Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
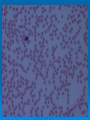
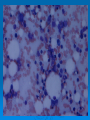
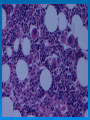
Severe Thrombocytopenia: Three VA cases Sarah Walter, M.D. Thrombocytopenia Thrombocytopenia is defined as a platelet count of < 150,000/ μL Due to: Increased destruction Sequestration Decreased production Thrombocytopenia Systematic approach to evaluating patients: History (associated illness, drugs, specific symptoms) Physical exam (anomalies, hepatosplenomegaly, infection, tumor, lymphadenopathy, bleeding) Careful interpretation of the complete blood count and examination of peripheral smear • If diagnosis not made, consider bone marrow examination with needle aspiration and biopsy Case 1 Case 1 49 year old female who presented to the Dermatology clinic with a petechial rash on her legs. She denied vaginal or mucosal bleeding. History of depression and PTSD treated with ziprasidone, trazadone, vanlafaxine, clonazepam. And she recently started carbamazepine 2 weeks prior. Case 1 Pre-drug lab values (2 weeks ago): WBC: 6.5 x 1000/μL (4.5 – 11.0) RBC: 3.9 M/μL (4.6 – 6.2) Plt: 272 x 1000/μL (150 – 400) Hgb: 12.2 g/dL (14.5 – 18.1) Hct: 35.2% (42 – 54) MCV: 90.4 fL (80 – 100) MCH: 31.3 pg (28 – 34) RDW: 12.7% (11.5 – 14.5) Laboratory data at time of visit: WBC: 4.6 x 1000/μL (4.5 – 11.0) RBC: 4.45 M/μL (4.6 – 6.2) Plt: 3.32 x 1000/μL (150 – 400) Hgb: 12.6 g/dL (14.5 – 18.1) Hct: 39.5% (42 – 54) MCV: 88.9 fL (80 – 100) MCH: 28.4 pg (28 – 34) RDW: 12.8% (11.5 – 14.5) Case 1 Additional pertinent laboratory data: PT: 11.9 sec (10.8 – 13.7) aPTT: 19.9 sec (21.6 – 34.2) Occult blood: Positive UA: Negative for blood Fe: 93 μg/dL (35 – 145) TIBC: 314 μg/dL (275 – 400) Ferritin: 133 ng/mL (25 – 180) Case 1 Smear: Case 1 Differential diagnosis: Drug-induced thrombocytopenia ITP Infectious (viral) TTP DIC Case 1 Carbamazepine was discontinued. Pt. received 1 unit of platelets (posttransfusion count: 13.3 1 week following, platelet count 383. Case 1 Diagnosis: Drug-induced thrombocytopenia: The main differential diagnosis in a druginduced thrombocytopenia is ITP. Drug exposure is the cause of 5-20% of thrombocytopenias Typically see the effect approximately 14 days after starting the medication Drug-Induced Thrombocytopenia Mechanism of various blood dyscrasias due to drugs: Interference with hematopoiesis, bone marrow suppression Drug induced antibodies Commonly seen with the psychotropic drugs, quinidine, sulfonamides, and gold • Study by Stübner et al (2004), found that clozapine was most common psychotropic drug to cause blood dyscrasias (0.18%) followed by carbamazepine (0.14%). Drug-Induced Thrombocytopenia Mechanisms of drug-dependent antibody formation: Accelerated platelet destruction due to drugdependent antibody • Reversible drug binding to one of the platelet surface glycoproteins (GP Ib/IX, GP IIb/IIIa) causing conformational change, resulting in the exposure of a neoepitope, expressed by a sequence that is normally concealed within the hydrophobic domain of the protein. • Molecular structure of the drug becomes an integral part of the new antigenic epitope There are no good laboratory tests to detect these drug-induced antibodies. Drug-Induced Thrombocytopenia Criteria to make diagnosis: 1) Candidate drug preceded thrombocytopenia AND recovery from thrombocytopenia was complete and sustained after the drug was discontinued. 2) The candidate drug was the only drug used prior to the onset of thrombocytopenia OR other drugs were continued or reintroduced after discontinuation of the candidate drug with a sustained normal platelet count. 3) Other etiologies for thrombocytopenia were excluded. 