Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
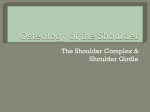
[ research report ] KEVIN D. HARRIS, PT, DSc1 • GAIL D. DEYLE, PT, DSc2 • NORMAN W. GILL, PT, DSc3 • ROBERT R. HOWES, PA-C4 Manual Physical Therapy for Injection-Confirmed Nonacute Acromioclavicular Joint Pain S houlder pain is a common reason for people to seek treatment from a physical therapist. In 2003, approximately 13.7 million people in the United States required medical care for shoulder pain,11 and the 12- TTSTUDY DESIGN: Prospective single-cohort study. TTOBJECTIVES: To determine and document changes in pain and disability in patients with primary, nonacute acromioclavicular joint (ACJ) pain treated with a manual therapy approach. TTBACKGROUND: To our knowledge, there are no published studies on the physical therapy management of nonacute ACJ pain. Manual physical therapy has been successful in the treatment of other shoulder conditions. TTMETHODS: The chief inclusion criterion was greater than 50% pain relief with an ACJ diagnostic injection. Patients were excluded if they had sustained an ACJ injury within the previous 12 months. Treatment was conducted utilizing a manual physical therapy approach that addressed all associated impairments in the shoulder girdle and cervicothoracic spine. The primary outcome measure was the Shoulder Pain and Disability Index. Secondary measures were the American Shoulder and Elbow Surgeon and global rating of change scales. Outcomes were collected at baseline, 4 weeks, and 6 months. The Shoulder Pain and Disability Index and American Shoulder and Elbow Surgeon scale values were analyzed with a repeated-measures analysis of variance. month prevalence of shoulder pain has been estimated to be 30%, which is second only to low SUPPLEMENTAL VIDEO ONLINE back pain.50 Acromioclavicular joint (ACJ) disease is reported to be present in 31% of all patients with shoulder pain.48 Additionally, as many as TTRESULTS: Thirteen patients (11 male; mean 41% of all shoulder injuries in an athletic SD age, 41.1 9.6 years) completed treatpopulation involve the ACJ.33 Nearly half ment consisting of an average of 6.4 sessions. of the patients who sustain a grade I or Compared to baseline, there was a statistically II ACJ injury have a symptomatic ACJ 6 significant and clinically meaningful improvement for the Shoulder Pain and Disability Index years after injury.43 Pain and dysfunction at 4 weeks (P = .001; mean, 25.9 points; 95% of ACJ origin may lead to an inability to confidence interval [CI]: 11.9, 39.8) and 6 months perform manual labor tasks and sports (P<.001; mean, 29.8 points; 95% CI: 16.5, 43.0), and difficulty with activities of daily and the American Shoulder and Elbow Surgeon living. scale at 4 weeks (P<.001; mean, 27.9 points; 95% The ACJ is a synovial joint that proCI: 14.7, 41.1) and 6 months (P<.001; mean, 32.6 vides the scapula with additional range points; 95% CI: 21.2, 43.9). of rotation on the thorax, which allows TTCONCLUSION: Statistically significant and the scapula to adjust outside of its initial clinically meaningful improvements were observed in all outcome measures at 4 weeks and 6 plane (posterior tipping and internal romonths, following a short series of manual therapy tation) to follow the changing shape of interventions. These results, in a small cohort of the thorax as arm movement occurs.34,36 patients, suggest the efficacy of this treatment Recent biomechanical studies demonapproach but need to be verified by a randomized strated the ACJ’s significant role in overcontrolled trial. all shoulder motion, which suggests that TTLEVEL OF EVIDENCE: Therapy, level 4. J the ACJ should not be overlooked in any Orthop Sports Phys Ther 2012:42(2):66-80, Epub patient with shoulder pain.36-38,58 We hy25 October 2011. doi:10.2519/jospt.2012.3866 pothesize that the nonacute symptomTTKEY WORDS: distal clavicle excision, atic ACJ behaves in a physical manner manipulation, mobilization, Mumford, shoulder similar to that of other symptomatic or Clinical Education Director, Physical Therapy Service; Fellow, Army-Baylor University Doctoral Fellowship in Orthopaedic Manual Physical Therapy, Brooke Army Medical Center, Fort Sam Houston, TX. 2Professor, Baylor University Graduate School, Senior Faculty, Army-Baylor University Doctoral Fellowship in Orthopaedic Manual Physical Therapy, Physical Therapy Service, Brooke Army Medical Center, Fort Sam Houston, TX. 3Graduate Program Director and Associate Professor, Army-Baylor University Doctoral Fellowship in Orthopaedic Manual Physical Therapy, Physical Therapy Service, Brooke Army Medical Center, Fort Sam Houston, TX. 4Program Manager, U.S. Army-Baylor University Doctorate of Science in Physician Assistant Studies in Clinical Orthopaedics, Orthopedics Service, Brooke Army Medical Center, Fort Sam Houston, TX. The Institutional Review Board at Brooke Army Medical Center, Fort Sam Houston, TX approved this study. All participants provided written, informed consent prior to participation. The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Departments of the Army or Defense. Address correspondence to Dr Kevin Harris, Physical Therapy Service, Fort Sam Houston Primary Health Clinic, 3851 Roger Brooke Drive, Fort Sam Houston, TX 78234. E-mail: [email protected]; [email protected] 1 66 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 66 1/18/2012 3:27:01 PM degenerative joints, with loss of motion due to pain, capsular stiffness, and/or bony impingement. Presumably arthritic, stiff and painful joints elsewhere in the body have been shown to respond well to an impairment-based manual physical therapy approach in randomized clinical trials.17,18,28,66 ACJ pain commonly presents with localized superior shoulder pain, tenderness to palpation at the ACJ, and possibly swelling in the presence of distal clavicle osteolysis.6,23,65 Functional limitations of ACJ pain include difficulty with resistance-training activities that place the glenohumeral joint in an extended position.8,9,13,55 Current treatment of chronic ACJ pain can be surgical or nonsurgical. The operative approach, a distal clavicle excision (DCE), or “Mumford” procedure, is commonly performed. 9,21,49 However, since the inception of the DCE in 1941 there have been no clinical trials to our knowledge to define the role of the procedure relative to no intervention or lowerrisk interventions.7,26,44 Current evidence regarding DCE as a treatment option for nonacute ACJ pain is therefore derived from studies comparing different surgical techniques.9,19,21,35,49,53 Surgical complications for these procedures occur in 0% to 64% of cases and include infection, heterotopic ossification, joint instability, suprascapular neuropathy, and distal clavicle fracture, in addition to complications associated with anesthesia. 