Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Middle East respiratory syndrome wikipedia , lookup
Chagas disease wikipedia , lookup
Sarcocystis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Gastroenteritis wikipedia , lookup
Hookworm infection wikipedia , lookup
Trichinosis wikipedia , lookup
Leptospirosis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Hepatitis C wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Plasmodium falciparum wikipedia , lookup
Schistosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Neonatal infection wikipedia , lookup
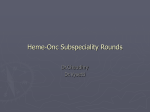
1151 Hemolysis and Infection: Categories and Mechanisms of Their Interrelationship Frank E. Berkowitz From the Department of Pediatrics, Emory University School of Medicine, Atlanta, Georgia Anemia is commonly recognized during the course of infections, especially chronic and acute infections in children [1, 2]. Possible mechanisms for this development of anemia include failure of iron utilization, bone-marrow suppression, and shortened duration of red blood cell (RBC) survival (hemolysis) . Hemolysis is a well-recognized feature of infections such as malaria, but it may also occur in a wide variety of other infections. Recognition of such hemolysis is important not only because it may require specific management but also because it may provide a clue to the cause of the infectious process. The association of hemolytic anemia with infection has been briefly reviewed by Beutler [3]. The present review will provide a clinically useful classification of different cause-andeffect associations of hemolytic and infectious processes and examine the mechanisms by which these associations occur. Case Reports Case I A 3-week-old boy was admitted to Baragwanath Hospital, Johannesburg, with a history of a recent onset of fever. He had been born by normal vaginal delivery at another hospital. He had received phototherapy and at 2 weeks of age had received an exchange transfusion for hyperbilirubinemia of unknown etiology. On admission he was a well-looking baby with mild fever and no other clinical findings. The hemoglobin concentration was 9.1 g/dl., and the total leukocyte count was 7.9 x 109/L, with 63% neutrophils, 5% monocytes, and Received 29 May 1990; revised 27 December 1990. Reprints and correspondence: Dr. Frank E. Berkowitz, Department of Pediatrics, Emory University School of Medicine, 69 Butler Street SE, Atlanta, Georgia 30303. Reviews of Infectious Diseases 1991;13:1151-62 © 1991 by The University of Chicago. All rights reserved. 0162-0886/91/1306-0041$02.00 32 % lymphocytes. The CSF was normal. He was treated for possible bacteremia with penicillin and gentamicin. On the third day he was pale and had splenomegaly. A blood smear showed a high concentration of Plasmodiumfalciparum. He was treated intravenously with quinine but developed hypoglycemia and shock. He received an exchange transfusion but died on the following day. Neither the mother nor the donors of the blood for the original exchange transfusion gave evidence of malaria. Case 2 An 8-year-old boy from Mozambique was admitted to Johannesburg Hospital with a 3-week history of a high intermittent fever, rigors, vague abdominal pain, and dark urine. He had been treated with chloroquine for presumed malaria but did not respond clinically. On examination he was an illappearing child with marked pallor, a temperature of 37.8°C (which later rose to 40°C), weight of 22.5 kg, a pulse rate of 134/minute, and a blood pressure of 90/36 mm Hg. He had mild jaundice but no cyanosis. The other important findings were a slight distension of the abdomen with a 4-cm tender hepatomegaly but no splenomegaly, bilateral axillary lymphadenopathy, and the child's withdrawn but conscious state and extreme weakness, with brisk deep tendon reflexes. The results oflaboratory investigations were as follows: hemoglobin concentration, 5.1gldL; mean corpuscular volume, 106 fl; mean corpuscular hemoglobin (MCH), 22.4 pglcell; MCH concentration, 31.8 g of Hb/dL of red blood cells (RBCs); total leukocyte count, 30.5 X lQ9/L, with 68% neutrophils, 22 % lymphocytes,S % monocytes, 3 % metamyelocytes, and 1% each of myelocytesand basophils; platelet count, 377 x 109/L; reticulocyte count, 23.2 %; total bilirubin, 6 ~mol/L, with a direct component of 1 ~mol/L; aspartate aminotransferase, 102 units/L; alanine aminotransferase, 76 units/L; and haptoglobin, 0.7 g/L (normal, 1.0-3.0 giL). The patient was given a blood transfusion. Blood, urine, and stool cultures were negative for pathogens, and the chest radiograph was normal. Blood smears for Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 Different cause-and-effect relationships between hemolytic and infectious processes are categorized in a clinically useful manner as follows: infections causing hemolysis by invasion of red blood cells (RBCs), by hemolysins, or by immune mechanisms; oxidative damage to RBCs during infections; hemolysis secondary to infection-induced pathologic processes; hemolytic effects of antimicrobial therapy; and predisposition of an individual to infection caused by an underlying hemolytic disorder or therapy for that disorder. The mechanisms of these interrelationships are discussed in detail. 1152 Berkowitz Infections Causing Hemolysis-No Underlying RBC Abnormality Infection of the RBe Malaria. Malaria is one of the most common human infections and probably the best known and most dramatic example of the association of hemolysis and infection. A diagnosis of malaria should always be considered in patients with hemolysis and a fever, as demonstrated by patient 1. Falciparum malaria is the most widespread and potentially harmful type of malaria and that in which anemia is most severe. Anemia in malaria is due to both hemolysis and defective erythropoiesis [4]. Hemolysis occurs mainly extravascularly but may occur intravascularly in severe cases. The mechanisms of hemolysis appear to be both structural and immune. The structural changes in the RBC include membrane damage and increased membrane rigidity [4]. A review of the sites on the RBe that potentially expose it to damage by different malarial parasites has been presented elsewhere [5]. That the degree of anemia often exceeds the degree of parasitemia and that anemia may persist or first appear after clearance of the parasitemia suggests that mechanisms other than structural changes in the RBC might also operate in producing hemolysis [6, 7]. Evidence suggests that autoimmune hemolysis affecting nonparasitized RBCs accounts for some of this anemia, but the involvement of an autoimmune response remains controversial [8-10]. The prevalence of hemolysis, as measured by decreased serum concentrations of haptoglobin, has been used as an indicator of the prevalence of malaria in a community [11]. Babesiosis. Babesiosis is primarily an infection of animals, but it occasionally affects human beings. The causative organisms, members of the genus Babesia, of which there are several species, are sporozoans that infect RBCs and that may be confused on microscopic examination with malarial parasites. Most cases of babesiosis in humans are caused by Babesia microti, which is transmitted to humans by ticks. Most Table 1. Categories of association of infection and hemolysis. I. Infection causing hemolysis-no underlying RBC abnormality A. Infection of the RBC: malaria; babesiosis; bartonellosis B. Hemolytic toxin: Clostridium perfringens C. Immune hemolysis 1. Autoantibodies to the RBC 2. Deposition of immune complexes on the RBC 3. Exposure of T antigens in the RBC membrane D. Congenital infections: unknown mechanism II. Infection precipitating hemolysis by oxidative stress in individuals with underlying RBC disorder: G6PD deficiency; unstable hemoglobins; paroxysmal nocturnal hemoglobinuria III. Infection-induced pathologic responses causing hemolysis A. Hemolytic uremic syndrome B. Cardiac hemolytic anemia C. Hypersplenism (?) IV. Hemolysis caused by anti-infective therapy A. Autoimmune B. Oxidant stress C. Toxic, e.g., ribavirin V. Underlying hemolytic disorder predisposing to infection A. Hyposplenism: sickle cell disease B. Ischemia: sickle cell disease C. Reticuloendothelial blockade (?) D. Hyperferremia (?) E. Defect in neutrophil killing: variants