Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
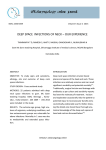
Deep Neck Infections Author: Alan D Murray, MD; Chief Editor: Arlen D Meyers, MD, MBA more... Overview Workup Treatment Updated: Mar 28, 2014 Background History of the Procedure Problem Epidemiology Etiology Pathophysiology Presentation Relevant Anatomy Contraindications Show All Multimedia Library References Background For centuries, the diagnosis and treatment of deep neck space infections have challenged physicians and surgeons. The complexity and the deep location of this region make diagnosis and treatment of infections in this area difficult. These infections remain an important health problem with significant risks of morbidity and mortality. See the image below. CT scan of the neck demonstrating left peritonsillar abscess. See 10 Patients with Neck Masses: Identifying Malignant versus Benign, a Critical Images slideshow, to help identify several types of masses. History of the Procedure In the past, infections of the deep neck spaces were associated with high rates of morbidity and mortality. The overwhelming complication rate of the past has been reduced with the advent of modern microbiology and hematology, the development of sophisticated diagnostic tools (eg, CT, MRI), the effectiveness of modern antibiotics, and the continued development of medical intensive care protocols and surgical techniques. Problem Infections of the deep neck spaces present a challenging problem for the following reasons: Complex anatomy: The anatomy of the deep neck spaces is highly complex and can make precise localization of infections in this region difficult. Deep location: The deep neck spaces are located deep within the neck. This makes diagnosis of infections difficult because they are often covered by a substantial amount of unaffected superficial soft tissue. Deep neck infections may be difficult to palpate and impossible to visualize externally. Access: Superficial tissues must be crossed to gain surgical access to the deep neck spaces, placing all of the intervening neurovascular and soft tissue structures at risk of injury. Proximity: The deep neck spaces are surrounded by a network of structures that may become involved in the inflammatory process. Neural dysfunction, vascular erosion or thrombosis, and osteomyelitis are just a few of the potential sequelae that can occur with involvement of surrounding nerves, vessels, bones, and other soft tissue. Communication: The deep neck spaces have real and potential avenues of communication with each other. Infection in one space can spread to adjacent spaces, thus gaining access to increasingly larger portions of the neck. In addition, certain deep neck spaces extend to other portions of the body (eg, mediastinum, coccyx), placing areas outside of the head and neck at risk of involvement when these spaces are involved. Epidemiology Frequency No accurate estimate of the frequency of deep neck space infections in the United States or worldwide presently exists. However, to assume that the incidence of infection in the United States is significantly lower than that of countries in which patients do not benefit from early medical intervention is reasonable. The complication rate is also likely to be greater in areas without wide access to modern medical treatment, including antibiotics, imaging modalities, and intensive care support. Etiology Before the widespread use of antibiotics, 70% of deep neck space infections were caused by spread from tonsillar and pharyngeal infections. Today, tonsillitis remains the most common etiology of deep neck space infections in children, whereas odontogenic origin is the most common etiology in adults.[1, 2, 3, 4] Causes of deep neck infections include the following: Tonsillar and pharyngeal infections Dental infections or abscesses Oral surgical procedures or removal of suspension wires Salivary gland infection or obstruction Trauma to the oral cavity and pharynx (eg, gun shot wounds, pharynx injury caused by falls onto pencils or Popsicle sticks, esophageal lacerations from ingestion of fish bones or other sharp objects) Instrumentation, particularly from esophagoscopy or bronchoscopy Foreign body aspiration Cervical lymphadenitis Branchial cleft anomalies Thyroglossal duct cysts Thyroiditis Mastoiditis with petrous apicitis and Bezold abscess Laryngopyocele IV drug use [5] Necrosis and suppuration of a malignant cervical lymph node or mass As many as 20-50% of deep neck infections have no identifiable source. Other important considerations include patients who are immunosuppressed because of human