Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
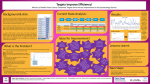
What gets in the way of Faster Cancer Treatment? A review of factors that cause patients to delay or decline treatment Marie Young and Lisa Reynolds Cancer Support: Psychology and Social Work Counties Manukau Health Auckland, New Zealand Acknowledgements • Co-investigators: Frances James, Vanessa Garcia-Hoyos, Karin Jansen, Jackie Chadwick, Allan Edmondson, PWCC Consumer Council • Patients who have generously given their time and shared their experiences • Richard Small, Carl Eagleton, Brad Healey • Anne-Marie Wilkins, Lead Cancer Nurse Coordinator • Leilani Jackson, Pacific Cancer Nurse Coordinator • Tanya Weeks, Maaori Cancer Nurse Coordinator • CM Research Office and Health Intelligence Team Getting cancer treatment quickly • Timely treatment helps to ensure better outcomes and can reduce the stress on patients • However, there are major disparities in accessing treatment for Maaori and Pacific populations • Based on overseas experience, Ministry of Health in NZ introduced the Faster Cancer Treatment (FCT) programme (2014) to reduce waiting times for appointments, tests, and treatment Faster Cancer Treatment (FCT) 62 days Initial symptoms GP visit Referral received FSA 14 days Decision to treat 31 days First treatment Treatment finishes Faster Cancer Treatment (FCT) 62 days Initial symptoms GP visit Referral received Referral received for a patient with a high suspicion of a new cancer (i.e., not recurrence or metastases) FSA Decision to treat First treatment Treatment finishes MOH target – from July 2016, 85% of patients should receive their first cancer treatment within 62 days of referral (90% by June 2017) Research agenda Review the factors that cause patients to delay or decline treatment on the 62 day pathway How many? Who? How come? Stage 1. Analysis of clinical records: • Period Feb 2015 – Jan 2016 • Quantitative analyses – compare patients who met 62 days to those who did not • Identify those who did not meet 62 day target due to patient factors Stage 2. Qualitative analyses: • Understand reasons why patients delay/decline treatment • Clinical notes audit + interviews (approx. n = 20) Feb 2015 – Jan 2016 470 people started treatment after referral with high suspicion of cancer 332 people met the 62 day target (70.6%) 138 people (29.6%) did not 9 people (1.9%) declined Ethnically diverse – 16% Maaori, 21% Pacific, 24% treatment completely Asian, 38% NZ European /other 36% live in significant socioeconomic deprivation How do people who met the 62 day timeline compare to those who did not? No difference in age or gender But, people who did not meet timeline live in greater deprivation (p=.000) Significant difference in ethnicity (p=.001) Significant difference in tumour stream (p=.000) 15% n=17 27.7% n=64 Breast NZ European N=111 N=231 26% 28% n=12 n=12 Asian Lower GI N=47 N=43 44% n=31 45% n=19 NZ Maaori Urological N=71 N=42 Gynae N=38 Pacific N=63 43% n=27 66% n=25 Why? Reasons for delay clinical complications in diagnosis identified in clinical notes distress family prioritisation treatment for another condition treatment barriers due concerns / comorbidities anxiety impact on multiQoL ? factor patient other priorities conflict with beliefs delays to other investigations engagement capacity constraints system understanding emotional time needed avoidance to consider options practical problems faults / mistakes Reasons for delay People who experienced treatment delays clinical due to ‘patient factors’ &/or declined treatment (n=43) How are these people different to everybody else? identified in clinical notes distress family treatment barriers due concerns / comorbidities anxiety impact on multiQoL ? factor patient other priorities conflict with beliefs • No difference in age delays to otherlikely to be • More investigations p=.022) women (χ=5.27, • Difference in ethnicity (χ=18.79, p=.001). Compared to NZ European – Maaorisystem 2.84x, Pacific 4.03x engagement • Difference in cancer type (χ=21.10, p=.004). Women with gynae ca 3.25x practical more likely than with breast cancer understanding emotional time needed problems avoidance to consider Qualitative interviews to gain richer options understanding of patient factors leading delays to Kevin • • • • 76 years, NZ European Urological cancer No idea about timelines or faster cancer treatment Transport issues identified on clinical notes “It’s a volunteer bus that comes and gets you… The appointment was at so and so time, I was there at 9 o’clock, … waiting outside, and they never came.” • No sense that there might have been delays Hepi • • • Tongan, 55 years, Gynaecological cancer Delay reason: ‘patient choice’ – cancelled her specialist appointment to look after her sister going through stem cell transplant • • • Talking to Hepi – other issues evident Gynae bleeding for at least 2 years that she had not consulted a doctor about Routine smear test from family doctor showed clear results – “and I didn’t say anything about my bleeding because I know for sure that she will get it … when doing my smear, my swab” • Hepi spoke up Doris* • • • NZ Maaori, 68 years Gynaecological cancer Delay reason: ‘transport issues’ • want Did not any realhospital]… problems with “I did to perceive come here [local because it timeline was closer to my family to visit me. But she sent me “I always felt I was making decision to Auckland … that’s where the the bestright place is for all you… through journey.” and that all themy doctors are there, the specialists’ and all that’s there… and they said think about yourself, “I actually thought that two months [to have] the worry about yourself, don’t worry about your family, operation was a good time… but in saying that I wish and that gave me the trust in them by pushing me to that it was quicker because obviously I was in a lot of be there... and that’s why I went there. I took that pain, and I was sick of taking Paracetamol every day option, and too bad for my family, they just have to and night. If I wasn’t in the pain I was in I wouldn’t travel.” have minded waiting a bit longer.” Emerging themes • Practical barriers e.g., transport didn’t turn up, couldn’t afford time off work to attend appointment • Family priorities e.g., attend a wedding, babysit grandchildren, look after unwell relatives • Treatment concerns e.g., conflict with traditional medicine, fears about side effects • Distress associated with diagnosis and/or treatment • Prioritising life experiences e.g., go on a holiday (and the doctor said it would be fine) • …. process errors Subtle disadvantage adds up “Subtle but accumulating disadvantage, ultimately producing a substantial treatment disparity…” (Hill et. al, 2013) clinical complications in diagnosis distress family prioritisation treatment for another condition treatment barriers due concerns / comorbidities anxiety impact on multiQoL ? factor patient other priorities conflict with beliefs delays to other investigations engagement capacity constraints system understanding emotional time needed avoidance to consider options practical problems faults / mistakes Inequities in delay • Maaori and Pacific, and people living in greater deprivation much more likely to experience delays to cancer treatment • ‘Patient choice’ is a poor descriptor • ’Small’ issues add up • Pushing people along the pathway isn’t always best for the patient • Next steps: • • • Complete qualitative interviews Simplify the complexity without losing richness of personal stories Change the way we meet our patient’s needs to reduce delays where appropriate (and allow time where appropriate) process errors Questions? “Never worry about numbers. Help one person at a time, and always start with the person nearest you” Mother Teresa