of G6PD deficiency VI. Predisposition to infection by therapy for hemolytic disorders A. Blood transfusion: transmission of infectious agents B. Immunosuppressive therapy C. Splenectomy D. Iron overload from repeated blood transfusions E. Deferoxamine therapy: predisposition to systemic yersiniosis, zygomycoses VII. Underlying hemolytic disorder, with aplastic crisis precipitated by infection with parvovirus B19 cases in the United States occur in the northeast, particularly on the islands off the Massachusetts coast [12]. The disease resembles malaria clinically, but it is usually self-limited, except in asplenic individuals, for whom it may be fatal. The mechanism of hemolysis in babesiosis is unclear. However, changes in the RBC membrane, such as protrusions, inclusions, and perforations, suggest that direct parasite-induced damage to the RBC occurs [13]. Hemophagocytosis in the bone marrow has also been described [14]. Bartonellosis (Oroyafever). Bartonellosis is caused by the gram-negative bacillus Bartonella bacilliformis. It is transmitted by the sandfly in the valleys of the Andes in Peru, Colombia, and Ecuador. The organism initially infects endothelial cells and subsequently becomes attached to the surface of RBCs. The acute phase of the illness is associated with a severe hemolytic anemia, whereas the chronic (eruptive) phase is characterized by verrucous skin lesions [15]. The hemolytic anemia lasts for about 10 days. The mechanical fragility of the RBCs increases, but the Coombs' test is negative. It has been suggested that the causative organism can be re- Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 plasmodia and microfilaria were negative. Agglutinating antibodies to the 0 antigen of Salmonella typhi were present at a titer of 1:3,200. A diagnosis of typhoid fever with severe hemolytic anemia was made, and the patient was treated with amoxicillin at a dosage of 1 g every 6 hours orally, to which he responded well. The patient's glucose-6-phosphate dehydrogenase (G6PD) activity was 72 % of the control value during the acute illness, and 25 % of the control value when measured 3 months later. He thus had G6PD deficiency and suffered from a hemolytic crisis precipitated by typhoid fever. These cases are dramatic examples of an infectious process causing hemolytic anemia. Different categories of association of hemolytic and infectious processes are summarized in table 1. RID 1991;13 (November-December) RID 1991;13 (November-December) Hemolysis and Infection Hemolytic Toxins Although many pathogenic bacteria produce hemolytic toxins (hemolysins) that may be virulence factors [17], the only bacterial hemolysin known to cause hemolysis in humans is the ex toxin of Clostridium perfringens. This toxin, when given iv to animals-but not when given im-causes massive intravascular hemolysis [18, 19]. The toxin reacts with an RBC surface lipoprotein complex, a reaction that results in the release oflysolecithin, a potent hemolysin. In humans, this hemolysinmay produce severeintravascular hemolysis [20]. Immune Hemolysis Due to Infection There are three basic mechanisms by which infections may result in hemolysis on an immune basis: antibodies to the RBCs are produced as a result of the infection (autoimmunity); antibody-antigen complexes specifically related to the infectious agent coat the RBC, which then acts as an "innocent bystander"; the infectious agent results in exposure of RBC antigens, which are normally hidden, to naturally occurring antibodies (polyagglutination). Autoimmune hemolytic anemia. Autoimmune hemolytic anemia is the result of the formation of antibodies directed to antigens on the RBC membrane [21]. Infections account for 1'\.18 % of cases of autoimmune hemolytic anemia overall [22] and for rv27 % of cases in children [23]. The possible immunologic bases for the production of these antibodies are discussed in other reviews [22, 24]. The three main types of RBC autoantibodies are the socalled warm antibodies and cold antibodies and the DonathLandsteiner antibodies [21]. Warm antibodies are usually of the IgO class and bind at 37°C to RBC protein antigens-usually those of the Rh sys- tem. Antibodies of subclasses Ig03 and IgOl may be bound to Fe receptors of phagocytic cells, resulting in phagocytosis of the RBC to which such antibodies are attached, a process that occurs primarily in the spleen. Cold antibodies are usually of the IgM class. They bind to RBCs at low temperatures and fix complement. At warm temperatures (body temperature) the antibody is eluted off the RBC. The complement remains fixed, however, and may form the terminal "attack" complex, causing intravascular hemolysis. Alternatively, the C3b component of complement may allow the RBC to become attached, via C3b receptors, to a phagocyte. Phagocytosis in this situation occurs mainly in the liver. Cold antibodies are generally directed at polysaccharides in the RBC, especially antigens of the Ii system. The i antigen is found on all human fetal and neonatal RBCs and is progressively replaced by the I antigen as the individual gets older [25]. Most infection-induced autoimmune hemolytic anemias are mediated by cold antibodies (i.e., they cause cold hemagglutinin disease [CHADD [22]. The infectious agents most commonly associated with CHAD are Mycoplasma pneumoniae (in which the antibody is directed at the I antigen) and EpsteinBarr virus (in which it is directed at the i antigen) [21]. CHAD has also been described following mumps, cytomegalovirus infection, Legionnaire's disease, and visceral leishmaniasis [26-28]. Donath-Landsteiner antibodies, which are IgO, cause paroxysmal cold hemoglobinuria (PCH). These antibodies become attached to the RBCs at low temperature and fix complement. When the RBCs are warmed, they are lysed intravascularly by the complement. The target RBC antigen is the P antigen. PCH is usually an acute illness, presenting during the convalescent stage of an infection with the sudden onset of pallor, hemoglobinuria, jaundice, and hepatosplenomegaly [22], and is usually self-limited. It has been reported following upper respiratory tract infections, chickenpox, infectious mononucleosis, mumps, measles, measles immunization, and M. pneumoniae infections [21, 22]. A more chronic form may complicate secondary syphilis [29]. Autoimmune hemolytic anemia (AIHA) has been reported following a wide variety of infections, including infection with human immunodeficiency virus (HN) [30, 31]. The type of antibody responsible for the disease is not always made clear in the reports. Immunizations have also been implicated in AIHA [23, 32]. In most of the reported cases, the role of the immunization as a cause of the hemolytic anemia was not well demonstrated. The diagnosis of AIHA depends on the demonstration of sensitization of the RBCs with antibody (i.e., coated) by showing that the RBCs are agglutinated by an antiglobulin preparation. This is the direct antiglobulin test (DAT) or direct Coombs' test. The antiglobulin preparation consists of a mixture of antibodies to IgO, IgM, and complement, or of antibody to one of them. To determine the antigen to which the Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 moved from the RBC surface by phagocytes without the destruction of the RBC itself [16]. Superinfection with non-typhoid salmonellae is a major cause of morbidity and mortality during the acute phase of bartonellosis and is discussed in the section on underlying hemolytic disorders that predispose to infection. In addition to infecting the RBC and causing hemolysis, malaria, babesiosis, and bartonellosis are usually transmitted in specific geographic locations and by specific arthropod vectors (malaria and babesiosis may also be transmitted by blood transfusion) and are diagnosed by visualization of the infecting organism on a Oiemsa-stained blood smear (bartonellosis may also be diagnosed by blood culture). Therefore, in individuals with evidence of hemolysis and infection, a history of travel, blood transfusion, iv drug abuse, and exposure to arthropods must be obtained and consideration must be given to examination of thick and thin blood smears under an oil-immersion lens. 1153 1154 Berkowitz Congenital Infections Chronic intrauterine infections, e.g., congenital syphilis, rubella, cytomegalovirus