immunodeficiency virus (HIV) infection, chemotherapy, or immunosuppressant drugs for transplantation. These patients may have increased frequency of deep neck infections and atypical organisms, and they may have more frequent complications. Pathophysiology Deep neck space infections can arise from a multitude of causes. Whatever the initiating event, development of a deep neck space infection proceeds by one of several paths, as follows: Spread of infection can be from the oral cavity, face, or superficial neck to the deep neck space via the lymphatic system. Lymphadenopathy may lead to suppuration and finally focal abscess formation. Infection can spread among the deep neck spaces by the paths of communication between spaces. Direct infection may occur by penetrating trauma. Once initiated, a deep neck infection can progress to inflammation and phlegmon or to fulminant abscess with a purulent fluid collection. This distinction is important because the treatment of these 2 entities is very different. The signs and symptoms of a deep neck abscess develop because of the following: Mass effect of inflamed tissue or abscess cavity on surrounding structures Direct involvement of surrounding structures with the infectious process For example, tonsillitis may lead to peritonsillar abscess. If not treated successfully, peritonsillar abscess may spread to the lateral pharyngeal space. From there, infection spreads to the posterior pharyngeal and prevertebral spaces and into the chest. Mediastinitis and empyema may ensue, leading to death. Alternatively, infection may spread from the lateral pharyngeal space to the contents of the carotid sheath, leading to internal jugular vein thrombosis, subacute bacterial endocarditis, pulmonary emboli, carotid artery thrombosis and cerebrovascular insufficiency, or Horner syndrome. Lateral pharyngeal space abscess alone may cause airway obstruction at the level of the pharynx. Ungkanont et al reviewed 117 children treated for deep neck infections during a 6-year period.[6] The following distribution results were revealed: Peritonsillar infections (49%) Retropharyngeal infections (22%) Submandibular infections (14%) Buccal infections (11%) Parapharyngeal space infections (2%) Canine space infections (2%) The microbiology of deep neck infections usually reveals mixed aerobic and anaerobic organisms, often with a predominance of oral flora. Both gram-positive and gram-negative organisms may be cultured. Group A beta-hemolytic streptococcal species (Streptococcus pyogenes), alpha-hemolytic streptococcal species (Streptococcus viridans, Streptococcus pneumoniae), Staphylococcus aureus, Fusobacterium nucleatum, Bacteroides melaninogenicus, Bacteroides oralis, and Spirochaeta, Peptostreptococcus, and Neisseria species often are found together in various combinations. Pseudomonas species, Escherichia coli, and Haemophilus influenzae are occasionally encountered. A study by Asmar of retropharyngeal abscess microbiology demonstrated polymicrobial culture results in almost 90% of patients.[7] Aerobes were found in all cultures, and anaerobes were found in more than 50% of patients. Other studies have shown an average of at least 5 isolates from cultures. May et al found evidence that biofilm phenotypes may be associated with the pathogenesis of deep neck infections, as well as with the recalcitrance to treatment experienced with larger deep neck abscesses. The investigators obtained biopsy samples from abscess walls located in the deep neck spaces of 14 patients undergoing surgical drainage. Scanning electron microscopy revealed that 12 of the 14 tissue samples contained biofilm imbedded with rod- and cocci-shaped bacteria.[8] Presentation Obtain a detailed history from patients in whom deep neck space infection is suspected. Eliciting a history of the following is important: Pain Recent dental procedures Upper respiratory tract infections (URTIs) Neck or oral cavity trauma Respiratory difficulties Dysphagia Immunosuppression or immunocompromised status Rate of onset Duration of symptoms Physical examination should focus on determining the location of the infection, the deep neck spaces involved, and any potential functional compromise or complications that may be developing. A comprehensive head and neck examination should be performed, including examination of the dentition and tonsils. The most consistent signs of a deep neck space infection are fever, elevated WBC count, and tenderness. Other signs and symptoms largely depend on the particular spaces involved and include the following: Asymmetry of the neck and associated neck masses or lymphadenopathy, which