3,9,12,24,59 Eskola et al20 investigated long-term results of patients managed with DCE for complaints of ACJ pain and reported that nearly 1 in 3 patients had poor long-term outcomes and advised against DCE for patients with higher functional demands on their shoulders. Current noninvasive management of ACJ pain includes rest, activity modification, oral analgesics, nonsteroidal antiinflammatory medications, and ice. 9,55 However, evidence for these management strategies is lacking.29 Injections of corticosteroids and/or anesthetic agents into the ACJ may also be used.7-9,63 Corticosteroid injections have associated risks that include subcutaneous fat atrophy, dermal thinning, cellulitis, and septic arthritis.8,45 Relief of symptoms via corticosteroid injection is reported to last anywhere from 2 hours to 3 months and cannot be considered a definitive treatment, as demonstrated by multiple, separate prospective cohort studies in which 72% to 81% of patients failed to achieve a lasting benefit.29,30,63 The only identified instance in the literature of nonsurgical management for nonacute ACJ pain is a case report describing the use of glenohumeral mobilizations.14 However, there is evidence to support the use of manual physical therapy for the treatment of individuals with subacromial impingement syndrome (SAIS).2,41,61 Systematic reviews show the benefits of manual therapy compared to other treatments for individuals with SAIS.16,41 These benefits generally include improved strength and function and decreased pain.2 Previous studies of manual physical therapy treatment for SAIS and nonspecific shoulder pain included techniques directed to the ACJ.2,10,51,61,68,69 Despite the body of evidence that includes ACJ treatment, the ACJ may be overlooked when treating common pathology of the shoulder girdle.8 There are no reported negative effects of manual therapy directed to the ACJ in the literature. The purpose of this study was to determine and document the short- and long-term changes in pain and disability following the use of manual physical therapy to treat movement impairments and painful structures in the shoulder girdle, upper extremity, chest, and cervicothoracic spine in patients with nonacute ACJ pain. METHODS Patients T he study was a prospective, single-cohort design. Consecutive patients presenting to the outpatient physical therapy clinic at Brooke Army Medical Center, Fort Sam Houston, TX, between February 2010 and July 2010, with a primary complaint of shoulder pain were screened for eligibility criteria. Inclusion criteria required patients to be 18 years of age or older, to be able to read, write, and speak sufficient English to complete the self-report outcome questionnaires, and report a greater than 50% pain reduction following an anesthetic-only ACJ injection within the previous 30 days. Relief of pain after an injection containing anesthetic into the joint space of the ACJ is considered the gold standard in diagnosing primary ACJ pain.13,62,65 Patients were excluded if they had a past history of the following: rheumatoid arthritis, connective tissue disorders (eg, systemic lupus erythematosus, Sjogren’s syndrome, or polymyositis/dermatomyositis), infection, neurological deficit, neoplastic growth in the shoulder girdle, fracture or ligamentous injury of any grade to the shoulder girdle within the last 12 months, corticosteroid injection in the ACJ in the last 6 months, ACJ surgery, or inability to attend at least 4 treatment sessions. All patients reviewed and signed a consent form approved by the Institutional Review Board at Brooke Army Medical Center, Fort Sam Houston, TX, prior to participation and the rights of patients were protected. Therapists Three physical therapists participated in the examination and treatment of all patients in this study. The physical therapists were board certified in orthopaedic physical therapy and were either faculty or fellows in training in an orthopaedic manual physical therapy fellowship program. Participating therapists had an average of 9.3 years of clinical experience with a range of 8 to 12 years. In addition to the common backgrounds and training of the physical therapists, a 2-hour collaborative session on ACJ manual examination and treatment techniques and strategies took place prior to beginning the trial. Examination Procedure Patients who were eligible to partici- journal of orthopaedic & sports physical therapy | volume 42 | number 2 | february 2012 | 67 42-02 Harris.indd 67 1/18/2012 3:27:03 PM [ pate were advised of the trial. Once they agreed to participate, the diagnostic injection (50% lidocaine, 50% marcaine) was performed by an orthopaedic physician assistant. The diagnostic process consisted of the patients performing an activity to provoke their shoulder pain and recording the associated pain level. Following the injection, the activity was performed in the same manner and pain was reassessed. The patient was enrolled in the study if there was at least a 50% drop in the pain associated with the above provocative activity. All patients who enrolled in the trial provided demographic information, answered a standard medical history screening questionnaire, completed the Shoulder Pain and Disability Index (SPADI), and completed the American Shoulder Elbow Surgeon (ASES) scale during the initial visit. At the next visit, all patients underwent a thorough examination of the shoulder, chest, arm, and cervicothoracic spine by the treating physical therapist to determine impaired movement and/or strength and the presence of pain and functional limitations. Treatment was then initiated as indicated by the results of the patient interview and the manual examination. Outcome Measures Patients completed the SPADI and the ASES scale at baseline, 4 weeks, and 6 months. The primary outcome measure was the patients’ perceived level of pain and disability, as measured by the SPADI, at the 6-month follow-up visit. The SPADI and the ASES scale are commonly used shoulder-specific self-report questionnaires that have been demonstrated to be valid, reliable, and responsive to change.57 The SPADI consists of 2 subscales, pain and disability, which are combined to produce a total score ranging from 0 (no pain or functional difficulty) to 100 (highest level of pain and functional difficulty). The SPADI is reliable,40 valid,39 and responsive4 for shoulder pain of musculoskeletal, neurogenic, or undetermined origin.27,56,57 The minimal clinically important difference research report (MCID) for the SPADI is 10 points.42,67 The ASES scale consists of equally weighted pain and disability subscales, where the 2 subscales are combined to produce a total score ranging from 0 (highest levels of pain and functional difficulty) to 100 (no pain and no functional difficulty). The pain