infection, and toxoplasmosis, are commonly associated with a hemolytic anemia, the mechanism of which is unknown [42-44]. Infection Precipitating Hemolysis by Oxidative Stress in Individuals with an Underlying RBe Disorder The normal RBC is frequently exposed to oxidant stresses that can result in oxidation of the RBC membrane and/or of hemoglobin. The balance between the severity of the oxidant stress and the power of the reducing mechanisms of the RBC will determine whether the RBC will suffer oxidative damage. If such damage occurs, the life span of the RBC will be reduced [45]. The RBC membrane may undergo lipid peroxidation and disulfide bonding, reactions that result in increased rigidity of the cell. Hemoglobin may be oxidized to methemoglobin and, via the intermediate compound hemichrome, to Heinz bodies, which are inclusions that bind to the RBC membrane, contributing to its increased rigidity [45]. The main reducing mechanisms of the RBC consist of four enzymes: glucose-6-phosphate dehydrogenase (G6PD), glutathione reductase, NADH diaphorase, and glutathione peroxidase (figure 1 [45]). Methemoglobin is reduced primarily by NADH diaphorase, which is not shown in the diagram. NADPH methemoglobin reductase, which is shown in the diagram, plays a role only in the presence of an artificial electron carrier such as methylene blue [46]. Deficiency of these enzymes is most commonly inherited, the most common and important deficiency being that of G6PD [45]. Certain inherited abnormalities of hemoglobin, e.g., sickle hemoglobin; hemoglobin Barts (HbH); and hemoglobins Zurich, Christchurch, Koln, and Volga, also render the RBC particularly susceptible to oxidative damage [47]. The main factors causing oxidative stress in RBCs are infections (discussed here) and drugs and toxins (discussed later). The role of infections as a cause of hemolysis via oxidative stress has been most thoroughly investigated in individuals with G6PD deficiency. The gene for the enzyme G6PD lies on the X-chromosome and is polymorphic. The genetic variants-more than 150are produced by one or more genetic mutations [48]. They have been categorized into five groups according to the activity of the enzyme. A few variant enzymes have a shortened life span, which results in progressive deficiency in enzyme activity with increasing age of the RBC. This deficiency renders the cell susceptible to oxidative damage and hemolysis. The enzyme with standard activity is G6PDB. The most common variants resulting in deficient activity are G6PDA-, which is common in blacks in sub-Saharan Africa and in the United States; G6PDMediterranean, in the Mediterranean Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 antibodies are directed, it is necessary to elute the antibodies off the RBC. Depositionofimmune complexes on the RBC. This form of immune hemolysis, in which the RBC acts as an "innocent bystander;' is one of the most common forms of hemolysis affecting children because of its frequent occurrence in systemic infections caused by Haemophilus infiuenzae type b. The high frequency of anemia in children with meningitis due to H. influenwe, as compared with meningitis due to other bacteria, was first noted by Schiavone and Rubbo in 1953 [33], and the association of such anemia with a longer duration of illness was recognized by Kaplan and Oski in 1980 [34]. In 1986 Shurin et al. confirmed these findings and showed that polyribose phosphate (PRP, the H. infiuenzae type b capsular antigen) and antibodies to PRP were present simultaneously in the sera of children with systemic infection with H. influenwe and anemia, as was evidence of recent intravascular hemolysis [35]. These workers showed in vitro that RBCs sensitized with PRP were lysed when they were incubated together with antibodies to PRP and complement, demonstrating that the hemolysis that occurs during H. influenwe type b infections is due to an immune-complex mechanism. PRP-sensitized RBCs bind antibody to PRP, after which complement is fixed, a sequence resulting in hemolysis [35]. Whether the RBC is truly an "innocent bystander" or exhibits specific PRP receptors is unclear. A similar mechanism is also thought to explain the anemia that occurs in African trypanosomiasis [36] and to playa role in the pathogenesis of anemia in malaria [8]. Polyagglutination. Polyagglutination occurs when Thomsen-Friedenreich (T) cryptoantigens within the RBC membrane are exposed to naturally occurring serum antibodies to T antigens. The T antigen is a precursor substance of the human MN blood group antigens. It is normally masked but may become unmasked by exposure of the RBC to neuraminidase, which removes sialic acid from surface glycoproteins. Most individuals >6 months old have circulating antibodies to T antigens. If the T antigen is unmasked, these antibodies, which are mainly of the IgM class, cause agglutination and subsequent phagocytosis of the RBCs [37]. This phenomenon of polyagglutination has been noted in young infants with bowel disorders, such as necrotizing enterocolitis, in whom neuraminidase produced by enteric bacteria is thought to cause exposure of the T antigen [38-40]. Such agglutination may be recognized only during attempts at cross-matching blood [41]. In young infants who lack antibodies to T antigens, exposure of the T antigen will not result in polyagglutination and hemolysis. However, transfusion of adult blood containing antibodies to T antigens may result in hemolysis [39, 40]. Lenz et al. found evidence of polyagglutination in 17 of 53 adults in a surgical intensive care unit. In 12 of these 17 patients, elevated serum levels of neuraminidase, presumably of microbial origin, could be demonstrated [37]. RID 1991;13 (November-December) RID 1991;13 (November-December) Hemolysis and Infection G6P NADP GSH 6PG N ADPH GSSG area; G6PDDebrousse, in North Africa; and G6PDCanton, in Southern Asia [49]. The role of infection in precipitating hemolysis in individuals with G6PD deficiency was first appreciated during the 1960s·[50, 51]. Pursuing the observation that transient anemia during acute bacterial infection occurred more commonly in American blacks (30%-40%), in whom G6PD deficiency is common, than among American whites (5%-10%), in whom this deficiency is rare, Mengel et al. prospectively studied the association of infection, anemia, and G6PD deficiency in 206 black patients [52]. Of 69 patients with anemia only, 14 (20%) had G6PD deficiency; of 47 with infection only, 14 (30 %) had this deficiency; and of 18 with both anemia and infection, 12 (67 %) had this deficiency. Mengel et al. concluded that the likelihood of G6PD deficiency in a patient with both infection and anemia is high [52]. More recently, Shannon et al. found that infection is the factor precipitating hemolysis in 10 of 14 black children with G6PD deficiency [53]. How does infection impose oxidative stress on the RBC? A large body of evidence suggests that the stress is accomplished by phagocytic cells, e.g., neutrophils that have been activated by the infection [54-59]. It is thought that superoxide produced by neutrophils causes oxidation of hemoglobin to methemoglobin and that H 20 z interacts with the methemoglobin to cause hemolysis. Other evidence indicates that proteolytic mechanisms account for some of the damage inflicted on the RBCs by activated neutrophils [59]. How are neutrophils brought into proximity with RBCs in order to exert their damaging effect? Evidence suggests that the cells are brought into contact by immune-complex bridges [60]. The RBC receptors for these complexes are thought to be their surface receptors for the activated complement components C3b and C4b [61, 62]. Infection-Induced Pathologic Responses Causing Hemolytic Anemia Three unrelated syndromes are included in the category of pathologic responses to infection that result in a shortened RBC survival time: hemolytic-uremic syndrome, cardiac hemolytic anemia, and hypersplenism. Hemolytic-Uremic Syndrome Hemolytic-uremic syndrome (HUS) consists of a group of disorders characterized by hemolytic anemia, thrombocytopenia, renal injury, CNS dysfunction, and thrombotic microangiopathy. Its clinical spectrum overlaps with that of thrombotic thrombocytopenic purpura [63, 64]. The syndrome exhibits different epidemiologic patterns, i.e., epidemic (typical) and endemic (atypical). Typical HUS affects primarily, although not exclusively, infants and young children. It is characterized clinically by a prodromal illness - usually gastroenteritis or an upper respiratory tract infection - followed by the acute onset of renal failure, hemolytic anemia, and thrombocytopenia. Pathologically it is characterized by thrombotic Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 Figure 1. Principal reactions involved in reduction of oxidized compounds in the red cell, which involves the enzymes glucose6-phosphate dehydrogenase (1); glutathione reductase (2); NADPH methemoglobin reductase Q); and glutathione peroxidase ~). G6P = glucose-6-phosphate; 6PG = 6-phosphogluconate; NADP = nicotinamide adenine dinucleotide phosphate; GSSG = glutathione (oxidized form); GSH = glutathione (reduced form); RSSR = compound with sulfhydryl groups (oxidized form); RSH = compound with sulfhydryl groups (reduced form); Hb Fe2+ = hemoglobin with ferrous iron; and HbFe 3+ = hemoglobin with ferric iron. Reprinted with permission from W. B. Saunders [45]. 