Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
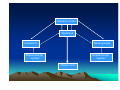
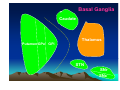
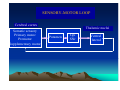
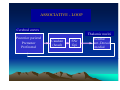
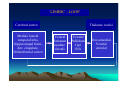
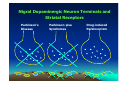
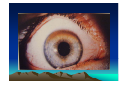
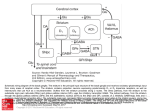
Movement Disorders and Extrapyramidal System Doç. Dr. Sibel Ertan İ.Ü. CTF. Nöroloji ABD. Motor System • • • • • I. neuron (corticospinal pathway) Extrapyramidal system (basal ganglia) Cerebellum Loops for praxis II. neuron: Anterior horn cells of the spinal cord Cranial cell nuclei in the brain stem • Peripheral nerve, motor cranial nerves • Neuromuscular junction • Muscle Definition Neurologic syndromes in which there is either an excess of movement, or a paucity of voluntary and automatic movements unrelated to weakness or spasticity. Most movement disorders are associated with pathologic alterations in the basal ganglia or their connections. But disorders of the • Cerebellum or its pathways • Cerebral cortex • Thalamus • Brain stem • Spinal cord • Peripheral nerves may also cause several movement disorders. Cerebral cortex Thalamus Basal ganglia Cerebellum Dopaminergic system Dopaminergic system Spinal cord Basal Ganglia Caudate Thalamus Putamen GPe GPi STN SNr SNc Basal ganglia subcortical nuclei: caudate putamen globus pallidus caudate, putamen & globus pallidus are named corpus striatum Caudate &putamen are named striatum globus pallidus & putamen are named lentiform nuclei Definition The term extrapyramidal system, coined by British neurologist Kinnier Wilson, refers to the basal ganglia and an array of brain stem nuclei (red nucleus, reticular formation etc.) to which they are connected. Striatum (caudate+putamen) is the principle receptive structure of the basal ganglia. Globus pallidus is the principle output structure of the basal ganglia. SENSORY-MOTOR LOOP Cerebral cortex Somatic sensory Primary motor Premotor Supplementary motor Thalamic nuclei Putamen Gpi SNr Ventral lateral ASSOCIATIVE - LOOP Cerebral cortex Thalamic nuclei Posterior parietal Premotor Prefrontal Caudate (head) SNr Gpi Ventral ant.,Dorsal medial LIMBIC - LOOP Cerebral cortex Medial, lateral temporal lobs, hippocampal form., Ant. cingulate, Orbitofrontal cortex Thalamic nuclei Ventral Striatum caudate (head) Ventral Pallidum Gpi SNr Dorsomedial, Ventral anterior OCULOMOTOR - LOOP Cerebral cortex Thalamic nuclei Posterior parietal Prefrontal Frontal eye field caudate (body) SNr Gpi Ventral ant., Dorsal medial • Diseases of the basal ganglia are associated with abnormal involuntary movements that typically occur at rest and disappear in sleep. • They are generally divided into two categories: Hyperkinetic and hypokinetic • The hyperkinetic variety is seen in such disorders as chorea, athetosis, ballism, dystonia, tremor, and tics. • The hypokinetic variety is seen largely in Parkinson’s disease. • Following anatomic loci for pathology are agreed on: - Substantia nigra in Parkinson’s disease - Caudate nucleus in chorea - Subthalamic nucleus in ballism - Caudate or lentiform nucleus (especially putamen) in dystonia Hypokinetic Disorders • Parkinsonism Six cardinal features: 1. Tremor at rest 2. Rigidity 3. Bradykinesia-hypokinesia 4. Flexed posture 5. Loss of postural reflexes 6. Freezing phenomenon • Tremor, rigidity, and flexed posture are referred positive phenomena. • Bradykinesia, loss of postural reflexes, and freezing are negative phenomena. Rest Tremor • 4-5 Hz • Present in the extremities, almost always distally • Classic “pill-rolling” tremor involves the thumb and the forefinger • Rest tremor disappears with action but reemerges as the limb maintain a posture. • Rest tremor is also common in the lips, chin, and tongue • Rest tremor of the hands increases with walking • Stress worsens the tremor Rigidity • Increased resistance (muscle tone) to passive movement elicited when the exami.ner moves the patient’s limbs, neck or trunk • Equal in all directions • The underlying tremor may cause “cogwheeling” Flexed