score of the ASES scale is calculated from a single pain question and a corresponding visual analog scale. The function score of the ASES scale is calculated from the sum of 10 questions addressing function using a 4-point ordinal scale. Two of the 10 functional items on the ASES scale are left blank so that patients may tailor the instrument by writing in additional specific functional activities that are difficult for them to do. The ASES scale is a reliable, valid, and responsive instrument that measures functional limitations and pain in people with musculoskeletal shoulder pathologies.54 The 2 blank write-in questions were transferred at baseline to the 4-week and 6-month forms for each patient. To minimize potential sources of bias, all outcome measures were administered and verified by associate investigators who were not involved with treating the patients. Additionally, at the 4-week and 6-month follow-ups, patients answered a global rating of change (GROC) question, based on the scale described by Jaeschke et al,31 to rate their own perception of overall change in all symptoms. The GROC is a 15-point Likert scale ranging from –7 (“a very great deal worse”) to 0 (“about the same”) to +7 (“a very great deal better”). Intermittent descriptors of worsening or improving are assigned values ranging from –1 to –7 and +1 to +7, respectively. The MCID for the GROC is arbitrary, although it has been reported that scores of +4 and +5 indicate moderate changes in patient status and scores of +6 and +7 indicate large changes in patient status.31,32 Intervention Patients attended a 30-minute clinical session twice a week for 3 weeks after ] enrollment. The treating therapist could decide to add or subtract visits as needed, similar to clinical practice. Patients were asked to keep a log of their medication usage throughout the trial. Patients were not discouraged from engaging in physical activities unless the therapist determined that a specific activity was not well tolerated and directly aggravated their shoulder condition. Patients were not discouraged from seeking additional medical attention or receiving an injection. An impairment-based manual physical therapy approach was used for clinical decision making during examination and treatment.1 The examination focused on identifying impairments to movement, relevant muscular weakness, painful structures, functional limitations, and was tailored to the patients’ tolerance based on the severity and behavior of their symptoms. The manual therapy treatment was also tailored to patient tolerance and focused on addressing the impairments identified during the examination.17,18 Treatment primarily consisted of passive joint mobilization. Although the majority of treatment was focused on the ACJ, manual physical therapy treatments were also administered to the glenohumeral, sternoclavicular, and scapulothoracic joints, as well as the rib cage and cervicothoracic spine if impairments in those regions were judged by the physical therapist to contribute to the patient’s pain, stiffness, functional limitation, or disability.2 The physical therapists continued this tailored approach through subsequent treatment sessions by examining the patient to determine the response to each intervention and repeating or progressing the techniques that produced the desired effects. The primary treatment techniques were passive accessory glides of the distal end of the clavicle with the upper extremity in various physiological positions selected to make the ACJ treatment technique less painful. At other times, positions were selected to be more consistent with a position of pain during activity. 68 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 68 1/18/2012 3:27:04 PM Commonly used ACJ and glenohumeral joint mobilization techniques and progressions are described in APPENDIX A. Descriptions of these commonly used cervicothoracic techniques can be found in several recent publications.5,25,42,52,60,64 The treating physical therapist documented the quantity of manual treatment performed on each body region. In this study, 1 “treatment” was operationally defined as 3 periods of 30 seconds of mobilization (grades I-IV) or 1 thrust manipulation. The physical therapist could supplement in-clinic treatment with home exercises that reinforced the manual treatment, such as active-assisted shoulder flexion in supine or assisted shoulder internal rotation (APPENDIX B). However, no strengthening or self-mobilization exercises were prescribed by the physical therapists before the 4-week follow-up visit. At the 4-week follow-up visit, patients received instructions for a home-exercise program that consisted of strengthening and range-of-motion exercises. The patients were provided with handouts containing pictures and clear instructions on dosing and exercise progressions. Colored elastic bands were provided for progressive-resistance strengthening. The exercises prescribed were intended to supplement the manual physical therapy provided in the clinic and were chosen from a list of routinely used exercises (APPENDIX B). Patients were instructed to perform the home exercises 3 times per week and were given a log to track their compliance. “Good” compliance was determined to be performance of the program at least twice per week. Patients were invited back to the clinic 4 months after enrollment to determine if any “booster” treatments were necessary. Treatment resumed if the patient and physical therapist mutually agreed that additional treatment was likely to be beneficial. There was no limit on the number of subsequent treatment sessions. Finally, patients returned to the clinic 6 months after enrollment for the final assessment of the outcome measures. Patients were Assessed for eligibility, n = 223 Excluded, n = 208: • Less than 50% pain relief after injection, n = 3 • Did not meet inclusion criteria, n = 189 • Declined to participate, n = 8 • Presented with contraindications, n = 1 • Sustained recent trauma, n=4 • Received corticosteroid injection, n = 3 Enrolled, n = 15 Attended initial appointment, n = 14 Never returned for initial appointment, n = 1 Treatment provided twice per week for 3 wk 4-wk follow-up, n = 13 Unable to make time commitment, n=1 6-mo follow-up, n = 13 FIGURE 1. Flow diagram of patient recruitment and retention. also asked about the medications they were taking for their shoulder pain, their current activity level, home exercise program compliance, any subsequent injuries, and whether they had sought other care for their shoulder pain. Data Analysis The study had a single-group, withinsubjects, repeated-measures design, with 1 independent variable and 3 dependent variables. The independent variable was time with 3 levels (baseline, 4 weeks, and 6 months). The dependent variables were the