Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
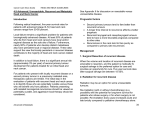
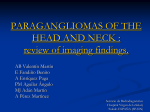
CASE REPORT Amy Chen, MD, Section Editor Multidisciplinary management of locally advanced and widely metastatic paraganglioma in a patient with life-threatening compressive symptoms Vladimir Neychev, MD, PhD,1 David Straughan, MD,2 Karel Pacak, MD, PhD, DSc,3 Electron Kebebew, MD,1* 1 Endocrine Oncology Branch, National Cancer Institute, National Institutes of Health, Bethesda, Maryland, 2Thoracic and Gastrointestinal Oncology Branch, National Cancer Institute, National Institutes of Health, Bethesda, Maryland, 3Section on Endocrinology and Genetics, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, Bethesda, Maryland. Accepted 13 April 2015 Published online 15 June 2015 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.24069 ABSTRACT: Background. Patients presenting with locally advanced, metastatic paraganglioma with life-threatening compressive symptoms of critical anatomic structure pose a significant management challenge. Methods. We present a case of a 15-year-old patient with enlarging right neck mass causing dysphagia and respiratory compromise from near complete obstruction of the oropharynx. Results. Evaluation of the patient’s family history led to the identification of a mutation in the succinate dehydrogenase subunit B (SDSD) gene (G725A). Laboratory and imaging workup revealed an 8.8 3 6.6 3 4.1 cm metabolically and biochemically active right neck mass, a tumor in the left para-aortic region, and multiple bony lesions consistent with widely metastatic disease. Multidisciplinary management included pre- INTRODUCTION Paragangliomas are rare neuroendocrine tumors derived from the neuroendocrine cells of the extra-adrenal autonomic paraganglia that can be found anywhere from the scull base to the pelvis.1 Anatomic site, clinical presentation, and malignant potential of paragangliomas are variable and closely related to the genetic background. The highest malignancy rate is associated with inherited mutations in the B subunit of the succinate dehydrogenase gene (SDHB).2 Patients with SDHB mutations may have multiple catecholamine-secreting abdominal, thoracic, and neck paragangliomas.3,4 Although the standard treatment of locally advanced malignant paraganglioma harboring SDHB mutation is resection of the primary tumor and locoregional disease, the optimal management of patients *Corresponding author: E. Kebebew, Endocrine Oncology Branch (EOB), Building 10-CRC, Room 4–5952, 10 Center Drive, Bethesda, MD 20892. E-mail: [email protected] Consent and Ethics: Written informed consent was obtained from the legal guardian of the patient for publication of this Case Report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal. The manuscript was written in compliance with the Helsinki Declaration. Contract grant sponsor: This work was supported in part by the Intramural Research Program of the Center for Cancer Research, National Cancer Institute. operative clinical optimization, coil embolization, and palliative resection of the neck mass. Conclusion. Although the currently available treatment options for patients with advanced metastatic paraganglioma render no survival benefit, a multidisciplinary management approach aimed at relief of tumor-related symptoms and catecholamine excess should be underC 2015 Wiley Periodicals, Inc. Head Neck 37: E205–E208, 2015 taken. V KEY WORDS: paraganglioma, succinate dehydrogenase gene (SDHB), metastatic disease, compressive symptoms, management approach with advanced, widely metastatic tumors remains illdefined. In this case report, we present a challenging case of a patient with functional multifocal paragangliomas metastatic to lymph nodes and bony skeleton with lifethreatening compressive symptoms from a tumor in the neck. CASE REPORT A 15-year-old boy with a medical history of autism was in his usual state of health until a right neck mass was appreciated by his mother. This was initially attributed to lymphadenopathy secondary to a viral illness and no further medical attention was sought. Over the next 2 years, his mother noticed that his neck mass was enlarging, and he gradually developed difficulties with swallowing solid foods. He was able to tolerate only soft foods and liquids, which resulted in significant weight loss (approximately 20%). He began complaining of unrelenting headaches during the day, and he was more restless with sweating and worsening snoring requiring use of a continuous