posture • Commonly begins in the arms and spreads to involve the entire body • Striatal hand • Striatal toe • Lateral tilting of the trunk is common Bradykinesia • Slowness of movement, difficulty in initiating a movement, and loss of automatic movement • Hypokinesia is the reduction in amplitude of movement Loss of postural reflexes • Pulltest is positive • With progress of the disease frequent fallings • The patient collapses into the chair on attempting to sit down (sitting en bloc) Freezing • Inability to perform active movements (motor block) • Often involves the legs when walking but can also involve eyelid opening,speaking and writing. The many causes of parkinsonism are divided into four categories: 1.Idiopathic 2. Symptomatic 3. Parkinson-plus syndromes 4. Heredodegenerative diseases The core biochemical pathology in parkinsonism is decreased dopaminergic neurotransmission in the basal ganglia. • Degeneration of the nigrostriatal dopamine system • Degeneration of the striatum with loss of dopamine receptors • Drug induced parkinsonism as the result of blockade of dopamine receptors. Nigral Dopaminergic Neuron Terminals and Striatal Receptors Parkinson’s Disease Parkinson-plus Syndromes Drug-induced Parkinsonizm Parkinson’s disease (primary parkinsonism) • Degeneration of the neuromelanin-containing neurons in the brain stem, especially in substantia nigra pars compacta and in the locus ceruleus. • Many of the surviving neurons contain eosinophilic cytoplasmic inclusions known as Lewy bodies. • By the time symptoms appear, the substantia nigra already has lost about 60% of dopaminergic neurons and the dopamine content in the striatum is about 80% less than normal. Parkinson’s disease (primary parkinsonism) • PD makes up approximately 80% of cases of parkinsonism. • Mean age at onset in both sexes is 55 years (range:20-80). • Male/female = 3/2. • Prevalence ≈ 160/100.000 and incidence 20/100.000/yr. • The cause of PD is unknown. Parkinson’s disease (primary parkinsonism) Treatment • Treatment is aimed at controlling symptoms because no drug or surgicl approach unequivocally prevents progression of PD. • Treatment is lifelong. • Treatment includes pharmacotherapy, physiotherapy and surgery. Parkinson’s disease (primary parkinsonism) Treatment Therapeutic choices for Parkinson’s disease Medications Dopamine precursor: levodopa (LD)±carbidopa or benserazide Dopamine agonists: bromocriptine, pergolide, pramipexole, ropinirole, apomorphine, cabergoline. Catecholamine-O-methyl transferase inhibitors:tolcapone and entacapone. Dopamine releaser: Amantadine. Monoamine oxidase type B inhibitor: selegiline. Anticholinergics:trihexyphenidyl, benztropine, biperidene... Antihistaminics:diphenhydramine, orphenadrine, phenindamine Parkinson’s disease (primary parkinsonism) Treatment Therapeutic choices for Parkinson’s disease Surgery Ablative surgery:Thalamotomy, pallidotomy. Restorative surgery:Embryonic dopaminergic tissue transplantation Deep brain stimulation:Thalamic stimulation, pallidal stimulation, subthalamic stimulation Parkinson’s disease (primary parkinsonism) Treatment • All symptomatic drugs can induce side effects, and if a patient is not troubled socially or occupationally by mild symptoms, dru therapy can be delayed until symptoms become more pronounced. • LD is the most effective drug, BUT 75% of patients have serious complications after 5 years of LD therapy. • Younger patients, in particular, are more likely to show response fluctuations. • DOPA-SPARING STRATEGY:Other antiparkinsonian drugs should be used first to delay the introduction of LD. • Selegiline delays the need for LD therapy by an average of 9 months. Hyperkinetic Disorders • Tremor * Involuntary oscillations of a body part produced by alternating or synchronous contractions of reciprocally innervated muscles. * Physiological tremor These tremors are very small amplitude and are demonstrable only by means of accelerometer. Enhanced physiological tremor: medical conditions, drugs, anxiety, fear… * Essential tremor ET Typically a postural tremor (4-12 Hz) but may be accentuated by goal-directed movements. The