1155 1156 Berkowitz Cardiac Hemolytic Anemia The association of hemolysis with disease of native heart valves was first recognized by Dameshek et al. in 1964 [67]. This type of hemolysis has been called macroangiopathic hemolysisand is thought to be caused by shear forces exerted on the RBC by extremely turbulent blood flow. The hemolysis occurs intravascularly and is characterized by hemoglobinuria, hemosiderinuria, a decreased plasma concentration of haptoglobin, and the finding of fragmented RBCs on blood smear. Although most cases occur in patients with prosthetic heart valves, it also occurs in patients with valvular rheumatic heart disease, particularly that affecting the aortic valve [68-70]. This type of hemolytic anemia may occur in patients with infective endocarditis but has been reported only rarely in patients with this infection who do not have prosthetic valves [68, 71-73]. Hypersplenism Hypersplenism is a syndrome consisting of splenomegaly, a decrease in one or more cellular elements of blood., a normal amount or hyperplasia of these elements in the bone marrow, and correction of the abnormality following splenectomy. Many underlying conditions may cause hypersplenism, including infections such as malaria, visceral leishmaniasis, schistosomiasis, tuberculosis, and brucellosis [74J. The anemia in hypersplenism is thought to be caused primarily by the sequestration ofRBCs in the spleen and expansion of the plasma volume. Shortened RBC survival and overt hemolysis are not prominent features of this condition. However, in several of the above-mentioned infections associated with marked splenomegaly, hemolytic anemia is thought to be immune-mediated. In these circumstances the splenomegaly may occur partially as a result of chronic hemolysis rather than as a cause of it [75]. Hemolysis Caused by Anti-Infective Therapy Hemolytic anemia accounts for rv10 % of the adverse hematologic effects of drugs. The precise role played by a specific drug in this hemolysis is not always clear, because the hemolysis might be caused by the disease being treated, by an underlying RBC abnormality, or by another drug. Although many different antimicrobial agents have been shown to cause hemolysis, only a few cases have been reported for several agents [76]. Drugs may cause hemolysis by immune or oxidative mechanisms. When the mechanism of hemolysis is unknown, the effect of the drug on the RBC is called toxic. Immune Drug-Induced Hemolytic Anemia There are three different immune mechanisms by which drugs may cause hemolysis: the immune-complex "innocent bystander" mechanism; the immune-complex drug-adsorption mechanism; and the autoimmune mechanism [77]. With both immune-complex mechanisms, the drug acts as a hapten. Since most drugs are small molecules (molecular weight, <500-1,000) and are non-protein, they are generally non-immunogenic by themselves. However, when the drugs are attached to a carrier protein such as an RBC membrane protein or a serum protein, they may become immunogenic. Immune-complex "innocent bystander"mechanism. In this circumstance, the prototype cause of which is quinidine, immune complexes consisting of the drug and antibodies to the drug become attached to the RBC, usually fixing complement and resulting in total lysis of the RBC. The direct Coombs' test is positive with anti-complement antiserum, and the indirect Coombs' test is positive only in the presence ofthe drug [77]. In some cases a specific RBC receptor antigen appears to be necessary for binding of the immune complex [78]. In a patient who has previously been sensitized to the drug, only a small amount of drug is necessary to cause hemolysis. Clinically, the hemolysis is acute, severe, and often intravascular. Drugs used in the treatment of infection that have been implicated in this type of immune hemolysis include acetaminophen, amoxicillin, cephalosporins, isoniazid, p-amino- Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 microangiopathy, which primarily affects the renal glomeruli. The blood smear shows features of microangiopathic hemolysis, i.e., fragmented RBCs, burr cells, helmet cells, and schistocytes [63]. Several microorganisms have been incriminated in the etiology of this syndrome. Those whose roles have been best demonstrated are Escherichia coli (verotoxin-producing strains), Shigella dysenteriae, and Streptococcus pneumoniae [63, 65]. The pathogenesis of HUS is not completely understood and may be different in different forms of the syndrome. Endothelial injury seems central to the pathogenesis [63]. The two main theories of pathogenesis are not mutually exclusive. According to the first theory, endothelial injury, which is caused by the inciting agent, e.g., verotoxin, is followed by platelet aggregation and the formation of microthrombi. The fibrin strands within the thrombi are thought to cause mechanical disruption of RBCs and platelets. According to the second theory, the inciting agent causes direct damage to endothelial cells, to RBCs, and to platelets. Other factors thought to be involved in the pathogenesis of HUS include membrane lipid peroxidation; changes in blood concentrations of coagulation factors, including an imbalance between thromboxane A 2 and prostacycline concentrations; and an increase in concentrations of von Willebrand factor multimers. The pathogenesis of HUS associated with shigella infections may involve endotoxin, while that associated with pneumococcal infections appears to be the unmasking of the T cryptantigen by neuraminidase [63, 66]. RID 1991;13 (November-December) RID 1991;13 (November-December) Hemolysis and Infection Oxidative Drug-Induced Hemolysis The balance between oxidative stresses exerted on the RBC and its reducing ability has been discussed earlier. The role of drugs in oxidative hemolytic anemia has been discussed in an excellent review by Gordon-Smith [45]. The best-known example of this type of hemolysis is that occurring in individuals with G6PD deficiency. Although hemolytic anemia caused by the antimalarial drug pamaquine was first recognized in 1926, it was only during the 1950s that its mechanism - oxidative hemolysis of G6PDdeficient red cells - was appreciated [82]. The clinical course of this disorder was demonstrated by a study in which primaquine was given to individuals with G6PDA- (the common deficient variant in African Americans). After 2 to 3 days they developed signs of acute hemolytic anemia. The hemolysis continued for about 1 week and then stopped, despite continued administration of the drug. Because the enzyme activity in the RBC decreases as the cell ages, hemolysis primarily affects the older cells. The younger cells, which have adequate enzyme activity, are not hemolyzed despite the presence of the drug. This has important implications for the diagnosis of this disorder [82]. When a diagnosis of G6PD deficiency is suspected on the basis of clinical illness and the hematologic findings of Heinz bodies and vacuolated RBCs (bite cells), it should be confirmed by the demonstration of reduced enzyme activity in the RBC. When this is done during or shortly after the hemolytic episode, the enzyme activity might appear to be