema, metabolic derangements, infection, renal failure and hemodynamic support are the mainstays of therapy. BOARD REVIEW QUESTIONS Test your knowledge of this topic. Go to www.turner-white.com and select Gastroenterology from the drop-down menu of specialties. www.turner-white.com Acute Liver Failure REFERENCES 1. Fontana RJ. Acute liver failure including acetaminophen overdose. Med Clin North Am 2008;92:761–94. 2. Bernal W, Auzinger G, Dhawan A, Wendon, J. Acute liver failure. Lancet 2010;376:190–201. 3. Larson AM, Polson J, Fontana RJ, et al. Acetaminopheninduced acute liver failure: results of a United States multicenter; prospective study. Hepatology 2005;42:1364–72. 4. Schiff E, Sorrell M, Maddrey, W. Schiff’s diseases of the liver. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2006. 5. Farmer D, Anselmo D, Ghobrial M, et al. Liver transplantation for fulminant hepatic failure: experience with more than 200 patients over a 17-year period. Ann Surg 2003;237:666–76. 6. Campsen J, Blei AT, Emond JC, et al. Outcomes of living donor liver transplantation for acute liver failure: the adultto-adult living donor liver transplantation cohort study. Liver Transpl 2008;14:1273–80. 7. Ostapowicz GA, Fontana RJ, Schiodt FV, et al. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann Intern Med 2002;137:947–54. 8. Schiodt FV, Atillasoy E, Shakil AO, et al. Etiology and outcome for 295 patients with acute liver failure in the United States. Liver Transplant Surg 1999;5:29–34. 9. Lee WM. Acetaminophen and the U.S. Acute Liver Failure Study Group: lowering the risks of hepatic failure. Hepatology 2004;40:6–9. 10. Schiodt FV, Rochling FJ, Casey DL, Lee WM. Acetaminophen toxicity in an urban county hospital. N Engl J Med 1997;337:1112–7. 11. Farrell GC. Drug-induced liver disease. Edinburgh: Churchill Livingstone; 1994. 12. Roussos A, Koilakou S, Kalafatas I, et al. Lamivudine treatment for acute severe hepatitis B: report of a case and review of the literature. Acta Gastroenterol Belg 2008;71:30–2. 13. Khandelwal N, James LP, Sanders C, et al; the Acute Liver Failure Study Group. Unrecognized acetaminophen toxicity as a cause of indeterminate acute liver failure. Hepatology 2011;53:567–76. 14. Lee WM. Drug-induced hepatotoxicity. N Engl J Med 2003;349:474–85. 15. Lee WM, Larson AM, Stravitz RT. AASLD position paper: the management of acute liver failure: Update 2011. AASLD Guidelines 2011;1–23. 16. Sato RL, Wong JJ, Sumida SM, et al. Efficacy of superactivated charcoal administration late (3 hours) after acetaminophen overdose. Am J Emerg Med 2003;21:189–91. 17. Makin AJ, Wendon J, Williams R. A 7-year experience of severe acetaminophen-induced hepatotoxicity (19871993). Gastroenterology 1995;109:1907–16. 18. Bernal W, Wendon J, Rela M, et al. Use and outcome of liver transplantation in acetaminophen-induced acute liver failure. Hepatology 1998;27:1050–5. 19. Lee WM, Hyan LS, Rossaro L, et al. Intravenous N-acetylcysteine improves transplant-free survival in early stage non-acetaminophen acute liver failure. Gastroenterology 2009;137:856–64. 20. Chalasani N, Fontana R, Bonkovsky H, et al. Causes, clinical features, and outcomes from a prospective study of drug-induced liver injury in the United States. Gastroenterology 2008;135:1924–34. 