positive airway pressure machine during sleep. He was also found to have an elevated blood pressure requiring antihypertensive medications. These worrisome symptoms, enlarging neck mass, and a family history of neck tumors raised concern for a possible neck paraganglioma, and he was referred to the National Institutes of HEAD & NECK—DOI 10.1002/HED DECEMBER 2015 E205 NEYCHEV ET AL. Health Clinical Center for further workup and management. Physical examination revealed global developmental delay with body weight 49.9 kg (17th percentile) and height 152.5 cm (first percentile). His blood pressure was 105/55 mm Hg with a heart rate of 64 beats per minute. Examination of the neck revealed marked asymmetry with a prominent, firm, mildly tender, right neck mass extending behind the right ear and causing midline shift with tracheal deviation. Examination of the oral cavity revealed that the tumor was obscuring the posterior oropharynx and displacing the right pharyngopalatine arch and tonsil. Cranial nerves II to XII were grossly intact. The abdomen was unremarkable as was the remainder of his physical examination. Laboratory workup was significant for an elevated chromogranin A of 796 ng/mL (normal, <96 ng/mL) and plasma norepinephrine of 2514 pg/mL (normal, 84–794 pg/mL), elevated total urinary metanephrines 4278 mcg/ 24h (normal, 120–603 mcg/24h), normetanephrine 4218 (normal, 91–456 mcg/24h), dopamine 445 mcg/24h (normal, 65–400mcg/24 h), and norepinephrine 555mcg/24h (normal, 15–80 mcg/24h), and iron deficiency microcytic anemia with a hemoglobin level of 8.6 g/dL (normal, 13.7–17.5 g/dL). Genetic testing of peripheral blood DNA showed a G725A missense mutation in exon 7 of the SDHB gene. Anatomic imaging, including CT and MRI, revealed a large, heterogeneously enhancing, hypervascular 8.8- 3 6.6- 3 4.1-cm right neck mass encasing the right common carotid artery proximally and the internal and external carotid branches distally (Shamblin class III) without significant arterial narrowing (Figure 1A and 1B). There was complete compression of the right internal jugular vein and the mass extended medially displacing and significantly narrowing the oropharynx and proximal esophagus. There was also a 3- 3 3- 3 3.6-cm left para-aortic mass and multiple skeletal lesions, including the proximal femur, pelvis, and the entire vertebral column. Functional imaging with 18F-fluorodeoxyglucose positron emission tomography (18F-fluorodeoxyglucose-PET) and 18F-6-Lfluorodopa PET (18F-DOPA-PET) showed uptake in the neck and retroperitoneum, and bony skeleton consistent with metastatic disease (Figure 1C and 1D). The management strategy was outlined after a multidisciplinary discussion of the case, including endocrinology, endocrine surgery, cardiology, hematology, medical oncology, otolaryngology, interventional radiology, and anesthesiology. A decision was made to resect the right neck mass for palliation of the compressive symptoms after preoperative clinical optimization was completed. One month before the planned operation, the patient was started on an a-blocker (phenoxybenzamine) for preoperative blood pressure control and a blockade. The mother was given instructions to keep the patient well hydrated, and a bblocker (atenolol) was initiated once sufficient a-blockade and intravascular volume were insured. His calorie, protein, and vitamin intake in the perioperative period were closely followed by a nutritionist. In addition, more than a month before surgery, iron supplementation was implemented. Preoperative evaluation by otolaryngology and anesthesiology deemed oral intubation with the aid of a E206 HEAD & NECK—DOI 10.1002/HED DECEMBER 2015 FIGURE 1. Anatomic and functional imaging. (A) Large right neck mass obstructing the oropharynx; (B) postoperative resolution of the oropharyngeal obstruction; (C) 18F-fluorodeoxyglucose positron emission tomography (18F-fluorodeoxyglucose-PET) showing metabolically active right neck and retroperitoneal paragangliomas with multiple skeletal metastases; (D) 18F-6-L-fluorodopa PET (18F-DOPA-PET) revealing FDOPA uptake by the right neck and left para-aortic masses and the bony skeleton metastases. glide scope was feasible; however, nasal intubation and/or tracheostomy were also considered as there was concern for an impending airway emergency intraoperatively. Before the surgery, the patient was taken to interventional radiology for right carotid artery balloon occlusion testing and coil embolization of the tumor. The 20-minute occlusion test revealed adequate