normal because a high proportion of the RBCs will be young. The assay should therefore be repeated after a few weeks, a necessity well demonstrated with regard to patient 2 described above. Many drugs have been incriminated as causing hemolysis in G6PD-deficient individuals, but in several cases the causative role of the drug in the hemolytic episode has not been well substantiated. Furthermore, the likelihood of a drug's causing hemolysis is influenced by the dose of the drug and the variant of the deficient enzyme [82]. The following antimicrobial drugs have been shown to cause hemolytic anemia in G6PD-deficient individuals: nalidixic acid, niridazole, nitrofurantoin, pamaquine, primaquine, sulfacetamide, sulfamethoxazole, sulfanilamide, sulfapyridine, and thiazolsulfone [82]. The combination trimethoprimsulfamethoxazole has been found to be safe for use in individuals with the G6PDA- variant [83]. The following drugs that are used in treating infections and that have previously been considered to be contraindicated for individuals with G6PD deficiency should actually be considered relatively safe: acetaminophen, aspirin, chloramphenicol, chlorguanide, chloroquine, colchicine, diphenhydramine, isoniazid, probenecid, pyrimethamine, quinidine, quinine, sulfamerazine, sulfamethoxypyridazine, sulfazoxazole, and trimethoprim [82]. Dapsone causes oxidative stress in RBCs and may cause methemoglobinemia and hemolysis [45]. When used in the usual dosage, dapsone does not cause significant hemolysis in individuals with the G6PDA- variant but may do so in individuals with the G6PDMediterranean variant or with variants of G6PD deficiency associated with chronic nonspherocytic hemolytic anemia [45]. Other drugs that may cause methemoglobinemia and hemolysis include sulfasalazine, which is used in the treatment of inflammatory bowel disease, and phenazopyridine hydrochloride, which is frequently used as a urinary analgesic [45]. "Toxic" Drug-Induced Hemolysis The drug-induced hemolysis referred to as "toxic" is that caused by unknown mechanisms. The prime example of an antimicrobial drug that produces such hemolysis is the broadspectrum antiviral agent ribavirin, a nucleoside analogue. This agent is given by aerosol inhalation for treatment of severe infection with respiratory syncytial virus and intravenously or orally for treatment of Lassa fever. Ribavirin is concentrated within the RBC, producing a mild hemolytic anemia that is generally not of clinical significance [84, 85]. Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 salicylic acid, probenecid, quinidine, guanine, rifampin, streptomycin, and sulfonamides [77, 79]. Blackwater fever, a severe form of intravascular hemolysis formerly occurring with repeated use of quinine in malaria-endemic areas, possibly represents an example of this type of immune hemolysis. Immune-complex drug-adsorption mechanism. In this circumstance, which most commonly occurs with penicillin, the drug binds to the RBC membrane. If antibodies to the drug are formed, they become attached to the drug on the RBC membrane. These antibodies are of the IgG class and do not fix complement. Ifmany antibody molecules become attached, extravascular hemolysis ensues. Although penicillin can frequently be found to coat RBCs, hemolysis of this type occurs only when large doses of this drug are administered. With cephalosporins, however, hemolysis may occur with the usual doses. The direct Coombs' test is positive with antiserum to IgG, and the indirect Coombs' test is positive only if drugsensitized RBCs are used in the test [77]. Antimicrobial agents that have been shown to cause hemolysis by this mechanism include the penicillins, several cephalosporins, erythromycin, tetracycline, isoniazid, quinidine, and streptomycin [76, 77, 80, 81]. Cephalosporin-coated RBCs may bind to non-immunoglobulin serum proteins. If the reagents used in the Coombs' test contain antibodies to these proteins, the Coombs' test may be positive in the absence of a setting for immune-mediated hemolysis [77]. Drug-induced autoimmune hemolyticanemia. In this circumstance, the prototype cause of which is a-methyldopa, the drug induces the formation of antibodies to RBCs without itself playing a role in the hemolytic process [77]. 1157 1158 Berkowitz Underlying Hemolytic Disorders Predisposing to Infection The most common hemolytic disease predisposing to infection is sickle cell disease. This predisposition is due primarily to the hyposplenism that follows the development of microinfarctions of the spleen, but a defect in C3b fixation to bacterial surfaces also is involved [101]. Hyposplenism may be detected in children with sickle cell disease who are as young as 4 months old and is usually present by the age of 1 year. This defect in host defense predisposes these individuals to infections - especially bacteremia - with encapsulated bacteria, particularly S. pneumoniae and H. irfiuenzae [87]. In Saudi Arabia and in tropical Africa.ienteric bacilli, e.g., E. coli and salmonellae, are also common causes of bacteremia in such individuals [102, 103]. In tropical Africa the most common infectious cause of death in individuals with sickle cell disease is malaria. Although individuals with sickle cell trait (heterozygous) are provided some protection against infection with P. falciparum, hyposplenic homozygotic individuals are particularly susceptible to severe infections with this parasite [l 02] . Persons with sickle cell disease are also particularly susceptible to osteomyelitis caused by non-typhoid salmonellae. Adeyokunnu and Hendrickse, in their study of 63 Nigerian children with salmonella osteomyelitis, found that 57 had sickle cell disease [104]. They postulated that the following sequence of events produces this infection. (1) Poor sanitation results in frequent gastrointestinal infections with salmonellae. (2) Bowel ischemia, which results from vasoocclusive episodes, facilitates hematogenous spread of these organisms. (3) The host defenses against salmonellae might be further compromised by hepatic dysfunction and hemolysis itself (see above). (4) Bone infarctions predispose to osteomyelitis and persistence of the organism in the affected area [104]. Another hemolytic disease in which there appears to be a specific predisposition to infection is G6PD deficiency. The evidence for this is both clinical and epidemiologic. G6PD deficiency primarily affects the RBC, resulting in hemolysis. However, the enzyme is also necessary for the production of the oxidative metabolites, e.g., H 20 2 , necessary for bacterial killing by phagocytes. G6PD activity of leukocytes is generally normal in individuals with G6PD deficiency in RBCs, but with rare variants of the enzyme deficiency, the leukocyte is affected. Individuals with these variants have presented with severe or recurrent infections, which often resemble those seen in patients with chronic granulomatous disease [105-107]. G6PD deficiency also appears to predispose to a particularly severe clinical course in patients with rickettsial infections [108, 109]. The epidemiologic evidence suggesting that G6PD deficiency predisposes to infection is provided by studies showing a higher prevalence of G6PD deficiency in infected than in noninfected individuals or a higher prevalence of infection in G6PD-deficient than in otherwise normal individuals. In 1975 Lampe et al. showed a higher prevalence of G6PD deficiency in children with typhoid fever, pneumococcal in- Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 It has been known for many years that certain conditions in which hemolysis occurs predispose to bacterial infections, e.g., bartonellosis to systemic salmonellosis and sickle cell disease to pneumococcal bacteremia [86, 87]. Although the specific reasons why different underlying hemolytic diseases predispose to infection may vary (see below), two possible mechanisms are responsible: reticuloendothelial blockade and increased availability of hemoglobin or iron for microbial growth. Experimental work in mice has shown that infusion of sensitized RBCs results in an increase in the fatality rate for Salmonella typhimurium infection [88], and infusion ofRBC stroma results in a decrease in the clearance function mediated by the hepatic macrophage complement receptor