21. Wilner IR, Mark DU, Howard SC, et al. Serious hepatitis a: an analysis of patients hospitalized during an urban epidemic in the United States. Ann Intern Med 1998;128:111–4 22. Advisory Committee on Immunization Practices (ACIP), Fiore AE, Wasley A, Bell BP. Prevention of hepatitis A through active or passive immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP).MMWR Recomm Rep 2006;55(RR-7):1–23. 23. Taylor RM, Davern T, Munoz S, et al. Fulminant hepatitis A virus infection in the United States: incidence, prognosis, and outcomes. Hepatology 2006;44:1589–97. 24. Vento S, Garofano T, Renzini C, et al. Fulminant hepatitis associated with hepatitis A virus superinfection in patients with chronic hepatitis C. N Engl J Med 1998;338:286–90. 25. Bhatia V, Singhal A, Panda SK, Acharya SK. A 20-year single-center experience with acute liver failure during pregnancy: is the prognosis really worse? Hepatology 2008;48:1577–85. 26. Jilani N, Das BC, Husain SA, et al. Hepatitis E virus infection and fulminant hepatic failure during pregnancy. J Gastroenterol Hepatol 2007;22:676–82. 27. World Health Statistics 2012. Geneva: WHO; 2012. Available at: http://www.who.int/gho/publications/world_health_ statistics/2012/en/ 28. Kumar M, Satapathy S, Monga R, et al. A randomized controlled trial of lamivudine to treat acute hepatitis B. Hepatology 2007;45:97–101. 29. Schmilovitz-Weiss H, Ben-Ari Z, Sikuler E, et al. Lamivudine treatment for acute severe hepatitis B: a pilot study. Liver Int 2004;24:547–51. 30. Miyake Y, Iwasaki Y, Takaki A, et al. Lamivudine treatment improves the prognosis of fulminant hepatitis B. Intern Med 2008;47:1293–9. 31. Torii N, Hasegawa K, Ogawa M, et al. Effectiveness and long-term outcome of lamivudine therapy for acute hepatitis B. Hepatol Res 2002;24:34. 32. Kondili LA, Osman H, Mutimer D. The use of lamivudine for patients with acute hepatitis B (a series of cases). J Viral www.turner-white.comGastroenterology Volume 14, Part 6 13 Acute Liver Failure Hepat 2004;11:427–31. 33. Hasan F, Owaid S, Ali M, et al. Lamivudine therapy for severe acute hepatitis B. J Hepatol 2005;42(suppl.2):178–9. 34. Lisotti A, Azzaroli F, Buonfiglioli F, et al. Lamivudine treatment for severe acute HBV hepatitis. Int J Med Sci 2008;5:309–12. 35. Delic D, Nesic Z, Prostran M, et al. Treatment of subacute hepatitis B with lamivudine: a pilot study in Serbia. Vojnosanit Pregl 2009;66:199–202. 36. Roznovský L, Orságová I, Kloudová A, Mrázek J. [Lamivudine therapy in patients with severe acute hepatitis B.] Klin Mikrobiol Infekc Lek 2007;13:59–65. Czech. 37. Chalupa P, Holub M. Favorable outcome of severe acute hepatitis B in a patient treated with antithrombin III and antiviral therapy. Clin Infect Dis 2009;49:481. 38. Tsai SH, Chang HM, Hsieh CB, et al. Acute fulminant hepatitis B in a patient with diabetic nephropathy treated successfully with concomitant lamivudine and molecular adsorbents recirculating system. J Infect 2006;53:e19–23. 39. Yu JW, Sun LJ, Yan BZ, et al. Lamivudine treatment is associated with improved survival in fulminant hepatitis B. Liver Int 2011;31:499–506. 40. Centers for Disease Control and Prevention. Guidelines for viral hepatitis surveillance and case management. Atlanta: CDC; 2005. http://www.cdc.gov/hepatitis/ PDFs/2005Guidlines-Surv-CaseMngmt.pdf. 41. Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007;45:507–39. 42. Gaeta GB, Stroffolini T, Chiaramonte M, et al. Chronic hepatitis D: a vanishing Disease? An Italian multicenter study. Hepatology 2000;32:824–7. 