is present in almost 70% of pediatric retropharyngeal abscesses according to a study by Thompson and colleagues Medial displacement of the lateral pharyngeal wall and tonsil caused by parapharyngeal space involvement Trismus caused by inflammation of the pterygoid muscles Torticollis and decreased range of motion of the neck caused by inflammation of the paraspinal muscles Fluctuance that may not be palpable because of the deep location and the extensive overlying soft tissue and muscles (eg, sternocleidomastoid muscle) Possible neural deficits, particularly of the cranial nerves (eg, hoarseness from true vocal cord paralysis with carotid sheath and vagal involvement), and Horner syndrome from involvement of the cervical sympathetic chain Regularly spiking fevers (may suggest internal jugular vein thrombophlebitis and septic embolization) Tachypnea and shortness of breath (may suggest pulmonary complications and warn of impending airway obstruction) Relevant Anatomy A detailed anatomic description of the major facial and deep neck spaces is beyond the scope of this article. However, a thorough knowledge of this anatomy is necessary for accurate diagnosis and treatment of these infections. The deep neck spaces are formed by fascial planes, which divide the neck into real and potential spaces. Fascial planes Two main fascial divisions exist, the superficial cervical fascia and the deep cervical fascia. Superficial cervical fascia: The superficial fascia, which lies just deep to the dermis, surrounds the muscles of facial expression. It includes the superficial musculoaponeurotic system (SMAS) and extends from the epicranium to the axillae and chest. The space deep to this layer contains fat, neurovascular bundles, and lymphatics. It does not constitute part of the deep neck space system. Deep cervical fascia: The deep cervical fascia encloses the deep neck spaces and is further divided into 3 layers, the superficial, middle, and deep layers of the deep cervical fascia. o The superficial layer of the deep cervical fascia is an investing fascia that surrounds the neck. It encompasses the sternocleidomastoid muscle, trapezius, muscles of mastication, and submandibular and parotid glands. It is limited superiorly by the nuchal ridge, mandible, zygoma, mastoid, and hyoid bones. Inferiorly, it is bounded by the clavicles, sternum, scapula, hyoid, and acromion. It contributes to the fascia covering the digastric muscle and to the lateral aspect of the carotid sheath. In its course from the hyoid bone to the medial table of the ramus of the mandible, it envelops the anterior belly of the digastric muscle and forms the floor of the submandibular space. Laterally, this fascia helps to define the parotid and masticator spaces. o The middle layer of the deep cervical fascia has 2 divisions, muscular and visceral. The muscular division surrounds the strap muscles (ie, sternohyoid, sternothyroid, thyrohyoid, omohyoid) and the adventitia of the great vessels. The visceral division surrounds the constrictor muscles of the pharynx and esophagus to create the buccopharyngeal fascia and the anterior wall of the retropharyngeal space. Both the muscular and visceral divisions contribute to the formation of the carotid sheath. The middle layer also envelops the larynx, trachea, and thyroid gland. It attaches to the base of the skull superiorly and extends inferiorly as low as the pericardium via the carotid sheath. o The deep layer of the deep cervical fascia is also subdivided into 2 divisions, prevertebral and alar. The prevertebral division adheres to the anterior aspect of the vertebral body and extends laterally to the transverse processes of the vertebrae. The alar division lies between the prevertebral division and the visceral division of the middle layer and defines the posterior border of the retropharyngeal space. It surrounds the deep neck muscles and contributes to the carotid sheath. Posteriorly, the muscular division of the middle layer of the deep cervical fascia fuses with the alar division of the deep layer of the deep cervical fascia at the level of thoracic vertebrae 1-2 (T1-T2). Deep neck spaces Within the deep neck are 11 spaces created by planes of greater and lesser resistance between the fascial layers. These spaces may be real or potential and may expand when pus separates layers of fascia. The deep neck spaces communicate with each other, forming avenues by which infections may spread. These spaces are described briefly. Parapharyngeal space o The parapharyngeal space (ie, lateral pharyngeal space, pharyngomaxillary space, pterygomaxillary space, pterygopharyngeal