Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
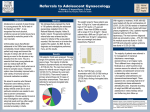
Targets Improve Efficiency! Ministry of Health Faster Cancer Treatment Targets Drive Process Improvement in the Gynaecology Service Background & Aim: In October 2014 the NZ Ministry of Health introduced a new health target: Faster Cancer Treatment (FCT). This target states that by July 2016, 85% of patients receive their first cancer treatment (or other management) within 62 days of being referred with a high suspicion of cancer and needing to be seen within two weeks, increasing to 90% by June 2017. The first publicised reporting period July – Dec 2014 showed none of the DHB’s met the faster cancer treatment target, see the table on the right. Our DHB, Counties Manukau Health (CMH), was one of the worst performing DHBs in the country with only 52% of the FCT patients meeting the target. In response CMH formed a working team of the Service Manager for Medicine, the Lead Cancer Nurse Co-ordinator and Improvement Advisors from Ko Awatea. This team was deployed to working with tumour streams, support services and diagnostic services to support these areas to make improvements that would deliver more timely diagnosis and treatment, as well as reduce the variability. What is the Problem? What: Currently only 14% of the Gynaecology high suspicion of cancer patients meet the Ministry of Health target of 62 days. This was only 0% for April 2015. When: Since July 2014 Where: Cancer Pathways for Gynaecology Service at CMH Scope: From date of receipt of referral to 1st cancer treatment Benefits: • Reduced time from referral received to 1st treatment commenced for FCT patients • Meet MOH 62 day target • Improved/enhanced process and standardization • Timely diagnosis and treatment for FCT patients • Reduced wait and delay time for high suspicion • of cancer patients • Efficient utilization of resources Objectives: Observe and create a high level map for the gynae cancer tumor stream to identify opportunities for improvement that will lead to: • ensuring that at least 85% of the high suspicion of cancer and urgent patients commence treatment within 62 days of secondary care referral by 1 July 2016 • meeting the requirements of the 31 day FCT indicator QR code Current State Analysis: Receive Referral Fail/Pass Fail Fail Total Pass Pass Total Grand Total Grade Referral Tumour Stream Gynaecological Gynaecological First Specialist Appointment (FSA) Diagnostics Results: MultiDisciplinary Meeting (MDM) Decision to Treat First Treatment Values Average of Time to Average of Time to Average of Time to Average of Time to Average of Time to grading FSA MDM decision to treat treatment started 8.24 15.35 52.44 12.31 27.35 8.24 15.35 52.44 12.31 27.35 5.25 8.00 6.00 5.67 9.00 5.25 8.00 6.00 5.67 9.00 7.67 13.95 45.11 11.26 23.18 July 2014 to Sept 2015 Oct 2015 to June 2016 Ideas for Improvement! Introduce dedicated FCT outpatient clinic slots at weekly Thursday clinics Appoint dedicated Cancer Nurse Co-ordinators Introduce standardised MDM templates for effective communication The various improvement interventions tested and implemented by the Gynaecology FCT team have resulted in creation of an improved stable system that is evident by the overall shift in the overall throughput (referral to first treatment) data for the FCT patients. Lessons Learnt: • Partnership between Management and Clinical Leadership is the key to drive improvement and sustained change • Involve all the key stakeholders within the service i.e. management, clinical lead, frontline staff, etc. right from the start • Change takes time! • Each pathway is different with different timeframes. The improvements need to be tailored to make them work. • Patient choice is a huge factor! We need to ensure we take that into consideration and not get stuck on just achieving the target. • A lot of churn for only 10% patients that fit into the target criteria. The service has to process a lot of patients at the start of the pathway who dropout once a negative cancer diagnosis is confirmed. Next Steps: • Enhancing communication with Primary Care to improve quality of referrals • Improve patient engagement with service through education especially Maaori and Pacific Island patients • Maximise ambulatory services to expidite time to diagnosis Project Team (Authors): Adrienne Laing (Service Manager – Gynaecology), Katherine Sowden (Clinical Lead - Gynaecology), Leani Curtis (Cancer Nurse Coordinator), Jennifer van der Westhuizen (Cancer Nurse Coordinator), Sneha Shetty (Improvement Advisor)