43. Hughes SA, Wedemeyer H, Harrison PM. Hepatitis delta virus. Lancet 2011;378(9785):73–85. 44. Fattovich G, Boscaro S, Noventa F, et al. Influence of hepatitis delta virus infection on progression to cirrhosis in chronic hepatitis type B. J Infect Dis 1987;155:931–5. 45. Fattovich G, Giustina G, Christensen E, et al. Influence of hepatitis delta virus infection on morbidity and mortality in compensated cirrhosis type B. The European Concerted Action on Viral Hepatitis (Eurohep). Gut 2000;46:420–6. 46. Chu C, C Yeh, Liaw Y. Fulminant hepatic failure in acute hepatitis C: increased risk in chronic carriers of hepatitis B virus. Gut 1999;45:613–7. 47. Rizzi R, Illei P. Herpes simplex virus hepatitis: case report and review. Clin Infect Dis 1997;24:334–8. 48. Peters DJ, Greene WH, Ruggiero F, McGarrity TJ. Herpes simplex induced fulminant hepatitis in adults: a call for empiric therapy. Dig Dis Sci 2000;45:2399–404. 49. Lautenschlager I. CMV infection, diagnosis and antiviral strategies after liver transplantation. Transpl Int 2009;22:1031–40. 50. Paya CV, Razonable RR. Cytomegalovirus infection after solid organ transplantation. In: Bowden RA, Ljungman P, 14 Hospital Physician Board Review Manual Paya CV, eds. Transplant Infections. Philadelphia: Lippincott, Williams & Wilkins;2003:298-325. 51. Gheorghe L, Popescu I, Iacob S, et al. Wilson’s Disease: a challenge of diagnosis. The 5-year experience of a tertiary center. Rom J Gastroenterol 2004;13:179–85. 52. Berman DH, Leventhal RI, Gavaler JS, et al. Clinical differentiation of fulminant Wilsonian hepatitis from other causes of hepatic failure. Gastroenterology 1991;100:1129–34. 53. Schilsky ML. Diagnosis and treatment of Wilson’s disease. Pediatric Transplantation 2002;6:15–19. 54. Stravitz RT, Lefkowitch JH, Fontana RJ, et al. Autoimmune acute liver failure: proposed clinical and histological criteria. Hepatology 2011;53:517–26. 55. Viruet EJ, Torres EA. Steroid therapy in fulminant hepatic failure secondary to autoimmune hepatitis. P R Heath Sci J 1998;17:297–300. 56. Hayashi M, Keefe EB, Krams SM, et al. Allograft rejection after liver transplantation for autoimmune liver disease. Liver Transpl Surg 1998;4:208–14. 57. Vogel A, Heinrich E, Bahr MJ, et al. Long-term outcome of liver transplantation for autoimmune hepatitis. Clin Transplant 2004;18:62–9. 58. Ko HH, Yoshida E. Acute fatty liver of pregnancy. Can J Gastroenterol 2006;20:25–30. 59. Simpson KR, Luppi CJ, O’Brien-Abel N. Acute fatty liver of pregnancy. J Perinat Neonatal Nurs 1998;11:35–44. 60. Kaplan MM. Acute fatty liver of pregnancy. N Engl J Med 1985;313:367–70. 61. Rolfes DB, Ishak KG. Acute fatty liver of pregnancy: a clinicopathologic study of 35 cases. Hepatology 1985;5:1149–58. 62. Sibai BM, Ramadan MK, Usta I, et al. Maternal morbidity and mortality in 442 pregnancies with hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome). Am J Obstet Gynecol 1993;169:1000–6. 63. Sibai RM, Ramadan MK, Chari RS, et al. Pregnancies complicated by HELLP syndrome (hemolysis, elevated liver enzymes and low platelets): subsequent pregnancy outcome and long term prognosis. Am J Obstet Gynecol 1995;172:125–9. 64. Bynum TE, Boitnott JK, Maddrey WC. Ischemic hepatitis. Dig Dis Sci 1979;24:129–35. 65. Gitlin N, Serio KM. Ischemic hepatitis: widening horizons. Am J Gastroenterol 1992;87:831–6. 