4) Reexposure to the candidate drug resulted in recurrent thrombocytopenia. Definite (Level 1): meet criteria 1, 2, 3, 4 Probable (Level 2): meet criteria 1, 2, 3 Drug-Induced Thrombocytopenia Thrombocytopenia associated with carbamazepine usually appears 14 to 16 days after initiation of drug. The platelet count completely resolved in all cases 7 days after after the drug was discontinued. Gold induced thrombocytopenia doesn’t follow this pattern, have persistently low platelets for months because of prolonged retention of gold salts Case 2 Case 2 24 year old African American female presented with complaints of: Easy bruising x 1 month Heavy menses 1-2 episodes of fever in the past month 2 days of cervical lymphadenopathy (resolved) Occasional night sweats No weight loss Case 2 Initial laboratory findings: WBC: 3.15 x 1000/μL (4.5 – 11.0) RBC: 3.26 M/μL (4.6 – 6.2) Plt: 3.16 x 1000/μL (150 – 400) Hgb: 8.80 g/dL (14.5 – 18.1) Hct: 26.7% (42 – 54) MCV: 81.8 fL (80 – 100) MCH: 27.0 pg (28 – 34) RDW: 16.1% (11.5 – 14.5) Abs Neutrophil: 1.63 x 1000/μL (1.8 – 7.8) Case 2 Smear Case 2 Differential diagnosis of pancytopenia with severe thrombocytopenia: Marrow infiltrative process (i.e. leukemia, lymphoma, metastatic disease) Idiopathic Thrombocytopenic Purpura (ITP) • Why the neutropenia and anemia? Next step, bone marrow biopsy. Case 2 Diagnosis: ITP Iron deficiency anemia, secondary to menometrorrhagia from low platelets Benign neutropenia of African Americans Low absolute neutrophil count seen in African Americans. No increased risk of infection. Case 2 Patient received steroids, IVIG x1, platelet transfusions. 1 week following, repeat CBC with a platelet count of 35 ITP Epidemiology of ITP: Incidence of 3-5 per cases 100,000 persons Onset typically adults aged 20-40 years Female predominance ITP Differential diagnosis: Diagnosis of exclusion, need to exclude drug-induced thrombocytopenia Familial thrombocytopenia • Check family history of low platelets unresponsive to treatment for ITP HIV-ITP Thrombotic thrombocytopenic purpura (TTP) Spurious thrombocytopenia resulting from platelet clumping • Always look at the peripheral smear of a patient with thrombocytopenia ITP Mechanism: Patients platelets are coated with IgG antibodies the recognize the platelet surface glycoproteins. Tissue macrophages recognize the Fc receptor, and phagocytose the platelet-AB complex. May also have reduced megakaryocyte production secondary to autoantibodies against megakaryocytes. Most frequent target antigens include GP Ib/IX/V and GP IIb/IIIa ITP Diagnosis: Diagnosis of exclusion Should exclude other causes of thrombocytopenia Review the peripheral smear Bone marrow examination if atypical Detection of anti-platelet antibodies(49-66% sensitive, 78-92% specific, interlaboratory agreement 55-67%) (not readily used) Flow cytometry to detect platelet associated autoantibodies (still being investigated but may be promising) ITP Diseases and disorders associated with ITP: HIV • Circulating immune complexes may nonspecifically deposit on platelet membrane, and are then cleared from system • Direct infection of megakaryocytes by HIV infection impairs platelet production Hepatitis C ?? H. pylori (still being debated) • Thought is that some strains of H. Pylori express the Lewis (Le) antigen. The Le antigen may adsorb the the platelet surface and serve as a target for anti-Le antibodies. SLE • The patient had elevated ANA titer (1:2500) (still to be worked up) ITP Treatment: Steroids Anti-D Use in Rh+ patients. The Anti-D will coat the patient’s RBC, so that the IgG coated RBC compete with the IgG coated platelets for phagocytosis from the spleen, blocking splenic destruction of platelets. IVIG Splenectomy if refractory to treatment Case 3 Case 3 76 year old male with 80-90% stenosis of left main coronary artery, 70% stenosis of left anterior descending coronary artery Underwent Coronary Artery Bypass Graft (CABG) Case 3 Platelet counts: Pre-op: 169 