site of involvement in most cases is the hands and it is frequently asymmetric initially. * Parkinsonian tremor Tremor at rest, at a frequency of 4-5 Hz, is the most characteristic and the most prominent type of tremor in PD, but postural and kinetic tremor are also frequently seen. Onset of the tremor is usually in one of the hands; rarely, it may begin in the legs. * Intention tremor Rhythmic involuntary oscillations that undergo exacerbation as the hand or foot approaches the target of a voluntary movement. It indicates involvement of the cerebellum or its connections. • Chorea (“dance”) Characterized by sudden, frequent involuntary, arrhythmic, purposeless, and quick jerks of the trunk, extremities, and head associated with facial grimaces. They are usually distal and of low amplitude. Causes of chorea are hereditary, autoimmune, vascular, metabolic, toxic, inflammatory or drug induced. • Athetosis (“without position”) Slow, writhing, continuous, wormlike movements of the distal parts of the extremities, chiefly the fingers, which show bizarre posturing. • Ballism (“jump or throw”) Sudden, quick, continuous, unusually violent, and flinging in nature. Usually confined to the contralateral vascular lesion in the subthalamic nucleus. • Dystonia (“bad tone”) Twisting, slow, contorting, involuntary movement, that is somewhat sustained and often repetitive. Dystonia can involve any part of the body. Dystonia is classified as (1) focal, (2) segmental, (3)multifocal, (4) hemidystonia, (5) generalized • Myoclonus Sudden shock-like muscle contractions. They can be focal, multifocal, or generalized. Myoclonus may be regular and rhythmic like tremor, but it is usually random and irregular like chorea. It differs from tremor in that there are visible pauses in between the jerks. It differs from chorea, which is flowing and resembles fragments of normal movements. Tics can resemble myoclonus but are voluntarily supressible for short periods; furthermore, an inner buildup of tension occurs during the supression of tics. • Tourette syndrome Characterized by motor and vocal tics. Motor tics are sudden, brief, involuntary movements involving muscles in different body parts such as eye blinking and shoulder shrugging. Vocal tics consist of gutteral sounds, grunts, or verbalization of words and phrases. Motor manifestations are often associated with behavioral abnormalities such as attention defisits and compulsive ritualistic behaviours. • Akathisia The motor activity in akathisia is described by patients as a voluntary effort to relieve uncomfortable sensations. Akathisia is usually expressed as changes in body position, standing, or pacing. In milder forms this can be voluntarily suppressed. In severe cases the need for motor activity is beyond control. Wilson disease (Hepatolenticular degeneration) • Autosomal recessive disorder with the gene being located on the long arm of chromosome 13. • The gene encodes a copper transporting P-type ATPase that is expressed in liver and kidney • Two fundamental defects: 1.reduced biliary transport of copper, 2.impaired formation of plasma ceruloplasmin • Free Cu in serum is increased • Overflow of copper from the liver produces accumulation in other organs, mainly in brain, kidney, and cornea . Wilson disease (Hepatolenticular degeneration) • In cornea, copper is deposited close to the endothelial surface of the Descement membrane (Kayser-Fleischer ring; most important diagnostic feature) • Symptoms begin between the ages of 11 and 25 years • Wilson disease is a disorder of motor function; there are no sensory symptoms and reflex alterations. • Symptoms of basal ganglia damage usually predominate but cerebellar symptoms may occasionally be in the foreground. • Tremors and rigidity are the most common early signs. • Seizures can occur at any stage of the disease. Wilson disease (Hepatolenticular degeneration) Treatment • Initial phase of the treatment (toxic copper levels are brought under control) Penicllamine Ammonium tetrathiomolybdate Triethylene tetramine dihydrohloride (trientine) • Maintenance therapy Zinc acetate Trientine + Zinc acetate