66. Gibson PR, Dudley FJ. Ischemic hepatitis: clinical features, diagnosis and prognosis. Aust N Z J Med 1984;14:822–5. 67. Menon KV, Shah V, Kamath PS. The Budd-Chiari syndrome. N Engl J Med 2004;350:578–85. 68. Valla DC. Budd-Chiari syndrome and veno-occlusive disease/ sinusoidal obstruction syndrome. Gut 2008;57:1469–78. 69. Mitchell MC, Boitnott JK, Kaufman S, et al. Budd-Chiari syndrome: etiology, diagnosis and management. Medicine www.turner-white.com Acute Liver Failure (Baltimore) 1982;61:199–218. 70. Valla D, Le MG, Poynard T, et al. Risk of hepatic vein thrombosis in relation to recent use of oral contraceptives. A case-control study. Gastroenterology 1986;90:807–11. 71. Mahmoud AE, Elias E, Beauchamp N, Wilde JT. Prevalence of the factor V Leiden mutation in hepatic and portal vein thrombosis. Gut 1997;40:798–800. 72. Darwish Murad S, Valla DC, de Groen PC, et al. Determinants of survival and the effect of portosystemic shunting in patients with Budd-Chiari syndrome. Hepatology 2004;39:500–8. 73. Raju GS, Felver M, Olin JW, Satti SD. Thrombolysis for acute Budd-Chiari syndrome: case report and literature review. Am J Gastroenterol 1996;91:1262–3. 74. Wang ZG, Zhang FJ, Yi MQ, Qiang LX. Evolution of management for Budd-Chiari syndrome: a team’s view from 2564 patients. ANZ J Surg 2005;75(1-2):55–63. 75. Ringe B, Lang H, Oldhafer KJ, et al. Which is the best surgery for Budd-Chiari syndrome: venous decompression or liver transplantation? A single-center experience with 50 patients. Hepatology 1995;21:1337–44. 76. Berger KJ, Guss DA. Mycotoxins revisited: Part I. J Emerg Med 2005;28:53–62. 77. French LK, Hendrickson RG, Horowitz BZ. Amanita phalloides poisoning. Clin Toxicol (Phila) 2011;49:128–9. 78. Enjalbert F, Rapior S, Nouguier-Soule J, et al. Treatment of amatoxin poisoning: 20-year retrospective analysis. J Tox Clin Toxicol 2002;40:715–57. 79. Agarwal K, Jones DE, Burt AD, Hudson M, James OF. Metastatic breast carcinoma presenting as acute liver failure and portal hypertension. Am J Gastroenterol 2002;97:750–1. 80. Lowenthal A, Tur-Kaspa R, Brower RG, Almog Y. Acute liver failure complicating ductal breast carcinoma: two cases and literature review. Scand J Gastroenterol 2003;38:1095–6. 81. Krauss EA, Ludwig PW, Sumner HW. Metastatic carcinoma presenting as fulminant hepatic failure. Am J Gastroenterol 1979;72:651–4. 82. Montero JL, Muntane J, de las Heras S, et al. Acute liver failure caused by hepatic melanoma infiltration. J Hepatol 2002:37:540–1. 83. Woolf GM, Petrovic LM, Rojter SE, et al. Acute liver failure due to lymphoma. A diagnostic concern when considering liver transplantation. Dig Dis Sci 1994;391:1351–8. 84. Munoz SJ, Robinson M, Northrup B, et al. Elevated intracranial pressure and computed tomography of the brain in fulminant hepatocellular failure. Hepatology 1991;13:209–12. 85. Ware AJ, D’Agostino A, Combes B. Cerebral edema: a major complication of massive hepatic necrosis. Gastroenterology 1971;61:877–84. 86. Bismuth H, Didier S. Liver transplantation in fulminant and subfulminant hepatitis. In: Morris PJ, Tihey NL, eds. Transplan- tation reviews. Vol. 2. Philadelphia: WB Saunders Co.; 1988. 87. Nora LM, Bleck TP. Increased intracranial pressure complicating hepatic failure. J Crit Illness 1989;4:87–96. 88. Canalese J, Gimson AE, Davies C, et al. Controlled trial of dexamethasone and mannitol for the cerebral edema of fulminant hepatic failure. Gut 1982:23:625–9. 