collateral flow from the left to right cerebral circulation and elicited no neurological symptoms (Figure 2A). These findings made the loss of the right carotid artery and its branches possible in case the dissection of the tumor from the carotid artery during surgery was not possible. There was a dramatic shrinkage of the tumor immediately after embolization (Figure 2B and 2C). He then underwent resection through a 5-cm oblique incision 1 cm below the angle of the mandible. Because of the complete encasement and invasion of the right common carotid artery and internal jugular vein, both of these structures were resected en bloc with the tumor. He was hemodynamically stable throughout the procedure, and there was 150 mL of blood loss. By postoperative day 1, his clinical status and compressive symptoms had already improved significantly. He was able to tolerate a regular diet and other symptoms, such as headaches and anxiousness, had resolved. He was successfully taken off of all antihypertensive medication and did not require the use of a continuous positive airway MANAGEMENT OF METASTATIC PARAGANGLIOMA FIGURE 2. Cerebral and neck angiograms. (A) Occlusion of the right common carotid artery revealing retrograde flow from the left cerebral circulation; (B) highly vascular paraganglioma at the carotid bifurcation; (C) preoperative coil embolization of the mass resulting in a significant decrease of tumor blood supply. pressure machine. He recovered well from his operation and was discharged home on postoperative day 3 without complication. However, on postoperative day 4, he collapsed in his bathroom at home with left hemiparesis. He was taken to a local hospital and was diagnosed with an embolic stroke. As he had just undergone surgery, tissue plasminogen activator treatment was not administered, but he was placed on aspirin. Twenty-four hours after onset of this acute cerebrovascular event, he had spontaneously recovered almost 100% of his motor function. He was discharged home on postoperative day 6 with instructions to continue his daily aspirin. At follow-up 3 weeks after surgery, he had no evidence of local compressive symptoms or neurological dysfunction. MRI of the neck showed resolution of the mass effect and a patent oropharynx (Figure 1B). One year after surgery, he is doing very well at school and continues to be free of local or systemic symptoms. DISCUSSION Our understanding of the pathophysiology and genetics of paragangliomas have improved significantly; however, their rarity and variable clinical features continue to present a considerable diagnostic and management challenge. These tumors may occur sporadically or as part of hereditary syndromes. Genotype-phenotype correlation may differ considerably depending on the underlying genetic mutation.3,4 Patients with mutations in the SDHB gene tend to present at a younger age and are prone to develop particularly severe phenotype with multifocal, usually large, paragangliomas with high metastatic potential.5–7 These slow-growing tumors can originate from both the sympathetic and parasympathetic ganglia and can be biochemically and clinically silent until a significant tumor bulk and metastases develop resulting in excess catecholamine secretion. Because of this indolent growth and insidious biochemical behavior, these tumors usually present in an advanced stage with widespread metastatic disease. This was the case with our patient who sought medical attention when systemic and local compressive symptoms from advanced metastatic disease developed. There are considerable controversy and limited data on the optimal management of head and neck paragangliomas.8 Although surgical resection has been recommended as the treatment of choice for early-stage localized disease, the treatment options for patients with locally advanced and widely metastatic tumors (especially those harboring an SDHB mutation) are limited, and the optimal management strategy has not been established.9,10 Nevertheless, several medical and surgical approaches have been proposed for patients with advanced disease including cytoreductive surgery for functional tumors, radiotherapy for local control, systemic chemotherapy with cyclophosphamide, vincristine and doxorubicin, 131iodine-labeled meta-iodobenzylguanidine therapy, radiofrequency ablation therapy, and or tumor embolization. However, any form of local or systemic therapy has side effects that may exceed the potential benefit of therapy and can carry a significant risk of massive catecholamine secretion