and an increase in the fatality rate for pneumococcal infection [89]. In vitro studies have shown that macrophages exposed to sensitized RBCs demonstrate decreased rates of bacterial killing [88-91]. This work suggests that ingestion of RBCs by the reticuloendothelial system, which is exaggerated in hemolytic states, may interfere with other clearance functions of the reticuloendothelial system, such as the removal of bacteria from the bloodstream. However, no decrease in reticuloendothelial clearance activity could be shown in studies of humans with thalassemia [92, 93]. The role of iron in host defenses and microbial growth has been reviewed by Bullen [94] and Finkelstein et al. [95]. They reviewed several reports in which iron therapy given for iron deficiency resulted in an increased incidence of severe infections, particularly those caused by enteric bacilli [94, 95]. Bullen demonstrated that blood facilitates the development of an infection in an enclosed space, e.g., the peritoneal cavity, by providing iron for microbial growth [94]. It is not clear if hemolytic conditions predispose to infections by providing iron to microorganisms. However, repeated blood transfusions resulting in iron overload, together with the use of deferoxamine, an iron chelator, undoubtedly predispose to severe infections. This effect of iron chelators has been observed in experimental animals with S. typhimurium infection and in humans with thalassemia with Yersinia enterocolitica infection [96, 97]. Yo' enterocolitica differs from many other bacteria in that it does not elaborate siderophores. When these organisms are present together with other bacteria, e.g., in the colon, they can assimilate iron by utilizing the siderophores produced by the other bacteria. In individuals with iron overload who are being treated with deferoxamine (a siderophore derived from Streptomyces pilosis) Y. enterocolitica present in a nonpermissive site, e.g., the bloodstream, can use deferoxamine as its siderophore and thus can multiply at such a site [98]. Deferoxamine also appears to predispose patients who are receiving it as therapy for iron or aluminum overload to infections with Zygomycetes [99, 100]. RID 1991;13 (November-December) RID 1991;13 (November-December) Hemolysis and Infection fection, and tuberculosis than in uninfected children [110]. In a study of 33,943 neonates in Saudi Arabia, Abu-Osba et al. showed that the incidence of bacteremia in infants with G6PD deficiency was significantly higher than that in otherwise normal infants. This increase was particularly significant for bacteremia caused by catalase-positive organisms (Le., those organisms capable of destroying leukocyte H2(h) [111]. Predisposition to Infection by Therapy for Hemolytic Disorders Blood Transfusion Blood transfusion is the primary supportive measure in the treatment of anemia, and transmission of infection is a major potential complication of this form of therapy. Although many different infectious agents can be transmitted by blood transfusion, the most important are the viral agentscausing hepatitis (non-A, non-B hepatitis and hepatitis B) and cytomegalovirus and HIV [112]. In malarial endemic areas, malaria is also an important transfusion-transmitted disease [112, 113] as is infection with Trypanosoma cruzi in areas where this parasite is endemic [112]. Infectious agents that may be transmitted by blood transfusion are listed in table 2 [114]. Many different bacteria have been reported to cause transfusion-acquired infections as a result of contamination of the blood after its collection from the donor [114]. Immunosuppression Corticosteroids are used for immunosuppression primarily for the treatment of autoimmune hemolytic anemias. If used in high doses for prolonged periods they predispose the patient to the infectious complications of chronic immunosuppression. Splenectomy Splenectomy is frequently performed in patients with hereditary hemolytic anemias such as hereditary spherocytosis and thalassemia major. Splenectomy renders the patient particularly susceptible to fulminating bacteremia with encapsulated organisms, in particular S. pneumoniae, H. irifluenzae type b, and Neisseria meningitidis [115]. Precipitation of an Aplastic Crisis by Parvovirus B19 in Individuals with Underlying Hemolytic Disorder Parvovirus B19 infects erythroid progenitor cells in the bone marrow, resulting in a transient decrease in the production ofRBCs. In normal individuals a transient decrease in hemoglobin concentration can be demonstrated, but usually this has little clinical consequence. However, in individuals with a chronic hemolytic anemia, whose RBCs have a shortened life and erythropoiesis is accelerated, this infection may result in the development of severe anemia, called an aplastic crisis. This infection has been reviewed elsewhere [116, 117]. Conclusion The wide variety of clinical situations in which hemolytic and infectious processes may be associated are described and categorized in a manner useful to the clinician. When a patient is suspected of having an infectious illness as well as a hemolytic process, it is essential to obtain a detailed history and to perform a thorough physical examination. Each pathologic process may necessitate the performance of several laboratory investigationsfor elucidation, e.g., cultures of different body fluids and various hematologic tests. However, attention to the following specific historical and laboratory information is of particular importance: (1) family or personal history, i.e., consanguinity, genetic diseases, gallstones, dark urine, chronic leg ulcers, recurrent episodes of anemia (especially after drug ingestion), and anemia unresponsive to hematinics [21, 118]; (2) epidemiologic history, i.e., geographic and travel history, blood transfusions, recreational activities, and other possible exposures to infectious agents; and (3) blood smear, which should include the examination of not only thin smears for RBC morphology, but also thick and thin smears for parasites. Table 2. Infectious agents transmitted in blood. Group Specific agents Viruses Hepatitis B, hepatitis A, hepatitis non-A non-B, cytomegalovirus; HIV; Epstein-Barr virus; HTLV-I Rickettsia prowazeki Treponema pallidum, Brucella, Yersinia enterocolitica; others associated with contamination of blood after its collection Plasmodium species; Trypanosoma cruzi; Trypanosoma brucei; Babesia species; Toxoplasma gondii Filaria Rickettsiae Bacteria Protozoa Nematodes NOTE. HTLV-I = human T cell Iymphotrophic virus I. References 1. Buchanan GR. The mild anemia of acute infection. Pediatr Infect Dis 1985;4 :225-8 2. Abshire TC, Reeves JD. Anemia of acute inflammation in children. J Pediatr 1983;103:868-71 3. Beutler E. Hemolytic anemia due to infections with microorganisms. In: Williams WJ, Beutler E, Erslev Al, Lichtman MA, eds. Hematology. 4th ed. New York: McGraw-Hill Book Co, 1990:~63-5 4. Weatherall DJ, Abdalla S. The anaemia of Plasmodium falciparum malaria. Br Med Bull 1982;38:147-51 5. Brown KN, Berzins K, Jarra W, Schetters T. Immune responses to Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 Although the variety of inherited and acquired hemolytic disorders is wide, presently relatively fewmodalities are available for treating these disorders. Several of these modalities predispose to infections, some of which have already been mentioned. 