SPADI, ASES scale, and GROC values. Descriptive statistics, including frequency counts for categorical variables and measures of central tendency and dispersion for continuous variables were calculated to summarize the data. Statistical model assumptions of normality and sphericity were assessed and the Greenhouse-Geisser correction was used for any comparisons found to violate the journal of orthopaedic & sports physical therapy | volume 42 | number 2 | february 2012 | 69 42-02 Harris.indd 69 1/18/2012 3:27:05 PM [ sphericity assumption. The primary outcome of interest was change in SPADI values over time. This was examined with a 1-way repeated-measures analysis of variance, with the alpha level set at .05, and time (baseline, 4 weeks, and 6 months) as the within-subjects factor. The ASES scale values were also analyzed in this manner. Planned pairwise comparisons were performed to examine the differences between baseline and the follow-up periods using Sidak correction and with 95% confidence intervals (CIs) also calculated for mean differences. An intention-to-treat analysis was planned to account for any dropouts, with missing data substituted by the “last value carried forward” method. Frequency distributions and a mean value were determined for the GROC. All data were analyzed using SPSS Version 16.0 for Windows software (SPSS Inc, Chicago, IL). research report TABLE 1 ] Baseline Demographics Variable Value Patients, n 13 Gender (male/female), n 11/2 Age (mean SD), y 41.1 9.6 Median symptom duration (range), mo 6 (2-240) Dominant side affected, n 6 Normal radiographs per radiologist, n 4 Taking medication for shoulder, n 5 100 90 80 70 60 50 40 RESULTS T wo hundred twenty-three patients with a primary complaint of shoulder pain were screened for possible eligibility criteria. Of the 26 patients who were offered participation, 6 declined due to the time commitment, 2 did not want the injection, and 3 did not achieve at least 50% pain relief following the injection. Fifteen patients, therefore, met the inclusion criteria and consented to participate in the study. One participant failed to return after enrollment but before any treatment, and another patient began treatment but only completed 2 treatment sessions due to military training requirements (FIGURE 1). Thirteen patients (mean SD age, 41.1 9.6 years; 85% male; symptom duration range, 2 to 240 months) completed treatment as prescribed and returned for follow-up visits at 4 weeks and 6 months (TABLE 1). The average number of treatment sessions was 6.4, which included booster visits for 3 patients. Between baseline and the 6-month follow-up visit, none of the patients sought additional medical care, had a subse- 34.6 30 20 10 8.7* 4.8† 0 Baseline 4 wk 6 mo FIGURE 2. Means and standard deviations for the Shoulder Pain and Disability Index (SPADI) scores. Two subscales, consisting of pain and disability, are combined to produce a total score ranging from 0 (no pain or functional difficulty) to 100 (highest levels of pain and functional difficulty). The minimal clinically important difference for the SPADI is 10 points.42,67 *Significant difference from baseline (P = .001). †Significant difference from baseline (P<.001). quent injection, decreased their activity level, or increased medication usage for their shoulder pain. Home exercise program compliance was judged to be good in 54% and poor in 15.4% of the cohort; however, by the 6-month follow-up visit, 30.8% stopped the exercises for reasons unrelated to their symptoms or functional limitations. The repeated-measures analysis of variance was statistically significant for the SPADI (F = 29.2, P<.001) and the ASES scale (F = 34.3, P<.001). Post hoc comparisons revealed statistically significant and clinically meaningful improvements compared to baseline for the SPADI at 4 weeks (P = .001; mean, 25.9 points; 95% CI: 11.9, 39.8) and 6 months (P<.001; mean, 29.8 points; 95% CI: 16.5, 43.0) (FIGURE 2) and the ASES scale at 4 weeks (P<.001; mean, 27.9 points; 95% CI: 14.7, 41.1) and 6 months (P<.001; mean, 32.6 points; 95% CI: 21.2, 43.9) (FIGURE 3). The mean SD GROC at 4 weeks was 5.4 1.3, which corresponds to “quite a bit better.” The average SD GROC value at 6 months was 6.3 0.6, which corresponds to “a great deal better.” Individual outcomes at each time point are displayed in TABLE 2. For the 1 patient who began treatment and dropped out, the intention-to-treat 70 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 70 1/18/2012 3:27:07 PM 100 Cx SCJ Tx 2% 1% 4% 92.0* 87.4* 90 80 70 GHJ 15% 59.5 60 50 ACJ 78% 40 30 20 10 0 Baseline 4 wk 6 mo FIGURE 3. Means and standard deviations for the American Shoulder and Elbow Surgeon (ASES) scores. Minimal clinically important difference is 6.4. The ASES consists of equally weighted pain and disability subscales, where the 2 subscales are combined to produce a total score ranging from 0 (highest levels of pain and functional difficulty) to 100 (no pain and no functional difficulty). *Significant difference from baseline (P<.001). TABLE 2 Individual Outcomes SPADI Patient ASES GROC Baseline 4 wk 6 mo Baseline 4 wk 6 mo 4 wk 6 mo 1 16.2 6.9* 4.6 73.3 98.3 98.3 7 6 2 29.2 12.3 2.3 53.3 61.7 98.3 4 7 3 13.9 2.3 4.6* 48.3 96.7 88.3 6 6 4 44.6 16.2 6.2 73.3 83.3 98.3 5 6 5 27.7 5.4 1.5 65.0 81.7 96.7 5 6 6 17.7 3.1 0.0 71.7 98.3 100.0 6 7 7 25.4 6.2 2.3 76.7 85.0 90.0 3 7 8 64.6 3.9 20.0 38.3 74.0 53.3 6 6 9 22.3 13.9* 1.5 68.3 88.3 98.3 4 6 10 22.3 2.3 1.5 56.7 100.0 100.0 7 7 11 31.5 9.2 7.7 66.7 96.7 90.0 7 5 12 67.7 30.0 10.0 51.7 75.0 85.0 4 6 13 66.2 1.5 0.0 30.0 96.7 100.0 6 7 Abbreviations: ASES, American Shoulder and Elbow Surgeon scale; GROC, global rating of change; SPADI, Shoulder Pain and Disability Index. *Change value did not exceed minimal clinically important difference compared to baseline. analysis was conducted by carrying the last value (baseline value) forward. At 4 weeks, the average improvement in SPADI values obtained from this analysis was 24.0 points (P<.001; 95% CI: 13.2, 34.9). As a sensitivity analysis, these results were similar to the analysis of the completers; therefore, we determined that the findings were not sensitive to a more conservative analysis. The ACJ was the primary focus of treatment and 78% of all manual therapy treatment performed in this study targeted that joint (FIGURE 4). All patients FIGURE 4. Treatment provided, with “treatment” operationally defined as 3 periods of 30-second mobilizations (grades I-IV) or 1 repetition of a thrust manipulation (grade V). Abbreviations: ACJ, acromioclavicular joint; Cx, cervical spine; GHJ, glenohumeral joint; SCJ, sternoclavicular joint; Tx, thoracic spine. received manual physical therapy treatment for the ACJ and had at least 1 additional region or joint treated with manual physical therapy techniques. All 