Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
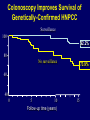
Genetics 202: Clinical Cancer Genetics James Ford, M.D., Associate Professor of Medicine (Oncology), Pediatrics (Medical Genetics) and Genetics Director, Stanford Program for Clinical Cancer Genetics and Genomics Nicki Chun, M.S. Genetic Counselor, Stanford Cancer Genetics Clinic Assistant Professor of Pediatrics - Genetic Counseling Learning Goals • Understanding sporadic v. familial v. hereditary cancers • Patterns of inheritance of hereditary cancer risk • Characteristics of inherited cancer syndromes • Goals of genetic counseling and testing for cancer syndromes • Diagnosis and management of Hereditary GI cancer syndromes • HNPCC – Lynch syndrome • HBOC • Gene Panels • Targeting BRCA mutant tumors for therapy with PARP inhibitors • DNA sequencing and rare genetic variants – going forward • Cancer Genomics – profiling tumors and personalized oncology Opportunities to Increase Cancer Survival Normal tissue Genetic Risk Assessment Malignant tissue Prevention Distant cancer spread Early detection Early treatment Death Treatment Somatic Germline Genetic testing for cancer risk susceptibility Increased focus on early detection and prevention Tumor molecular profiling & targeted therapies Personalized Medicine in Cancer: Risk Assessment and Prevention Identification of germline and familial genetic alterations that increase risk of cancer Development of targeted screening and early detection techniques prevent development of advanced cancers Incorporation of moderate and low-penetrant, common genetic variants in risk prediction and modification Personalized Medicine in Cancer: Tumor Profiling and Therapeutics Identification of genetic alterations that drive carcinogenesis Disease stratification for better prognostic/predictive markers Development of drugs that can effectively inhibit the function of these genetic alterations Molecularly targeted therapies to be used consistently and effectively in patients with cancer Assessment and prediction of drug resistance mechanisms Genetic Theory of Cancer • Cancer is a genetic disease • Most cancers have mutations in multiple genes • The underlying defect in cancers is Genomic Instability • Cancers require alterations in genes involved in cellular proliferation, cell cycle, apoptosis, telomere maintenance and DNA repair • Most inherited cancer syndromes are due to alterations in genes required for genomic stability. The Development of Hereditary Cancer Nonhereditary Mother or Father Hereditary 1 damaged gene 1 normal gene 2 normal genes 1 damaged gene 1 normal gene Loss of normal gene 1 damaged gene 1 normal gene Loss of normal gene Characteristics of Inherited Cancer Syndromes Sporadic vs. Familial vs. Hereditary Cancer Sporadic Cancers account for the vast majority of tumors occur without marked family history or early age Familial Cancers 5 - 20% of most common tumors show familial clustering may be due to chance, shared environmental factors or genes Hereditary Cancers account for 5 - 10% of cancers recognizable inheritance pattern (usually autosomal dominant) early age of onset, multiple primary cancers identified germline genetic alterations Cardinal Features of Hereditary Cancers • Early age of cancer onset • Multiple primary cancers showing specific combinations within the patient’s family • Excess of multifocal, bilateral or multiple primary cancers • Physical stigmata • Distinctive pathological features • Occasional differences in survival and clinical severity • Dominant pattern of transmission, with marked variability in phenotypic expressivity and gene penetrance Autosomal Dominant Inheritance Each