1159 1160 Berkowitz toimmune hemolytic anemia and human immunodeficiency virus (HIV) infection. Ann Intern Med 1988;109:249-50 31. Rapoport AP, Rowe JM, McMican A. Life-threatening autoimmune hemolytic anemia in a patient with the acquired immune deficiency syndrome. Transfusion 1988;28:190-1 32. Haneberg B, Matre R, Winsnes R, Dalen A, Vogt H, Finne PH. Acute hemolytic anemia related to diphtheria-pertussis-tetanus vaccination. Acta Paediatr Scand 1978;67:345-50 33. SchiavoneDJ, Rubbo SD. Anaemia associated with Haemophilus itifluenwe meningitis. Lancet 1953;2:696-8 34. Kaplan KM, Oski FA. Anemia with Haemophilus injiuenwe meningitis. Pediatrics 1980;65:1101-4 35. Shurin SB, Anderson P, Zollinger J, Rathbun RK. Pathophysiology of hemolysis in infections with Hemophilus injiuenwe type b. J Clin Invest 1986;77:1340-8 36. Vickerman K, Barry JD. African trypanosomiasis. In: Cohen S, Warren KS, eds. Immunology of parasitic infections. Oxford: Blackwell Scientific Publications, 1982:204-60 37. Lenz G, Goes D, Baron D, Sugg D, Heller W. Red blood cell T-activation and hemolysis in surgical intensive care patients with severe infections. Blut 1987;54:89-96 38. Obeid D, Bird GWG, Wingham J. Prolonged erythrocyte T-polyagglutination in two children with bowel disorders. J Clin Pathol 1977;30:953-5 39. Seges RA, Kenny A, Bird GWG, Wingham J, Baals H, Stauffer DG. Pediatric surgical patients with severe anaerobic infection: report of 16 T-antigen positive cases and possible hazards of blood transfusion. J Pediatr Surg 1981;16:905-10 40. Williams RA, Brown EF, Hurst D, Franklin LC. Transfusion of infants with activation of erythrocyte T antigen. J Pediatr 1989;115:949-53 41. Bird T, Stephenson J. Acute haemolytic anaemia associated with polyagglutinability of red cells. J Clin Pathol 1973;26:868-70 42. Lukens IN. Neonatal haematological abnormalities associated with maternal disease. Clin Haematol 1978;7:155-73 43. Whitaker JA, Sartain P, Shaheedy M. Hematological aspects of congenital syphilis. J Pediatr 1965;66:629-36 44. Ingall 0, Musher D. Syphilis. In: Remington JS, Klein JO, eds. Infectious diseases of the fetus and newborn infant. Philadelphia: W. B. Saunders, 1983:344-5, 347-8 45. Gordon-Smith EC. Drug-induced oxidative haemolysis. Clinics in Haematology 1980;9:557-86 46. Beutler E. Energy metabolism and maintenance of erythrocytes. In: Williams WI, Beutler E, Erslev AJ, Lichtman MA, eds. Hematology. 4th ed. New York: McGraw-Hill, 1990:362 47. Dacie J. The haemolytic anaemias. Vol 2. 3rd ed. Edinburgh: Churchill Livingstone, 1989:342 48. Beutler E. International cooperation in the study of glucose 6-phosphate dehydrogenase. Newsletter. Barcelona: International Society of Haematology. European and African Division, 1990;1:4-8 49. Piomelli S. G6PD deficiency and related disorders of the pentose pathway.In: Nathan DG, Oski FA, eds. Hematology of infancy and childhood. 3rd ed. Philadelphia: W. B. Saunders, 1987:583-612 50. Burka ER, Weaver Z ill, Marks PA. Clinical spectrum of hemolytic anemia associated with glucose-6-phosphate dehydrogenase deficiency. Ann Intern Med 1966;64:817-25 51. Salen G, Goldstein F, Haurani F, Wirts CWo Acute hemolytic anemia complicating viral hepatitis in patients with glucose-6-phosphate dehydrogenase deficiency. Ann Intern Med 1966;65:1210-20 52. Mengel CE, Metz E, Yancey WS. Anemia during acute infections. Role of glucose-6-phosphate dehydrogenase deficiency in Negroes. Arch Intern Med 1967;119:287-90 53. Shannon K, Buchanan GR. Severe hemolytic anemia in black children with glucose-6-phosphate dehydrogenase deficiency. Pediatrics 1982; 70:364-9 Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 erythrocytic malaria. Clinics in Immunology and Allergy 1986; 6:227-49 6. Pasvol G. The anaemia of malaria [editorial]. Q J Med 1986;58:217-9 7. Looareesuwan S, Merry AH, Phillips RE, Pleehachinda R, Wattanagoon Y, Ho M, Charoenlarp P, Warrell DA, Weatherall OJ. Reduced erythrocyte survival following clearance of malarial parasitaemia in Thai patients. Br J Haemotol 1987;67:473-8 8. Woodruff AW, Ansdell VE, Pettitt LE. Cause of anaemia in malaria. Lancet 1979;1:1055-7 9. Facer CA. Direct antiglobulin reactions in Gambian children with P. jalciparum malaria. III. Expression of IgG subclass determinants and genetic markers and association with anaemia. Clin Exp Immunol 1980;41:81-90 10. Abdalla S, Weatherall DJ. The direct antiglobulin test in P. jalciparum malaria. Br J Haematol 1982;51:415-25 11. Trope JF, Fribourg-Blanc A. Ahaptoglobinemia in African populations and its relation to malaria endemicity. Am J EpidemioI1988;127: 1282-8 12. Krause PJ. Babesiosis. In: Feigin RD, Cherry JD, eds. Textbook of pediatric infectious diseases. 2nd ed. Philadelphia: W. B. Saunders, 1987:2019-24 13. Sun T, Tenenbaum MJ, Greenspan J, Teichberg S, Wang R-T, Degnan T, Kaplan MH. Morphologic and clinical observations in human infection with Babesia microti. J Infect Dis 1983;148:239-48 14. Auerbach M, Haubenstock A, Solomon G. Systemic babesiosis: another cause of the hemophagocytic syndrome. Am J Med 1983; 80:301-3 15. Stechenberg BW. Bartonellosis. In: Feigin RD, Cherry JD, eds. Textbook of pediatric infectious diseases. 2nd ed. Philadelphia, W. B. Saunders, 1987:1096-8 16. Reynafarje C, Ramos J. The hemolytic anemia of human bartonellosis. Blood 1961;17:562-78 17. Arbuthnott JP. Bacterial cytolysins (membrane-damaging toxins). In: Cohen P, van Heyningen S, eds. Molecular action of toxins and viruses. Molecular aspects of cellular regulation. Vol 2. Amsterdam: Elsevier Biomedical Press, 1982:107-29 18. McDanel JL. Clostridium perfringens toxins (type A, B, C, D, E). Pharmacol Ther 1980;10:617-55 19. Smith LDS. Virulence factors of Clostridium perfringens. Rev Infect Dis 1979;1:254-60 20. Terebelo HR, McCue RL, Lenneville MS. Implication of plasma free hemoglobin in massive clostridial hemolysis. JAMA 1982;248: 2028-9 21. Dacie J. The haemolytic anaemias. Vol 1. 3rd ed. Edinburgh: Churchill Livingstone, 1985:4 22. Sokol RJ, Hewitt S. Autoimmune hemolysis: a critical review. Crit Rev Oncol Hematol 1985;4:125-54 23. Zupanska B, ~awkowicz W, G6rska B, Kozlowska J, Ochocka M, Rokicka-Milewska R, Derulska 0, Ciepielewska D. Autoimmune haemolytic anaemia in children. Br J Haematol 1976;34:511-20 24. Gibson J. Autoimmune hemolytic anemia: current concepts. Aust NZ J Med 1988;18:625-37 25. Petz LD, Garratty G. Acquired immune hemolytic anemias. New York: Churchill Livingstone, 1980:26-63 26. Warren RW, Collins ML. Immune hemolytic anemia in children. Crit Rev Oncol Hematol 1988;8:65-73 27. King JW, May JS. Cold agglutinin disease in a patient with Legionnaires' disease. Arch Intern Med 1980;10:1537-9 28. Kokkini G, Vrionis G, Liosis G, Papaefstathiou J. Cold agglutinin syndrome and haemophagocytosis in systemic leishmaniasis. Scand J Haematol 1984;32:441-5 29. Lascari AD. Haematologic manifestations of childhood diseases. New York: Thieme-Stratton, 1984:3, 33-4 30. Puppo F, Torresin A, Lotti G, Balleari E, Orlando G, Indiveri F. Au- RID 1991;13 (November-December) RID 1991;13 (November-December) Hemolysis and Infection 76. de Gruchy GC. Haemolytic anaemia. In: Drug-induced blood disorders. Oxford: Blackwell Scientific Publications, 1975:156-82 77. Petz LD, Branch DR. Drug-induced immune hemolytic anemia. In: Chaplin H Jr, ed. Immune hemolytic anemias. New York: Churchill Livingstone, 1985:47-94 78. Duran-Suarez JR, Martin-Vega C, Argelagues E, Massuet L, Ribera A, Triginer J. Red cell I antigen as immune complex receptor in drug-induced hemolytic anemias. Vox Sang 1981;41:313-5 79. Salama A, Gottsche B, SchleifferT, Mueller-Eckhardt C. 'Immune complex' mediated intravascular hemolysis due to IgM cephalosporindependent antibody. Transfusion 1987;27:460-3 80. Gmur J, Walti M, Neftel KA. Amoxicillin-induced immune hemolysis. Acta Haematol 1985;74:230-3 81. Branch DR, Berkowitz LR, Becker RL, Robinson J, Martin M, Gallagher MT, Petz LD. Extravascular hemolysis followingthe administration of cefamandole. Am J Hematol 1985;18:213-9 82. Beutler E. Glucose-6-phosphate dehydrogenase deficiency. In: Stanbury JB, Wyngaarden JB, Fredrickson DS, Goldstein JL, Brown MS, eds. The metabolic basis of inherited diseases. 