450 treatments performed in this study were grade III or IV mobilizations or grade V thrust manipulations into the resistance range of joint motion; no grade I or II joint mobilizations were performed. DISCUSSION W e observed a positive and clinically meaningful improvement in patients who had ACJ pain and dysfunction, as measured by the SPADI and ASES scale, following an average of 6.4 treatment sessions using an impairment-based manual physical therapy approach. The benefits were noted at 4 weeks and persisted to 6 months. These observed changes are clinically important because they exceeded the MCID for the SPADI and the ASES scale. We can be reasonably confident in this observation because the lower boundaries of the 95% CIs exclude the MCID for both outcome measures at both time points.47 Additionally, the raw SPADI scores at 4 weeks and 6 months approached those of an asymptomatic population.15 The GROC values journal of orthopaedic & sports physical therapy | volume 42 | number 2 | february 2012 | 71 42-02 Harris.indd 71 1/18/2012 3:27:08 PM [ indicated moderate to large overall improvement. The observed outcomes in this cohort are consistent with those of other studies that used a similar impairmentbased manual therapy approach for the treatment of subacromial impingement,2 mechanical neck pain,64 knee osteoarthritis,17,18 and lumbar spinal stenosis.66 The manual therapy approach utilized in this study was pragmatic and is generalizable to typical outpatient orthopaedic physical therapy settings. Although we had the ability to confidently diagnose primary ACJ pain in our patients by using a gold standard criterion, a diagnostic injection is typically not necessary in clinical practice. This manual therapy approach, when the history and examination findings suggest ACJ involvement, may be a reasonable strategy even in the absence of a diagnostic injection. In this cohort, the majority of treatment provided was specifically directed to the ACJ. The sample, relative to the number of patients screened for this pathology, was small due to the necessity of recruiting a homogenous group of patients who presented with nonacute primary ACJ pain. However, additional benefits may be derived from treating the ACJ in patients with SAIS because the ACJ may be responsible for some of the symptoms associated with SAIS.22,36,46 The ACJ also may influence the overall function of the shoulder girdle, suggesting that it be included in the examination of shoulder conditions. The observed changes in this trial contradict the opinion by Buttaci et al8 that physical therapists have little to offer patients with chronic ACJ pain. The pain and disability scores in our cohort of patients were similar at baseline, as measured by the ASES scale, to those of a cohort of patients who elected surgical intervention after a diagnosis of primary ACJ pain.9 Additionally, the short-term and long-term outcomes observed in this study were similar to the outcomes of patients who underwent surgery.9 This suggests that a manual physical therapy approach may be a noninvasive option for the population tradi- research report tionally treated with surgery. Clinical Reasoning The impairment-based manual therapy approach utilized in this study was a complex patient-centered process that utilized clinical reasoning and careful clinical decision making. At every encounter, the physical therapist judged the likely tolerance of the patient to the manual forces used in the examination and treatment to limit the possibility of increasing symptoms while achieving timely improvement. These judgments included how much to examine the patient globally, which movements to examine, how vigorously to mobilize, how to monitor pain while treating impaired movement, and the appropriate dosage of mobilizations in a given session. Other treatment decisions included when to layer in additional mobilization techniques and exercises specifically for the ACJ or other regions, and in what manner to progress a manual technique or exercise. Patients were commonly progressed within 2 to 3 visits to higher grade mobilizations in increasingly demanding positions of function based on their response to mobilizations in more neutral positions (APPENDIX A). Exercises were carefully dosed, initially selected to reinforce manual treatment of movement impairments, and later progressed and tailored to include strengthening. Limitations The outcomes of this prospective cohort should be interpreted with caution because, due to the study’s single-group design, a cause-and-effect relationship between the intervention and observed outcomes experienced by the patients cannot be inferred. As such, the efficacy of the intervention program cannot be generalized to a larger population. Potential confounding variables were addressed at the 6-month follow-up visit. None of the patients reported outside treatment and 3 of the 5 patients who were taking medication prior to treatment did not require medication after ] completion. Home exercise program compliance was 54% and the strengthening exercise program did not begin until after the 4-week follow-up. An improvement due to the passage of time is a possible explanation in this design; although, due to the chronic nature of the patients’ symptoms (median duration, 6 months; range, 2-240 months) at enrollment in the study, this is unlikely. Each of these factors may influence the magnitude and direction of change in pain and function in future trials and should therefore be considered accordingly. The results of this trial offer preliminary data for future research investigating interventions for nonacute ACJ pain. Future studies should include comparisons between this approach and other approaches or sham treatment and could possibly include comparisons of this impairment-based manual therapy approach to steroid injections or surgery. Moreover, the contribution of the ACJ to the signs and symptoms associated with other shoulder conditions should be investigated. CONCLUSION S tatistically significant and clinically meaningful short-term and long-term improvements in shoulder pain and disability were observed in a prospective cohort of 13 patients with nonacute ACJ pain who were treated with 6 sessions of impairmentbased manual therapy. Because this was a small cohort of patients without a comparison group, the efficacy of this intervention cannot be determined. However, the positive changes observed are similar to those seen in randomized trials of other orthopaedic conditions treated with a similar manual therapy approach. These results may provide clinical guidance as preliminary evidence of a low-risk, lowcost, pragmatic approach for the treatment of nonacute ACJ pain. t KEY POINTS FINDINGS: Statistically significant and 72 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 72 1/18/2012 3:27:10 PM clinically meaningful reductions in shoulder pain and disability were observed in a prospective cohort of patients with nonacute ACJ pain treated using an impairment-based manual therapy approach for an average of 6.4 treatment sessions. These results remained at 6 months. IMPLICATIONS: Physical therapists should consider using a comprehensive manual therapy approach to manage patients with nonacute ACJ pain. CAUTION: As a single-group study, cause and effect cannot be inferred. REFERENCES 11. 