space) occupies an inverted pyramidal area bounded by multiple components of the fascial system. The inferior limitation of this space is the lesser cornua of the hyoid bone; the entire space is situated superiorly with respect to the hyoid. The superior margin of the space is the skull base. Its medial boundary is the visceral division of the middle layer of deep cervical fascia around the pharyngeal constrictor and the fascia of the tensor and levator muscles of the velum palatini and the styloglossus. Laterally, the space is defined by the superficial layer of the deep cervical fascia that overlies the mandible, medial pterygoids, and parotid. o The posterior border is formed by the prevertebral division of the deep layer and by the posterior aspect of the carotid sheath at the posterolateral corner. The anterior boundary is the interpterygoid fascia and the pterygomandibular raphe. The parapharyngeal space can be subdivided into compartments by a line extending from the medial aspect of the medial pterygoid plate to the styloid process. o The internal maxillary artery, inferior alveolar nerve, lingual nerve, and auriculotemporal nerve comprise the anterior (ie, prestyloid) compartment. Infections in this compartment often give significant trismus. o The posterior (ie, poststyloid) compartment contains the carotid sheath (ie, carotid artery, internal jugular vein, vagus nerve) and the glossopharyngeal and hypoglossal nerves, sympathetic chain, and lymphatics. It also contains the accessory nerve, which is somewhat protected from pathologic processes in this region by its position behind the sternocleidomastoid muscle. o The parapharyngeal space connects posteromedially with the retropharyngeal space and inferiorly with the submandibular space. Laterally, it connects with the masticator space. The carotid sheath courses through this space into the chest. This space provides a central connection for all other deep neck spaces. It is directly involved by lateral extension of peritonsillar abscesses and was the most commonly affected space before the advent of modern antibiotics. o Infections can arise from the tonsils, pharynx, dentition, salivary glands, nasal infections, or Bezold abscess (ie, mastoid abscess). o Medial displacement of the lateral pharyngeal wall and tonsil is a hallmark of a parapharyngeal space infection. Trismus, drooling, dysphagia, and odynophagia are also commonly observed. Retropharyngeal space o The retropharyngeal space is sometimes considered a third medial compartment within the parapharyngeal space because the 2 communicate laterally. This space lies between the visceral division of the middle layer of the deep cervical fascia around the pharyngeal constrictors and the alar division of the deep layer of deep cervical fascia posteriorly. It extends from the skull base to the tracheal bifurcation around T2 where the visceral and alar divisions fuse. It primarily contains retropharyngeal lymphatics. o Infection may enter this space directly, as with traumatic perforations of the posterior pharyngeal wall or esophagus, or indirectly, from the parapharyngeal space. More than 60% of retropharyngeal abscesses in children are caused by upper respiratory tract infections, whereas most infections in adults in this region are caused by trauma and foreign bodies. Other common sources of infection in the retropharyngeal space are the nose, adenoids, nasopharynx, and sinuses. o Infections of this space may drain into the prevertebral space and follow that space into the chest. Mediastinitis and empyema ensue. Abscess in this space may push forward, occluding the airway at the level of the pharynx. It may appear as anterior displacement of one or both sides of the posterior pharyngeal wall because of involvement of lymph nodes, which are distributed lateral to the midline fascial raphe. o Retropharyngeal lymph nodes tend to regress by about age 5 years, making infection in this space much more common in children than adults. Prevertebral space o The prevertebral space is located anterior to the vertebral bodies and posterior to the prevertebral division of the deep layer of the deep cervical fascia. It lies just posterior to the danger space (see below). Laterally, it is bounded by the fusion of the prevertebral fascia with the transverse processes of the vertebral bodies. It extends from the skull base to the coccyx. o The most common etiology of prevertebral abscesses (other than extension from other sites) is trauma, particularly iatrogenic instrumentation. Involvement of the vertebrae can lead to osteomyelitis and spinal instability. Danger space o The danger