5th ed. New York: McGraw-Hill Book Co, 1983:1629-53 83. Markowitz N, Saravolatz LD. Use of trimethoprim-sulfamethoxazole in a glucose-6-phosphate dehydrogenase-deficient population. Rev Infect Dis 1987;9(Suppl 2):S218-5 84. Gilbert BE, Knight V. Biochemistryand clinical applicationsof ribavirin. Antimicrob Agents Chemother 1986;30:201-5 85. Canonico PG, Kastello MD, Spears CT, Brown JR, Jackson EA, Jenkens DE. Effects of ribavirin on red blood cells. Toxicol Appl Pharmacol 1984;74:155-62 86. Cuadra Me. Salmonellosis complication in human bartonellosis. Tex Rep BioI Med 1956;14:97-113 87. Barrett-Connor E. Bacterial infection and sickle cell anemia: an analysis of 250 infections in 166 patients and a review of the literature. Medicine (Baltimore) 1971;50:97-112 88. Kaye D, Gill FA, Hook EW. Factors influencing host resistance to salmonella infections: the effects of hemolysis and erythrophagocytosis. Am J Med Sci 1967;254:205-15 89. Grover GJ, Loegering DJ. Effect of red blood cell stroma on the reticuloendothelial system clearance and killing of Streptococcus pneumoniae. Cire Shock 1984;14:39-47 90. Loegering DJ, Blumenstock FA. Depressing hepatic macrophage complement receptor function causes increased susceptibility to endotoxemia and infection. InfectImmun 1985;47:659-64 91. Hand WL, King-Thompson NL. Effect of erythrocyte ingestion on macrophage antibacterial function. Infect Immun 1983;40:917-23 92. Hicsonmez G, Dalat E, Erbengi G. Reticuloendothelial phagocyticfunction in children with B-thalassemia major. Acta Haematol 1979; 61:283-7 93. Dimitriou P, Giamouris J,Nicolaidou P, Antipas SE, Fretzayas A, Messaropoulos T, Karpathios T. RES phagocytosis in children with homozygous l3-thalassemia in relation to blood transfusion. Scand J Haematol 1986;37:417-20 94. Bullen JJ. The significance of iron in infection. Rev Infect Dis 1981;3:1127-38 95. Finkelstein RA, Sciortino CV, McIntosh MA. Role of iron in microbehost interactions. Rev Infect Dis 1983;5(Suppl 4):S759-77 96. Jones RL, Peterson CM, Grady RW, Kumbaraci T, Cerami A. Effects of iron chelators and iron overload on Salmonella infection. Nature 1977;267:63-5 97. Robins-BrowneRM, RabsonAR, KoornhofHJ. Generalized infection with Yersinia enterocolitica and the role of iron. Contrib Microbiol Immunol 1979;5:277-82 98. Robins-Browne RM, Prpic JK. Effects of iron and desferrioxamine on infections with Yersinia enterocolitica. Infect Immun 1985;47:774-9 99. Sane A, Manzi S, Perfect J, Herzberg AL, Moore JO. Deferoxamine Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 54. Baehner RL, Nathan DG, Castle WB. Oxidant injury of caucasian glucose-6-phosphate dehydrogenase-deficient red blood cells by phagocytosing leukocytes during infection. J Clin Invest 1971; 50:2466-73 55. Weiss SJ. The role of superoxide in the destruction of erythrocyte targets by human neutrophils. J Biol Chern 1980;255:9912-7 56 Winterboum CC, Williamson D, Vissers MCM, Carrell RW. Unstable haemoglobin haemolytic crises: contributions of pyrexia and neutrophil oxidants. Br J Haematol 1981;49:111-6 57. Weiss SJ. Neutrophil-mediated methemoglobin formation in the erythrocyte: the role of superoxide and hydrogen peroxide. J Biol Chern 1982;257:2947-53 58. Claster S, Chiu DT-Y, Quintanilha A, Lubin B. Neutrophils mediate lipid peroxidation in human red cells. Blood 1984;64:1079-84 59. Claster S, Quintanilha A, Schott MA, Chiu D, Lubin B. Neutrophilinduced K + leak in human red cells: a potential mechanism for infection-mediated hemolysis. J Lab Clin Med 1987;109:201-10 60. Kasper ML, Miller WJ, Jacob HS. G6PD-deficiency infectious haemolysis: a complement-dependent innocent bystander phenomenon. Br J Haematol 1986;63:85-91 61. Siegel I, Liu TL, Gleicher N. The red-cell immune system. Lancet 1981;2:556-9 62. Comacoff JB, Hebert LA, Smead WL, VanAman ME, Birmingham DJ, Waxman FJ. Primate erythrocyte-immune complex-clearing mechanism. J Clin Invest 1983;71:236-47 63. Kaplan BS, Proesmans W. The hemolytic uremic syndrome of childhood and its variants. Semin Hematol 1987;24:148-60 64. Neild G. The haemolytic uraemic syndrome: a review. Q J Med 1987;63:367-76 65. Cleary ro. Cytotoxin-producing Escherichia coli and the hemolytic uremic syndrome. Pediatr Clin North Am 1988;35:485-501 66. Novak RW, Martin CR. Hemolytic-uremic syndromeand T-eryptantigen exposure by neuraminidase-producing pneumococci: an emerging problem? Pediatr Pathol 1983;1:409-13 67. Dameshek W, Roth SI, Jacobsen BM, DeSanctis RW, Castleman B, Carter JR, vanHeeckeren DW, Tomchik FS, Stanbury JB, Sandler AI, Urrutia GM. Case records of the Massachusetts General Hospital: weekly clinicopathological exercises: Case 52-1964. N Engl J Med 1964;271:898-905 68. Forshaw J, Harwood L. Redblood cell abnormalities in cardiac valvular disease. J Clin Pathol 1967;20:848-53 69. Krishnaswami S, Cherian G, John S. Red cell hemolysis in rheumatic valvular disease and following prosthetic and heterograft valve replacement surgery: a study of 40 cases and review of literature. Indian J Med Res 1975;63:130-50 70. Dupont B, Wennevold A. Mechanical hemolytic anemia in unoperated aortic valve disease. Acta Med Scand 1968;1984:353-7 71. Naidoo DP, Seedat MA, Vythilingum S. Isolated endocarditis of the pulmonary valve with fragmentation haemolysis. Br Heart J 1988; 60:527-9 72. Nishiura T, Miyazaki Y, Oritani K, TominagaN, TomiyamaY, Katagiris S, Kanayama Y, YonezawaT, Tarui S, YamadaT, Sakurai M, Kume H, Okudaira M. Aspergillus vegetative endocarditis complicated with schizocytic hemolytic anemia in a patient with acute lymphocytic leukemia. Acta HaematoI1986;76:60-2 73. Berkowitz FE, Dansky R. Infective endocarditis in black South African children: a report of 10 cases with some unusual features. Pediatr Infect Dis 1989;8:787-91 74. Sills RH. Hypersplenism. In: Pochedly C, Sills RH, Schwartz AD, eds. Disorders of the spleen: pathophysiology and management. New York: Marcel-Dekker, 1989:167-86 75. Woodruff AW. Mechanisms involved in anaemia associated with infection and splenomegaly in the tropics. Trans R Soc Trop Med Hyg 1973;67:313-28 1161 1162 Berkowitz trophil dysfunction and Chromobacterium violaceum sepsis. J Pediatr 1987;111:852-4 108. Whelton A, Donadio JV, Elisberg BL. Acute renal failure complicating rickettsial infections in glucose-6-phosphate dehydrogenasedeficient individuals. Ann Intern Med 1968;69:323-8 109. Piras MA, Calia G, Saba F, Gakis C, Andreoni G. Glucose-6-phosphate dehydrogenasedeficiency in male patients with Mediterranean spotted fever in Sardinia [letter]. J Infect Dis 1983;147:607-8 110. Lampe RM, Kirdpon S, Mansuwan P, Benenson MW. Glucose-6phosphate dehydrogenase deficiency in Thai children with typhoid fever. J Pediatr 1975;87:576-8 111. Abu-Osba YK, Mallouh AA, Hann RW. Incidence and cause of sepsis in glucose-6-phosphate dehydrogenase-deficient newborn infants. J Pediatr 1989;114:748-52 112. Seidl S, Kuhn! P. Transmission of diseases by blood transfusion. World J Surg 1987;11:30-5 113. Bove JR. Transfusion-transmitted diseases: current problems and challenges. Prog Hematol 1986;123-47 114. Tabor E, Rook AH, Quinnan GV Jr, Kark JA. Infectious complications of blood transfusions. New York: Academic Press, 1982:1-165 115. Sills RH. Splenic function: physiology and splenic hypofunction. Crit Rev Oncol Hematol 1987;7:1-36 116. Anderson U. Role of paravovirus B19 in human disease. Pediatr Infect Dis 1987;6:711-8 117. Ware R. Human parvovirus infection. J Pediatr 1989;114:343-8 118. LanzkowskyP. Hemolytic anemia. In: Pediatric hematology- oncology. A treatise for the clinician. New York: McGraw-Hill Book Co, 1980:148-58 Downloaded from http://cid.oxfordjournals.org/ at Penn State University (Paterno Lib) on September 12, 2016 treatment as a risk factor for zygomycete infection [letter]. J Infect Dis 1989;159:151-2 100. Rex JH, Ginsberg AM, Fries LF, Pass HI, Kwon-Chung KJ. Cunninghamella bertholletiae infection associated with deferoxamine therapy. Rev Infect Dis 1988;10:1187-94 101. Wagner GM, Vichinsky EP, Lande WM, Pennathur-Das R. Sickling syndromes and unstable hemoglobin disease. In: Mentzer WC, Wagner OM, eds. The hereditary hemolytic anemias. New York: Churchill Livingstone, 1989:145-221 102. Onwubalili JK. Sickle cell disease and infection. J Infect 1983;7:2-20 103. Mallouh AA, Salamah MM. Patterns of bacterial infections in homozygous sickle cell disease: a report from Saudi Arabia. Am J Dis Child 1985;139:820-2 104. Adeyokunnu AA, Hendrickse RG. Salmonella osteomyelitis in childhood: a report of 63 cases seen in Nigerian children of whom 57 had sickle cell anaemia. Arch Dis Child 1980;55:175-84 105. Cooper MR, DeChateletLR, McCall CE, LaViaMF, Spurr CL, Baehner RL. Complete deficiency of leukocyte glucose-S-phosphate dehydrogenase with defective bactericidal activity. J Clin Invest 1972;51:769-78 106. Vives Corrons JL, Feliu E, Pujades MA, Cardellach F, Rozman C, Carreras A, Jou JM, Vallespi MT, Zuazu FJ. Severe glucose-6phosphate dehydrogenase(G6PD) deficiencyassociated with chronic hemolytic anemia, granulocyte dysfunction, and increased susceptibility to infections: description of a new molecular variant (G6PD Barcelona). Blood 1982;59:428-34 107. Mamlok R, Mamlok V, Mills GC, Daeschner CW ill, Schmalstieg FC, Anderson DC. Glucose-6-phosphate dehydrogenase deficiency, neu- RID 1991;13 (November-December)