and hypertensive crisis.9 For patients with progressive, bulky disease in the neck area that requires palliation of imminent life-threatening complications from local compression, a multidisciplinary approach addressing all aspects of advanced metastatic disease must be undertaken and directed toward optimizing the patient’s clinical status for cytoreductive resection. The surgical resection of advanced, highly vascular, large tumors in a critical anatomic location, such as the neck, is complex, technically challenging, and carries a high risk of postoperative complications, including cranial nerve dysfunction, tracheoesophageal injury, and stroke. Preoperative assessment of the patency of circle of Willis and embolization of the main arterial supply of the carotid body tumor within 48 hours of surgery (in an adequately blocked patient) may help to reduce tumor size, bleeding, and other complications associated with surgery. Our patient underwent balloon occlusion testing with tumor embolization, which resulted in significant tumor shrinkage, easier dissection, and less blood loss in what could have been a much more difficult or impossible operation otherwise. As shown in our case, a patent circle of Willis with good retrograde cerebral circulation HEAD & NECK—DOI 10.1002/HED DECEMBER 2015 E207 NEYCHEV ET AL. on preoperative balloon occlusion testing makes the loss of the carotid artery encased by the tumor possible, but it does not prevent all potential complications. Physicians should still be aware that patients may experience transient ischemic attack or stroke postoperatively. Although there is no evidence of survival benefit for the palliative surgical resection of metastatic paragangliomas, in the patient described, it resulted in an immediate improvement of compressive symptoms, may reduce hormone secretion, and can improve the response to subsequent therapies and the ability to tolerate the side effects.9,11,12 While some may say that putting a patient through a difficult and potentially morbid palliative surgery without survival benefit is not warranted, it is hard to argue that a well-planned, multidisciplinary surgical approach can result in an instant and durable improvement of the patient’s quality of life, as shown in our case. REFERENCES 1. Kantorovich V, Pacak K. Pheochromocytoma and paraganglioma. Prog Brain Res 2010;182:343–373. 2. Kantorovich V, King KS, Pacak K. SDH-related pheochromocytoma and paraganglioma. Best Pract Res Clin Endocrinol Metab 2010;24:415– 424. E208 HEAD & NECK—DOI 10.1002/HED DECEMBER 2015 3. Sethi RV, Sethi RK, Herr MW, Deschler DG. Malignant head and neck paragangliomas: treatment efficacy and prognostic indicators. Am J Otolaryngol 2013;34:431–438. 4. Neumann HP, Pawlu C, Peczkowska M, et al. Distinct clinical features of paraganglioma syndromes associated with SDHB and SDHD gene mutations. JAMA 2004;292:943–951. 5. Timmers HJ, Kozupa A, Eisenhofer G, et al. Clinical presentations, biochemical phenotypes, and genotype-phenotype correlations in patients with succinate dehydrogenase subunit B-associated pheochromocytomas and paragangliomas. J Clin Endocrinol Metab 2007;92:779–786. 6. Burnichon N, Rohmer V, Amar L, et al. The succinate dehydrogenase genetic testing in a large prospective series of patients with paragangliomas. J Clin Endocrinol Metab 2009;94:2817–2827. 7. Venkatesan AM, Trivedi H, Adams KT, Kebebew E, Pacak K, Hughes MS. Comparison of clinical and imaging features in succinate dehydrogenasepositive versus sporadic paragangliomas. Surgery 2011;150:1186–1193. 8. Ellis RJ, Patel D, Prodanov T, Nilubol N, Pacak K, Kebebew E. The presence of SDHB mutations should modify surgical indications for carotid body paragangliomas. Ann Surg 2014;260:158–162. 9. Ta€ıeb D, Kaliski A, Boedeker CC, et al. Current approaches and recent developments in the management of head and neck paragangliomas. Endocr Rev 2014;35:795–819. 10. Chen H, Sippel RS, O’Dorisio MS, et al. The North American Neuroendocrine Tumor Society consensus guideline for the diagnosis and management of neuroendocrine tumors: pheochromocytoma, paraganglioma, and medullary thyroid cancer. Pancreas 2010;39:775–783. 11. Andersen KF, Altaf R, Krarup–Hansen A, et al. Malignant pheochromocytomas and paragangliomas – the importance of a multidisciplinary approach. Cancer Treat Rev 2011;37:111–119. 12. Persky MS, Setton A, Niimi Y, Hartman J, Frank D, Berenstein A. Combined endovascular and surgical treatment of head and neck paragangliomas–a team approach. Head Neck 2002;24:423–431.