space is immediately posterior to the retropharyngeal space and immediately anterior to the prevertebral space, between the alar and prevertebral divisions of the deep layer of the deep cervical fascia. It extends from the skull base to the posterior mediastinum and diaphragm. Laterally, it is limited by the fusion of the alar and prevertebral division with the transverse processes of the vertebrae. Some authors consider the danger space a component of the prevertebral space. o Infections in this region may be extensions of retropharyngeal, parapharyngeal, or prevertebral infections. o Spread within the danger space tends to occur rapidly because of the loose areolar tissue that occupies this region. This spread can lead to mediastinitis, empyema, and sepsis. Masticator space o The masticator space is situated laterally to the medial pterygoid fascia and medially to the masseter muscle. It is bounded by the sphenoid bone, the posterior aspect of the mandible, and the zygomatic arch. It lies inferiorly to the temporal space and is anterolateral to the parapharyngeal space. It contains the masseter, pterygoids, ramus and body of the mandible, temporalis tendon, and the inferior alveolar vessels and nerve. o Infection in the masticator space may spread to the parapharyngeal, parotid, or temporal space. o Infections here may be a result of dental infections, particularly of the third mandibular molars, and have reportedly occurred from removal of suspension wires following reduction and fixation of facial fractures. o Trismus is commonly seen in the initial presentation and may be a long-term sequela. Submandibular space o The submandibular space is bounded inferiorly by the superficial layer of the deep cervical fascia extending from the hyoid to the mandible, laterally by the body of the mandible, and superiorly by the mucosa of the floor of mouth. o It is considered to have 2 subdivisions, the sublingual and submaxillary spaces, which are divided by the mylohyoid muscle. The sublingual space contains the sublingual gland, hypoglossal nerve, and Wharton duct. It is in continuity with the submaxillary space via the posterior margin of the mylohyoid muscle, around which pus can readily tract. The submaxillary division is further subdivided by the anterior belly of the digastric into a central submental compartment and a lateral submaxillary space. o Infection in the submandibular space may be secondary to oral trauma, submaxillary or sublingual sialadenitis, or dental abscess of mandibular teeth. o The term Ludwig angina describes inflammation and cellulitis of the submandibular space, usually starting in the submaxillary space and spreading to the sublingual space via the fascial planes, not the lymphatics. As the submandibular space is expanded by cellulitis or abscess, the floor of the mouth becomes indurated, and the tongue is forced upward and backward, causing airway obstruction. Ludwig angina does not require the presence of a focal abscess. It typically includes bilateral involvement and manifests with drooling, trismus, pain, dysphagia, submandibular mass, and dyspnea or airway compromise caused by displacement of the tongue. This is a life-threatening condition that requires tracheostomy for airway control. Before antibiotics, the mortality rate of Ludwig angina was 50%. With modern antimicrobial and surgical therapies, the mortality rate is less than 5%. o Submandibular space infections may spread to the parapharyngeal space or retropharyngeal space. Carotid space o The carotid (ie, visceral vascular) space is a potential space within the carotid sheath containing the carotid artery, internal jugular vein, vagus nerve, and sympathetic postganglionic fibers. o This space may be affected indirectly from spread of infection from the surrounding parapharyngeal space or directly by injection of drugs in those who abuse IV drugs. The resulting jugular vein thrombophlebitis sends septic emboli to the heart and lungs. The carotid artery may thrombose, form an aneurysm, or erode and rupture. Horner syndrome may occur because of involvement of the cervical sympathetics in this space. o Treatment may include anticoagulation and possibly the ligation of involved vessels. Pretracheal space o The pretracheal (ie, anterior visceral) space is enclosed by the visceral division of the middle layer of the deep cervical fascia and lies immediately anterior to the trachea. It extends from the thyroid cartilage to the superior mediastinum. o Infections here are most commonly caused by perforation of the anterior esophageal wall by endoscopic instrumentation, foreign bodies, or trauma. o