child has 50% chance of inheriting the mutation No “skipped generations” Equally transmitted by men and women Normal Cancer more typical . . . Normal Affected Most Cancer Susceptibility Genes Are Dominant With Incomplete Penetrance Normal Susceptible Carrier Carrier, affected with cancer Sporadic cancer Penetrance is often incomplete May appear to “skip” generations Individuals inherit altered cancer susceptibility gene, not cancer Age-Specific Penetrance Percentage of individuals with an altered disease gene who develop the disease 100 Affected with colorectal cancer (%) 80 HNPCC mutation carriers 60 40 General population 20 0 0 20 40 60 80 Autosomal Dominant Inherited Cancer Syndromes • Breast and Ovarian Cancer • Colon Cancer and Polyposis HNPCC FAP Polyposis Cowdens Peutz-Jehgers Juvenile Polyposis • Other GI Cancers Gastric Pancreas BRCA1&2 MMR APC MYH PTEN STK11 SMAD4 BMPR1A CDH1 p16 • MEN1 Menin • MEN2/MTC RET • VHL VHL • Li-Fraumeni p53 Hereditary Susceptibility to Cancer • Who to test for genetic susceptibility? • What are the risks of cancer associated with known genetic mutations? • What can be done to prevent cancer in unaffected carriers? Genetics of Colorectal Cancer Syndrome Gene(s) Lynch syndrome MLH1, MSH2, MSH6, PMS2, EPCAM Adenomatous polyposis Familial Adenomatous Polyposis(FAP) APC Attenuated FAP APC MYH-associated polyposis MYH (biallelic) Hamartomatous polyposis Peutz-Jeghers Syndrome STK11 Juvenile Polyposis Syndrome SMAD4/BMPR1A Cowden Syndrome PTEN Colorectal Multistep Carcinogenesis Chromosomal Instability APC Normal Colorectal Epithelium K-ras Early Adenoma hMSH2 hMLH1 MMR DCC p53 Intermediate Adenoma Advanced Adenoma ?? Colorectal Carcinoma ?? Invasive Carcinoma TGFBRII MSH3 APC IGFIIR MSH6 BAX PTEN Microsatellite Instability ?? ?? Metastatic Carcinoma Categories of colorectal cancer (CRC) Sporadic (~65%) Rare CRC syndromes (<0.1%) Familial Adenomatous Polyposis (FAP) (1%) Familial Unknown gene (~30%) Hereditary Nonpolyposis Colorectal Cancer (Lynch) (5%) Clinical Features of Lynch Syndrome Early but variable age at CRC diagnosis (~45 years) Tumor site in proximal colon predominates (2/3rds) Extracolonic cancers: endometrium, ovary, stomach, urinary tract, small bowel, bile ducts, brain, sebaceous skin tumors Autosomal pattern of inheritance Contribution of Gene Mutations to HNPCC Families Sporadic Familial Unknown ~30% MSH2 ~30% HNPCC Rare CRC syndromes FAP MSH6 (rare) PMS2 (rare) MLH1 ~30% Cancer Risks in HNPCC 100 80 % with cancer 60 Colorectal 78% Endometrial 43% 40 Stomach 10% Urinary tract 10% Biliary tract 15% Ovarian 9% 20 0 0 20 40 60 Age (years) 80 Surveillance Options for LS Mutation Carriers Malignancy Intervention Recommendation Colorectal Cancer Colonoscopy Begin at age 20 – 25, repeat every 1 – 2 years Endometrial Cancer Transvaginal ultrasound Endometrial aspirate Annually, starting at age 35 Gastric Cancer EGD Begin at age 30 - 35, repeat every 2 – 3 years Renal/Ureteral Urine cytology Annually, starting at age 30 Colonoscopy Improves Survival of Genetically-Confirmed HNPCC Surveillance 100 92.2% 80 No surveillance 73.9% 60 40 0 5 10 Follow-up time (years) 15 Familial Risk for Common Cancers New Paradigm in Cancer Treatment: Targeted Therapy Robust Clinical Tumor Genotyping Assays Cancer Genomic Profiling and Treatment: A New Paradigm Words –More words Words –More words d Use repeat liquid biopsies To monitor response and assess Mechanisms of resistance Genomic Profiling: What to Expect Vogelstein et al. Cancer Genome Landscapes. Science (2013) Slide 4 Miller et al, Foundation Medicine, ASCO 2013. Abstract 11020 Stanford Molecular Tumor Board Workflow Referral to Cancer Genomics Service Tumor Biopsy