x 1000/μL (150 – 400) Day of surgery: 110 POD #1: 104 POD #2: 74.7 POD #3: 92.2 POD #4: 81.5 POD #5: 89.8 POD #6: 52.3 POD #7: 11.3 POD #8: 8.86 Case 3 Patient received heparin prior to and during surgery, with no documentation of heparin received post-operatively. No clinical evidence of clotting. Case 3 Differential diagnosis: Heparin-induced thrombocytopenia (HIT) Other drug-induced thrombocytopenia ITP DIC TTP Case 3 Diagnosis: Heparin-induced thrombocytopenia ELISA test positive Case 3 Patient was switched to Argatroban, all heparin was discontinued Platelet count increased to 231 No thrombotic events HIT Occurs as a result of an antibody complex between heparin and platelet factor 4 IgG antibodies bind to the platelet Fc receptor and cause platelet activation, resulting in platelet activation as well as clearance from circulation. HIT HIT Diagnosis: Diagnosis rests primarily on clinical grounds • Laboratory tests not always locally available. • Lab tests may not be available in timely manner • Available tests are not completely sensitive or specific. HIT Clinical diagnosis (Four T’s): Thrombocytopenia: >50% fall in platelet count Timing: Days 5-10 after exposure to heparin, or <day 1 with recent heparin exposure (past 30 days) Thrombosis: Proven new thrombosis; skin necrosis; acute systemic reaction after IV heparin OTher causes of platelet fall excluded HIT Functional assay: Utilize the ability of the antibody to cause platelet activation as an endpoint. Require source of normal human platelets with variability See platelet activation at therapeutic concentration of heparin, but not at markedly therapeutic levels HIT Functional assays: Serotonin release assay. Most sensitive and specific of the functional assays • Incubate washed platelets with radiolabeled serotonin. Metabolically active platelets tae up serotonin and store it in their granules. • “Hot” platelets incubated with patient’s serum in the presence and absence of heparin at therapeutic and supratherapeutic levels. • Measure radioactivity in supernatant. Positive if: >20% release at therapeutic heparin level <20% release at supratherapeutic levels • 99% specificity, high sensitivity • Very few labs perform because of technical difficulty and use of radioactive substances. HIT Functional assays: ATP release via luminescence aggregometry • Closely resembles SRA as alternative approach • Able to detect ATP release of activated platelets Platelet aggregation studies: • Donor platelets incubated with patient’s serum and heparin. Measure donor platelets aggregation without heparin, with therapeutic levels of heparin, and with supratherapeutic heparin • Highly dependent on donor platelets Sensitivity 39-81% Specificity 82% HIT Immunological Assays: ELISA to detect the Heparin-PF4 antibody • Does not require normal platelets, technically easier to perform • High false positive rate, low specificity 50-60% patients undergoing open heart surgery will have a positive ELISA in the absence of clinical HIT Commercially available assay detects IgG, IgA, and IgM heparin-PF4 antibodies • Unlikely that IgM would cause clinical disease HIT Immunologic Assays: ELISA (cont’d): • Does have higher sensitivity than aggregation studies ELISA for HIT may initially be negative at time first clinically suspect HIT, but that a portion of those may then develop a positive ELISA if the test is repeated based on persisting clinical suspicion. May have false negative because HIT is due to an antigen other than PF4 HIT No laboratory test is 100% specific or sensitive for HIT Interpret results in light of the pretest probability. Should only be performed when there is a clinical indication of HIT HIT Treatment: Discontinue all heparin and low molecular weight heparin Use alternative anticoagulant (direct thrombin inhibitor): • Argatroban • Lepirudin The End