Infections cause dysphagia and odynophagia, pain, fever, and possible hoarseness and airway obstruction. Peritonsillar space o This space is bounded by the tonsil medially and the superior constrictor laterally. The anterior and posterior tonsillar pillars form the remaining borders of this space. o Peritonsillar abscesses are the most common deep neck space abscess and represent a sequela of tonsillar infections. o Individuals with peritonsillar abscesses typically exhibit trismus, pain, odynophagia, drooling, a "hot potato" voice, and fever. They demonstrate uvular deviation, palatal asymmetry, and displacement of the tonsil medially. Note that the tonsillar erythema and exudates may be mild despite the presence of an abscess. o Patients who have had their tonsils removed effectively lose this space, but they can still develop peritonsillar pathology. o Peritonsillar abscesses are most commonly managed by incision and drainage or by needle aspiration. Most commonly, interval tonsillectomy is performed 4-12 weeks after resolution of the infection. o Peritonsillar abscesses may spread to the parapharyngeal space if not addressed promptly. Parotid space o The parotid space is enclosed by the superficial layer of the deep cervical fascia. This is an incomplete enclosure because the superomedial aspect of the gland is not covered. This discontinuity allows communication between the parapharyngeal space and the parotid space. o The parotid space is crossed by the external carotid artery, the posterior facial vein, and the facial nerve. o Infections in the parotid space often occur in dehydrated, debilitated patients with poor oral hygiene who develop salivary duct obstruction. o Pain, edema, and erythema in the region of the parotid are typically observed with fever. Trismus is a later finding. Temporal space o The temporal space lies between the temporalis fascia and the periosteum of the temporal bone, and it contains the internal maxillary artery and the inferior alveolar artery and nerve. The temporalis muscle effectively divides the space into a deep and superficial compartment. o Abscesses in this region are characterized by pain and trismus and may exhibit deviation of the mandible. o Incision and drainage may be accomplished by an approach 3 cm lateral to the lateral canthus or by a horizontal brow incision. Contraindications No absolute contraindications to surgical drainage of deep neck space infections exist. However, for patients experiencing airway compromise from the infection, the need to establish a safe airway takes priority and should be addressed before initiating any other surgical procedures. Once the airway has been secured, the surgical drainage procedure can be performed. References 1. Conrad DE, Parikh SR. Deep Neck Infections. Infect Disord Drug Targets. Feb 17 2012;[Medline]. 2. Chang L, Chi H, Chiu NC, Huang FY, Lee KS. Deep neck infections in different age groups of children. J Microbiol Immunol Infect. Feb 2010;43(1):47-52. [Medline]. 3. Wang LF, Tai CF, Kuo WR, Chien CY. Predisposing factors of complicated deep neck infections: 12-year experience at a single institution. J Otolaryngol Head Neck Surg. Aug 2010;39(4):335-41. [Medline]. 4. Poeschl PW, Spusta L, Russmueller G, Seemann R, Hirschl A, Poeschl E, et al. Antibiotic susceptibility and resistance of the odontogenic microbiological spectrum and its clinical impact on severe deep space head and neck infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. Aug 2010;110(2):151-6. [Medline]. 5. Daramola OO, Flanagan CE, Maisel RH, Odland RM. Diagnosis and treatment of deep neck space abscesses. Otolaryngol Head Neck Surg. Jul 2009;141(1):123-30. [Medline]. 6. Ungkanont K, Yellon RF, Weissman JL, et al. Head and neck space infections in infants and children. Otolaryngol Head Neck Surg. Mar 1995;112(3):375-82. [Medline]. 7. Asmar BI. Bacteriology of retropharyngeal abscess in children. Pediatr Infect Dis J. Aug 1990;9(8):595-7. [Medline]. 8. May JG, Shah P, Sachdeva L, et al. Potential role of biofilms in deep cervical abscess. Int J Pediatr Otorhinolaryngol. Jan 2014;78(1):10-3. [Medline]. 9. Kirse DJ, Roberson DW. Surgical management of retropharyngeal space infections in children. Laryngoscope. Aug 2001;111(8):1413-22. [Medline]. 10. Marioni G, Staffieri A, Parisi S, Marchese-Ragona R, Zuccon A, Staffieri C, et al. Rational diagnostic and therapeutic management of deep neck infections: analysis of 233 consecutive cases. Ann Otol Rhinol Laryngol. Mar 2010;119(3):181-7. [Medline]. 11. Plaza Mayor G, Martínez-San Millán J, Martínez-Vidal A. Is conservative treatment of deep neck space infections appropriate?. Head Neck. Feb 2001;23(2):126-33. [Medline]. 