89. Haussinger D, Kircheis G, Fischer R, et al. Hepatic encephalopathy in chronic liver disease: a clinical manifestation of astrocyte swelling and low-grade cerebral edema? J Hepatol 2000;32:1035–8. 90. Munoz SJ. Difficult management problems in fulminant hepatic failure. Seminar Liver Dis 1993;13:395–413. 91. Bemeur C, Butterworth R. Liver-brain proinflammatory signally in acute liver failure: role in the pathogenesis of hepatic encephalopathy and brain edema. Metab Brain Dis 2013;20:145–50. 92. Wijdicks EF, Nyberg SL. Propofol to control intracranial pressure in fulminant hepatic failure. Transplant Proc 2002;34:1220–2. 93. Alba L, Hay JE, Angulo P, Lee WM. Lactulose therapy in acute liver failure. J Hepatol 2002;36:33A 94. Vaquero J, Fontana RJ, Larsen AM, et al: Complications and use of intracranial pressure monitoring in patients with acute liver failure and severe hepatic encephalopathy. Liver Transplant 2005;11:1581–9. 95. Keays RT, Alexander GJ, Williams R. The safety and value of extradural intracranial pressure monitors and fulminant hepatic failure. J Hepatology 1993;18:205–9. 96. Lidofsky SD, Bass NM, Prager MC, et al: Intracranial pressure monitoring and liver transplantation for fulminant hepatic failure. Hepatology 1992;16:1–7. 97. Marshall LF, Smith RW, Rauscher LA, et al. Mannitol dose requirements in brain injured patients. J Neurosurg 1978;48:169–72. 98. Ede RJ, Gimson AE, Bihari D, Williams R. Controlled hyperventilation in the prevention of cerebral oedema in fulminant hepatic failure. J Hepatol 1986;2:43–51. 99. Murphy N, Auzinger G, Bernal W, Wendon J. The effect of hypertonic sodium chloride on intracranial pressure in patients with acute liver failure. Hepatology 2002;39:464–70. 100. Jalan R, Olde Damink SW, Deutz NE, et al. Moderate hypothermia in patients with acute liver failure and uncontrolled intracranial hypertension. Gastroenterology 2004; 127:1338–46. 101. Rose C, Michalak A, Pannunzio M, et al. Mild hypothermia delays the onset of coma and prevents brain edema and extracellular brain glutamate accumulation in rats with acute liver failure. Hepatology 2000;31:872–7. 102. Varma V, Mehta N, Kumaran V, Nundy S. Indications and contraindications for liver transplantation. Int J Hepatol 2011;2011:121862. 103. Rolando N, Gimson A, Wade J, et al. Prospective controlled www.turner-white.comGastroenterology Volume 14, Part 6 15 Acute Liver Failure trial of selective parenteral and enteral antimicrobial regimen in fulminant liver failure. Hepatology 1993;17:196–201. 104. Rolando N, Philpott-Howard J, Williams R. Bacterial and fungal infection in acute liver failure. Semin Liver Dis 1996;16:389–402. 105. Rolando N, Harvey F, Brahm J, et al. Prospective study of bacterial infection in acute liver failure: An analysis of fifty patients. Hepatology 1990;11:49–53. 106. Rolando N, Harvey F, Brahm J, et al. Fungal infection: A common, unrecognised complication of acute liver failure. J Hepatol 1991;12:1–9. 107. Vaquero J, Polson J, Chung C, et al. Infection and the progression of hepatic encephalopathy in acute liver failure. Gastroenterology 2003;125:755–64. 108. Rolando N, Wade J, Davalos M, et al. The systemic inflammatory response syndrome in acute liver failure. Hepatology 2000;32(4 Pt 1):734–9. 