12. 13. 14. 15. 1. A merican Academy of Orthopaedic Manual Physical Therapists. Orthopaedic Manual Physical Therapy Description of Advanced Specialty Practice. Tallahassee, FL: American Academy of Orthopaedic Manual Physical Therapists; 2008. 2. Bang MD, Deyle GD. Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome. J Orthop Sports Phys Ther. 2000;30:126-137. 3. Blazar PE, Iannotti JP, Williams GR. Anteroposterior instability of the distal clavicle after distal clavicle resection. Clin Orthop Relat Res. 1998;114-120. 4. Bot SD, Terwee CB, van der Windt DA, Bouter LM, Dekker J, de Vet HC. Clinimetric evaluation of shoulder disability questionnaires: a systematic review of the literature. Ann Rheum Dis. 2004;63:335-341. 5. Boyles RE, Ritland BM, Miracle BM, et al. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. 2009;14:375-380. http://dx.doi.org/10.1016/j.math.2008.05.005 6. Burbank KM, Stevenson JH, Czarnecki GR, Dorfman J. Chronic shoulder pain: part I. Evaluation and diagnosis. Am Fam Physician. 2008;77:453-460. 7. Burbank KM, Stevenson JH, Czarnecki GR, Dorfman J. Chronic shoulder pain: part II. Treatment. Am Fam Physician. 2008;77:493-497. 8. Buttaci CJ, Stitik TP, Yonclas PP, Foye PM. Osteoarthritis of the acromioclavicular joint: a review of anatomy, biomechanics, diagnosis, and treatment. Am J Phys Med Rehabil. 2004;83:791-797. 9. Charron KM, Schepsis AA, Voloshin I. Arthroscopic distal clavicle resection in athletes: a prospective comparison of the direct and indirect approach. Am J Sports Med. 2007;35:53-58. http://dx.doi.org/10.1177/0363546506294855 10. Chen JF, Ginn KA, Herbert RD. Passive mobilisation of shoulder region joints plus advice and ex- 16. 17. 18. 19. 20. 21. 22. 23. 24. ercise does not reduce pain and disability more than advice and exercise alone: a randomised trial. Aust J Physiother. 2009;55:17-23. Choi K, Swierzewski SJ, III. Shoulder pain overview, anatomy of the shoulder. Available at: http://www.rheumatologychannel.com/shoulderpain/index.shtml. Accessed December 12, 2011. Chronopoulos E, Gill HS, Freehill MT, Petersen SA, McFarland EG. Complications after open distal clavicle excision. Clin Orthop Relat Res. 2008;466:646-651. http://dx.doi.org/10.1007/ s11999-007-0084-4 Chronopoulos E, Kim TK, Park HB, Ashenbrenner D, McFarland EG. Diagnostic value of physical tests for isolated chronic acromioclavicular lesions. Am J Sports Med. 2004;32:655-661. Cibulka MT, Hunter HC. Acromioclavicular joint arthritis treated by mobilizing the glenohumeral joint. A case report. Phys Ther. 1985;65:1514-1516. Clarke MG, Dewing CB, Schroder DT, Solomon DJ, Provencher MT. Normal shoulder outcome score values in the young, active adult. J Shoulder Elbow Surg. 2009;18:424-428. http://dx.doi. org/10.1016/j.jse.2008.10.009 Desmeules F, Cote CH, Fremont P. Therapeutic exercise and orthopedic manual therapy for impingement syndrome: a systematic review. Clin J Sport Med. 2003;13:176-182. Deyle GD, Allison SC, Matekel RL, et al. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther. 2005;85:1301-1317. Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial. Ann Intern Med. 2000;132:173-181. Elhassan B, Ozbaydar M, Diller D, Massimini D, Higgins LD, Warner JJ. Open versus arthroscopic acromioclavicular joint resection: a retrospective comparison study. Arthroscopy. 2009;25:1224-1232. http://dx.doi.org/10.1016/j. arthro.2009.06.010 Eskola A, Santavirta S, Viljakka HT, Wirta J, Partio TE, Hoikka V. The results of operative resection of the lateral end of the clavicle. J Bone Joint Surg Am. 1996;78:584-587. Freedman BA, Javernick MA, O’Brien FP, Ross AE, Doukas WC. Arthroscopic versus open distal clavicle excision: comparative results at six months and one year from a randomized, prospective clinical trial. J Shoulder Elbow Surg. 2007;16:413-418. http://dx.doi.org/10.1016/j. jse.2006.10.006 Fu FH, Harner CD, Klein AH. Shoulder impingement syndrome. A critical review. Clin Orthop Relat Res. 1991;162-173. Gerber C, Galantay RV, Hersche O. The pattern of pain produced by irritation of the acromioclavicular joint and the subacromial space. J Shoulder Elbow Surg. 1998;7:352-355. Ghodadra N, Lee GH, Kung P, Busfield BT, 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. Kharazzi FD. Distal clavicle fracture as a complication of arthroscopic distal clavicle resection. Arthroscopy. 2009;25:929-933. http://dx.doi. org/10.1016/j.arthro.2009.02.008 Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Gutierrez-Vega Mdel R. Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. 2009;39:20-27. http://dx.doi.org/10.2519/jospt.2009.2914 Gurd FB. The treatment of complete dislocation of the outer end of the clavicle: an hitherto undescribed operation. Ann Surg. 1941;113:1094-1098. Heald SL, Riddle DL, Lamb RL. The shoulder pain and disability index: the construct validity and responsiveness of a region-specific disability measure. Phys Ther. 1997;77:1079-1089. Hoeksma HL, Dekker J, Ronday HK, et al. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomized clinical trial. Arthritis Rheum. 2004;51:722-729. http:// dx.doi.org/10.1002/art.20685 Hossain S, Jacobs LG, Hashmi R. The long-term effectiveness of steroid injections in primary acromioclavicular joint arthritis: a five-year prospective study. J Shoulder Elbow Surg. 2008;17:535-538. http://dx.doi.org/10.1016/j. jse.2007.12.001 Jacob AK, Sallay PI. Therapeutic efficacy of corticosteroid injections in the acromioclavicular joint. Biomed Sci Instrum. 1997;34:380-385. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10:407-415. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a minimal important change in a disease-specific Quality of Life Questionnaire. J Clin Epidemiol. 1994;47:81-87. Kaplan LD, Flanigan DC, Norwig J, Jost P, Bradley J. Prevalence and variance of shoulder injuries in elite collegiate football players. Am J Sports Med. 2005;33:1142-1146. http://dx.doi. org/10.1177/0363546505274718 Levangie PK, Norkin CC. Joint Structure and Function: A Comprehensive Analysis. 4th ed. Philadelphia, PA: F.A. Davis Company; 2005. Levine WN, Soong M, Ahmad CS, Blaine TA, Bigliani LU. Arthroscopic distal clavicle resection: a comparison of bursal and direct approaches. Arthroscopy. 