Pathology Sample Prep Research Consent Coordinator Tissue Bank Molecular analysis (NGS) Analytics & Informatics Molecular Tumor Board Results and Treatment CLIA Lab Research Lab Genetic Counseling Identify Drug Drug Approval Treatment Clinical f/u Genomic testing for patients: example report Challenges: Cancer Genomic Medicine Genomic targets are rare Need for common, cost-effective NGS diagnostics / databases Effective targeted therapies; predictive biomarkers Small sample sizes; alternative endpoints Tumor Heterogeneity Drug Resistance Incidentalome [TITLE] Challenges: Cancer Targets ER Pathway (GATA3, FOXA1, RUNX1) PI3K Pathway (PIK3CA, AKT, mTOR, PTEN) MAP3K, JNK, ERK Cyclin D, CDK4/6 Epigenetic Pathways MDM2/p53 DNA Repair Pathways FGFR Notch HER2 Tumor Heterogeneity Tumor Heterogeneity Tumor Heterogeneity Liquid Biopsies CAPP-Seq Liquid Biopsy Applications: Target Biomarkers Slide 29 Molecularly-guided Trials Trials in Progress –Lung MAP – lung squamous cell carcinoma –FOCUS4 – First-line metastatic colorectal –MODUL - First-line metastatic colorectal –SIGNATURE – not disease-specific –MyPathway – not disease-specific Evolving Trials –MATCH – Any line –not selected by primary site –ASSIGN – 2nd line colorectal – Phase II/III Barriers to Personalized CA Therapy Trials Escalating regulatory burden Access to approved drugs off label Access to investigational agents Tracking patient outcomes Need for new clinical trial paradigms –Prospective randomized vs. observational –Retrospective observational (exceptional responders) Indirect Results: Tumor Whole-Genomes Coming soon . . . . Tumor and germline DNA sequence mostly identical Medical significance of Incidental Genomic Findings often unclear – non-syndromic, penetrance? Germline Variants that will be found in tumors: Disease genes, Disease risk, drug response, VUS Guidelines for “Actionable” Ethics – obligation to inform Consent – opt-in versus opt-out Clinical Outcomes: Intermountain Cohort Study Standard Treatment Cohort Matched Age Gender Diagnosis #Previous trx - No Sequence - Chemo Genomic Treatment Cohort - Sequence - Targeted Trx Compare Outcomes: 1° Progression Free Survival 2° Cost of Care Adverse Events Quality of Life Progression Free Survival: Traditional: 12.0 weeks Targeted: 23.9 weeks Cost of Care: Traditional: $3,473/wk HR: 0.53, p<0.002 Targeted: $3,023/wk p= 0.22 Nadauld (IMH), Ford (Stanford) et al. ASCO 2015 Cancer Genomics Tumor Board Case 49 yo male with widely metastatic CRC – lungs, liver, colon. Progressed through Xelox/Bev, Xeliri, Irinotecan/Cetuximab. Liver biopsy sent for sequencing –HER2 amplification –APC mutation –P53 splice site alteration Trial of Herceptin – no effect Trial of TDM-1 -> Responding! Patient Case: Colon Cancer Future Directions: Germline Genotyping carriers for more accurate risk assessment Multigene panels / NGS for diagnosis Exome / WGS for “mystery” families Identification of novel moderate penetrant genes Calculating risk of multiple low-penetrant alleles VUS: ethnic/racial groups, functional studie Future Directions: Germline Genotyping carriers for more accurate risk assessment Multigene panels / NGS for diagnosis Exome / WGS for “mystery” families Identification of novel moderate penetrant genes Calculating risk of multiple low-penetrant alleles VUS: ethnic/racial groups, functional studie Future Directions: Somatic Tumors Tumor profiling and genotyping will identify more targets Gene panels vs. exomes vs. WGS Targeting multiple alterations simultaneously Clinical trials to assess outcomes –genomic v. empiric; exceptional responders; bucket-trials Non-invasive DNA sampling New technologies and informatics Clinically oriented genomics programs