109. Boks AL, Brommer EJ, Schalm SW, et al. Hemostasis and fibrinolysis in severe liver failure and their relation to hemorrhage. Hepatology 1986;6:79–86. 110. Tripodi A, Primignani M, Chantarangkul V, et al. Thrombin generation in patients with cirrhosis: the role of platelets. Hepatology 2006;44:440–5. 111. Drews R, Weinberger S. Thrombocytopenic disorders in critically ill patients. Am J Respir Crit Care Med 2000;162:347–51. 112. Shuman RB, Schuster DP, Zuckerman GR. Prophylactic therapy for stress ulcer bleeding: a reappraisal. Ann Intern Med 1987;106:562–7. 113. Macdougall BR, Bailey RJ, Williams R. H2-receptor antagonists and antacids in the prevention of acute gastrointestinal haemorrhage in fulminant hepatic failure. Two controlled trials. Lancet 1977;1:617–9. 114. Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation: Canadian Critical Care Trials Group. N Engl J Med 1998;338:791–7. 115. Stravitz RT, Kramer DJ. Management of acute liver failure. National Review Gastro Hep 2009;6:542–3. 116. Bellomo R, Chapman M, Finfer S, et al. Low-dose dopamine in patients with early renal dysfunction: A placebo- controlled randomised trial. Australian and New Zealand Intensive Care Society (ANZICS) Clinical Trials Group. Lancet 2000;356:2139–43. 117. De Backer D, Creteur J, Silva E, et al. Effects of dopamine, norepinephrine, and epinephrine on the splanchnic circulation in septic shock: Which is best? Crit Care Med 2003;31:1659–67. 118. Holmes CL. Vasoactive drugs in the intensive care unit. Curr Opin Crit Care 2005;11:413–7. 119. Harry R, Auzinger G, Wendon J. The clinical importance of adrenal insufficiency in acute hepatic dysfunction. Hepatology 2002;36:395–402. 120. Harry R, Auzinger G, Wendon J. The effects of supraphysiological doses of corticosteroids in hypotensive liver failure. Liver Int 2003;23:71–77. 121. Wilkinson SP, Blendis LM, Williams R. Frequency and Type of Renal and Electrolyte Disorders in Fulminant Hepatic Failure. Br Med J. 1974 February 2; 1(5900): 186–189. 122. Davenport A, Will EJ, Davison AM. Early changes in intracranial pressure during haemofiltration treatment in patients with grade 4 hepatic encephalopathy and acute oliguric renal failure. Nephrol Dial Transplant 1990;5:192–8. 123. Schmidt L, Dalhoff K. Serum phosphate is an early predictor of outcome in severe acetaminophen-induced hepatotoxicity. Hepatology 2002;36:659–62. 124. Walsh TS, Wigmore SJ, Hopton P, et al. Energy expenditure in acetaminophen-induced fulminant hepatic failure. Crit Care Med 2000;28:649–54. 125. Munoz SJ. Nutritional therapies in liver disease. Semin Liver Dis 1991;11:278–91. 126. Pauwels A, Mostefa-Kara N, Florent C, Levy VG. Emergency liver transplantation for acute liver failure: Evaluation of London and Clichy criteria. J Hepatol 1993;17:124–7. 127.Anand AC, Nightingale P, Neuberger JM. Early indicators of prognosis in fulminant hepatic failure: An assessment of the King’s criteria. J Hepatol 1997;26:62–8. 128. Shakil O, Kramer D, Mazariegos G, et al. Acute liver failure: clinical features, outcome analysis, and applicability of prognostic criteria. Liver Transplantation 2000;6:163–9. 129. Organ Procurement and Transplantation Network. Policy and procedure November 2011. February 15, 2011. http:// optn.transplant.hrsa.gov/ Copyright 2013 by Turner White Communications Inc., Wayne, PA. All rights reserved. 16 Hospital Physician Board Review Manual www.turner-white.com