2006;22:516-520. http://dx.doi. org/10.1016/j.arthro.2006.01.013 Ludewig PM, Braman JP. Shoulder impingement: biomechanical considerations in rehabilitation. Man Ther. 2011;16:33-39. http://dx.doi. org/10.1016/j.math.2010.08.004 Ludewig PM, Phadke V, Braman JP, Hassett DR, Cieminski CJ, LaPrade RF. Motion of the shoulder complex during multiplanar humeral elevation. J Bone Joint Surg Am. 2009;91:378-389. http:// dx.doi.org/10.2106/JBJS.G.01483 Ludewig PM, Reynolds JF. The association of scapular kinematics and glenohumeral joint pathologies. J Orthop Sports Phys Ther. journal of orthopaedic & sports physical therapy | volume 42 | number 2 | february 2012 | 73 42-02 Harris.indd 73 1/18/2012 3:27:10 PM [ 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 2009;39:90-104. http://dx.doi.org/10.2519/ jospt.2009.2808 MacDermid JC, Solomon P, Prkachin K. The Shoulder Pain and Disability Index demonstrates factor, construct and longitudinal validity. BMC Musculoskelet Disord. 2006;7:12. http://dx.doi. org/10.1186/1471-2474-7-12 Michener LA, Leggin BG. A review of self-report scales for the assessment of functional limitation and disability of the shoulder. J Hand Ther. 2001;14:68-76. Michener LA, Walsworth MK, Burnet EN. Effectiveness of rehabilitation for patients with subacromial impingement syndrome: a systematic review. J Hand Ther. 2004;17:152-164. http:// dx.doi.org/10.1197/j.jht.2004.02.004 Mintken PE, Cleland JA, Carpenter KJ, Bieniek ML, Keirns M, Whitman JM. Some factors predict successful short-term outcomes in individuals with shoulder pain receiving cervicothoracic manipulation: a single-arm trial. Phys Ther. 2010;90:26-42. http://dx.doi.org/10.2522/ ptj.20090095 Mouhsine E, Garofalo R, Crevoisier X, Farron A. Grade I and II acromioclavicular dislocations: results of conservative treatment. J Shoulder Elbow Surg. 2003;12:599-602. http://dx.doi. org/10.1016/S1058274603002155 Mumford EB. Acromioclavicular dislocation: a new operative treatment. J Bone Joint Surg Am. 1941;23:799-802. Murdoch DM, McDonald JR. Mycobacterium avium-intracellulare cellulitis occurring with septic arthritis after joint injection: a case report. BMC Infect Dis. 2007;7:9. http://dx.doi. org/10.1186/1471-2334-7-9 Neer CS, 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54:41-50. Noteboom JT, Allison SC, Cleland JA, Whitman JM. A primer on selected aspects of evidencebased practice to questions of treatment. Part 2: interpreting results, application to clinical practice, and self-evaluation. J Orthop Sports Phys Ther. 2008;38:485-501. http://dx.doi. org/10.2519/jospt.2008.2725 Ostor AJ, Richards CA, Prevost AT, Speed CA, Hazleman BL. Diagnosis and relation to general health of shoulder disorders presenting to primary care. Rheumatology (Oxford). 2005;44:800-805. http://dx.doi.org/10.1093/ rheumatology/keh598 Pensak M, Grumet RC, Slabaugh MA, Bach BR, Jr. Open versus arthroscopic distal clavicle research report 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. resection. Arthroscopy. 2010;26:697-704. http:// dx.doi.org/10.1016/j.arthro.2009.12.007 Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain. 2003;102:167-178. Pribicevic M, Pollard H. Rotator cuff impingement. J Manipulative Physiol Ther. 2004;27:580-590. http://dx.doi.org/10.1016/j. jmpt.2004.10.004 Puentedura EJ, Landers MR, Cleland JA, Mintken PE, Huijbregts P, Fernandez-de-Las-Penas C. Thoracic spine thrust manipulation versus cervical spine thrust manipulation in patients with acute neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. 2011;41:208-220. http://dx.doi.org/10.2519/jospt.2011.3640 Rabalais RD, McCarty E. Surgical treatment of symptomatic acromioclavicular joint problems: a systematic review. Clin Orthop Relat Res. 2007;455:30-37. http://dx.doi.org/10.1097/ BLO.0b013e31802f5450 Richards RR, An K-N, Bigliani LU, et al. A standardized method for the assessment of shoulder function. J Shoulder Elbow Surg. 1994;3:347-352. http://dx.doi.org/10.1016/ S1058-2746(09)80019-0 Rios CG, Mazzocca AD. Acromioclavicular joint problems in athletes and new methods of management. Clin Sports Med. 2008;27:763-788. http://dx.doi.org/10.1016/j.csm.2008.06.006 Roach KE, Budiman-Mak E, Songsiridej N, Lertratanakul Y. Development of a shoulder pain and disability index. Arthritis Care Res. 1991;4:143-149. Roy JS, MacDermid JC, Woodhouse LJ. Measuring shoulder function: a systematic review of four questionnaires. Arthritis Rheum. 2009;61:623632. http://dx.doi.org/10.1002/art.24396 Sahara W, Sugamoto K, Murai M, Yoshikawa H. Three-dimensional clavicular and acromioclavicular rotations during arm abduction using vertically open MRI. J Orthop Res. 2007;25:12431249. http://dx.doi.org/10.1002/jor.20407 Strauss EJ, Barker JU, McGill K, Verma NN. The evaluation and management of failed distal clavicle excision. Sports Med Arthrosc. 2010;18:213-219. http://dx.doi.org/10.1097/ JSA.0b013e3181e892da Strunce JB, Walker MJ, Boyles RE, Young BA. The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain. J Man Manip Ther. 2009;17:230-236. Tate AR, McClure PW, Young IA, Salvatori R, ] 62. 63. 64. 65. 66. 67. 68. 69. Michener LA. Comprehensive impairment-based exercise and manual therapy intervention for patients with subacromial impingement syndrome: a case series. J Orthop Sports Phys Ther. 2010;40:474-493. http://dx.doi.org/10.2519/ jospt.2010.3223 van Riet RP, Bell SN. Clinical evaluation of acromioclavicular joint pathology: sensitivity of a new test. J Shoulder Elbow Surg. 2011;20:73-76. http://dx.doi.org/10.1016/j.jse.2010.05.023 van Riet RP, Goehre T, Bell SN. The long term effect of an intra-articular injection of corticosteroids in the acromioclavicular joint. J Shoulder Elbow Surg. In press. http://dx.doi.org/10.1016/j. jse.2011.05.010 Walker MJ, Boyles RE, Young BA, et al. The effectiveness of manual physical therapy and exercise for mechanical neck pain: a randomized clinical trial. Spine (Phila Pa 1976). 2008;33:2371-2378. http://dx.doi.org/10.1097/ BRS.0b013e318183391e Walton J, Mahajan S, Paxinos A, et al. Diagnostic values of tests for acromioclavicular joint pain. J Bone Joint Surg Am. 2004;86-A:807-812. Whitman JM, Flynn TW, Childs JD, et al. A comparison between two physical therapy treatment programs for patients with lumbar spinal stenosis: a randomized clinical trial. Spine (Phila Pa 1976). 2006;31:2541-2549. http://dx.doi. org/10.1097/01.brs.0000241136.98159.8c Williams JW, Jr., Holleman DR, Jr., Simel DL. Measuring shoulder function with the Shoulder Pain and Disability Index. J Rheumatol. 1995;22:727-732. Winters JC, Sobel JS, Groenier KH, Arendzen HJ, Meyboom-de Jong B. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomised, single blind study. BMJ. 1997;314:1320-1325. Yiasemides R, Halaki M, Cathers I, Ginn KA. Does passive mobilization of shoulder region joints provide additional benefit over advice and exercise alone for people who have shoulder pain and minimal movement restriction? A randomized controlled trial. Phys Ther. 2011;91:178189. http://dx.doi.org/10.2522/ptj.20100111 @ MORE INFORMATION WWW.JOSPT.ORG 74 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 74 1/18/2012 3:27:11 PM APPENDIX A COMMONLY USED ACROMIOCLAVICULAR JOINT MOBILIZATIONS AND LINES OF PROGRESSION Caudal Glide Progression Arm at side Arm in abduction Prone, arm flexed Impairments with caudal glide commonly found with difficulty in elevating arm Loaded position Progression of position and grade of mobilization Caudal Glides, Grades I-V • P atient position - Supine, arm at side, minimal glenohumeral joint (GHJ) extension • Therapist position - Place the tips of both thumbs on the superior surface of the clavicle adjacent to the acromioclavicular joint (ACJ); spread fingers out for stability - Position forearms in line with the caudal movement at the ACJ • Mobilization technique - Graded oscillatory mobilization is applied by the arms, acting through stable thumbs - May span the joint or be proximal to joint along distal clavicle - May alter angle to a more medially directed force Alternate Technique for ACJ Caudal Glides • L ay “passive thumb” along distal clavicle • Apply caudally directed force through opposite pisiform journal of orthopaedic & sports physical therapy | volume 42 | number 2 | february 2012 | 75 42-02 Harris.indd 75 1/18/2012 3:27:14 PM [ research report ] APPENDIX A Caudal Glides in Abduction • P atient position - Supine, arm abducted, minimal GHJ extension • Therapist position - Place the tips of both thumbs on the superior surface of the clavicle adjacent to the ACJ; spread fingers out for stability - Position forearms in line with the caudal movement at the ACJ • Mobilization technique - Graded oscillatory mobilization is applied by the arms, acting through stable thumbs - May span the joint or be proximal to joint along distal clavicle - May alter angle to a more medially directed force Caudal Glides in Prone Flexion • P atient position - Prone upper extremity flexed overhead with forearm resting on chair • Therapist position - Standing at patient’s head - Thumbs on distal clavicle, fingers splayed out for stability • Mobilization technique - Apply caudally directed mobilization Caudal Glides in Loaded Position • P atient position - Prone on elbows • Therapist position - Standing - Thumbs on distal clavicle • Mobilization technique - Caudal 76 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 76 1/18/2012 3:27:15 PM APPENDIX A Caudal Glides in Loaded Adduction • P atient position - Prone on elbows - Leaning to ipsilateral side • Therapist position - Standing - Thumbs on distal clavicle • Mobilization technique - Caudal Caudal Glides in Loaded Position • P atient position - Prone - Arm abducted and off plinth - Hand in contact with surface • Therapist position - Standing - Thumbs on distal clavicle • Mobilization technique - Caudal glide Anterior to Posterior (AP) Glide Progression Seated, internal rotation bias Arm at side Impairments with AP glide commonly found with difficulty in horizontal adduction or internal rotation Seated Seated, flexed, horizontally adducted Progression of position and grade of mobilization journal of orthopaedic & sports physical therapy | volume 42 | number 2 | february 2012 | 77 42-02 Harris.indd 77 1/18/2012 3:27:16 PM [ research report ] APPENDIX A AP Glides in Supine, Grades I-V • P atient position - Supine • Therapist position - Place the tips of both thumbs on the anterior surface of the clavicle adjacent to the ACJ; spread fingers out for stability - Position forearms in line with the posterior movement at the ACJ • Mobilization technique - Graded oscillatory mobilization is applied by the body and arms, acting through stable thumbs - Pad of the outer thumb should feel the joint motion (feel for the stationary acromion process) - Variations: use the pisiform to apply posterior mobilization or use acromioclavicular (AC) shear test technique AP Mobilization in Sitting, Grades I-V AP Mobilization in Sitting, Grades I-V • P atient position - Seated • Therapist position - Standing perpendicular to shoulder - Apply 1 hand along distal clavicle - Apply the other hand across posterior acromion • Mobilization technique - Apply graded AP mobilization 78 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 78 1/18/2012 3:27:17 PM APPENDIX A AP Mobilization, Grades I-V, for Internal Rotation Bias • S ame as previous technique, except preposition patient in internal rotation • Progress position, grade, and/or dosage as tolerated AP Mobilization in Flexion, Grades I-V, for Horizontal Adduction Bias • P atient position - Seated or standing - Forearm resting on stable surface (plinth, cabinet, etc) • Therapist position - Perpendicular to shoulder - AP hand position • Mobilization technique - Apply graded AP mobilization Posterior-to-Anterior (PA) Mobilization in Prone, Grades I-V • P atient position - Prone - Arm off table • Therapist position - Standing near axilla of patient - Place the tips of both thumbs on the posterior distal clavicle • Mobilization technique - Apply graded PA mobilization - May combine with previous "loaded" techniques journal of orthopaedic & sports physical therapy | volume 42 | number 2 | february 2012 | 79 42-02 Harris.indd 79 1/18/2012 3:27:19 PM [ research report ] APPENDIX A Clavicle Rotation (Wiggle) • P atient position - Supine • Therapist position - Stand near the patient's shoulder, facing toward the clavicle - Gently grip the mid clavicle, using the thumbs on the inferior edge and fingertips superiorly • Mobilization technique - Apply a gentle mobilization force using a rocking or "wiggling" motion through repetitive wrist flexion and extension - Works as a nice, easing technique following direct AC and/or sternoclavicular (SC) joint mobilizations APPENDIX B LIST OF THERAPEUTIC EXERCISES To be performed in a well tolerated and painless manner. Range of Motion These may be performed as passive, active-assisted, or active movements, as determined by the therapist. • Flexion in upright or supine position • Internal rotation using a cane behind the back • Anterior chest and shoulder stretch (pectoralis major stretch) • Horizontal adduction Strengthening • Pain-free push-up progression - Start with wall push-ups not exceeding 90° of elbow flexion - Progress to varying angles of trunk inclination • Resisted tubing - Internal rotation - External rotation - Flexion to 90° - Abduction in the plane of the scapula to 90° • Scapular stabilization progression (scapular retraction/protraction) - Progression • On all fours with elbows straight • Incline push-up position • Regular push-up position 80 | february 2012 | volume 42 | number 2 | journal of orthopaedic & sports physical therapy 42-02 Harris.indd 80 1/18/2012 3:27:19 PM