12. McClay JE, Murray AD, Booth T. Intravenous antibiotic therapy for deep neck abscesses defined by computed tomography. Arch Otolaryngol Head Neck Surg. Nov 2003;129(11):1207-12. [Medline]. 13. Lalakea Ml, Messner AH. Retropharyngeal abscess management in children: current practices. Otolaryngol Head Neck Surg. Oct 1999;121(4):398-405. [Medline]. 14. Cable BB, Brenner P, Bauman NM, Mair EA. Image-guided surgical drainage of medial parapharyngeal abscesses in children: a novel adjuvant to a difficult approach. Ann Otol Rhinol Laryngol. Feb 2004;113(2):115-20. [Medline]. 15. Dodds B, Maniglia AJ. Peritonsillar and neck abscesses in the pediatric age group. Laryngoscope. Sep 1988;98(9):956-9. [Medline]. 16. Huang TT, Liu TC, Chen PR. Deep neck infection: analysis of 185 cases. Head Neck. Oct 2004;26(10):854-60. [Medline]. 17. Chen MK, Wen YS, Chang CC. Deep neck infections in diabetic patients. Am J Otolaryngol. May-Jun 2000;21(3):169-73. [Medline]. 18. Staffieri C, Fasanaro E, Favaretto N, et al. Multivariate approach to investigating prognostic factors in deep neck infections. Eur Arch Otorhinolaryngol. Feb 13 2014;[Medline]. 19. Broughton RA. Nonsurgical management of deep neck infections in children. Pediatr Infect Dis J. Jan 1992;11(1):14-8. [Medline]. 20. Alexander DW, Leonard JR, Trail ML. Vascular complications of deep neck abscesses. A report of four cases. Laryngoscope. Mar 1968;78(3):361-70. [Medline]. 21. Barratt GE, Koopmann CF Jr, Coulthard SW. Retropharyngeal abscess--a ten-year experience. Laryngoscope. Apr 1984;94(4):455-63. [Medline]. 22. Brook I. Microbiology and management of peritonsillar, retropharyngeal, and parapharyngeal abscesses. J Oral Maxillofac Surg. Dec 2004;62(12):1545-50. [Medline]. 23. Cmejrek RC, Coticchia JM, Arnold JE. Presentation, diagnosis, and management of deep-neck abscesses in infants. Arch Otolaryngol Head Neck Surg. Dec 2002;128(12):1361-4. [Medline]. 24. Coller FA, Yglesias L. The relation of the spread of infection to fascial planes in the neck and thorax. Surgery. 1937;1:323-337. 25. Coticchia JM, Getnick GS, Yun RD, Arnold JE. Age-, site-, and time-specific differences in pediatric deep neck abscesses. Arch Otolaryngol Head Neck Surg. Feb 2004;130(2):201-7. [Medline]. 26. Crespo AN, Chone CT, Fonseca AS. Clinical versus computed tomography evaluation in the diagnosis and management of deep neck infection. Sao Paulo Med J. Nov 4 2004;122(6):259-63. [Medline]. 27. Forrest LA, Weed HG. Deep neck infections. In: Otolaryngology Head and Neck Surgery. Mosby-Year Book;1988:1700-1706. 28. Gianoli GJ, Espinola TE, Guarisco JL, Miller RH. Retropharyngeal space infection: changing trends. Otolaryngol Head Neck Surg. Jul 1991;105(1):92-100. [Medline]. 29. Gidley PW, Ghorayeb BY, Stiernberg CM. Contemporary management of deep neck space infections. Otolaryngol Head Neck Surg. Jan 1997;116(1):16-22. [Medline]. 30. Grodinsky M, Holyoke E. The fascia and fascial spaces of the head, neck, and adjacent regions. Am J Anat. 1938;63:367-408. 31. Hollinshead WH. Anatomy for Surgeons. Vol 2. Addison Wesley Longman;1982:269289. 32. Levitt GW. The surgical treatment of deep neck infections. Laryngoscope. Mar 1971;81(3):403-11. [Medline]. 33. Lindner HH. The anatomy of the fasciae of the face and neck with particular reference to the spread and treatment of intraoral infections (Ludwig's) that have progressed into adjacent fascial spaces. Ann Surg. Dec 1986;204(6):705-14. [Medline]. 34. Miller WD, Furst IM, Sandor GK, Keller MA. A prospective, blinded comparison of clinical examination and computed tomography in deep neck infections. Laryngoscope. Nov 1999;109(11):1873-9. [Medline]. 35. Moncada R, Warpeha R, Pickleman J, et al. Mediastinitis from odontogenic and deep cervical infection. Anatomic pathways of propagation. Chest. Apr 1978;73(4):497-500. [Medline]. 36. Pontell J, Har-El G, Lucente FE. Retropharyngeal abscess: clinical review. Ear Nose Throat J. Oct 1995;74(10):701-4. [Medline]. 37. Potter JK, Herford AS, Ellis E. Tracheotomy versus endotracheal intubation for airway management in deep neck space infections. J Oral Maxillofac Surg. Apr 2002;60(4):34954; discussion 354-5. [Medline]. 38. Ridder GJ, Eglinger CF, Technau-Ihling K, Laszig R. Deep neck abscess masquerading hypopharyngeal carcinoma. Otolaryngol Head Neck Surg. Nov 2000;123(5):659-60. [Medline]. 39. Sprinkle PM, Veltri RW, Kantor LM. Abscesses of the head and neck. Laryngoscope. Jul 1974;84(7):1142-8. [Medline]. 40. Stalfors J, Adielsson A, Ebenfelt A. Deep neck space infections remain a surgical challenge. A study of 72 patients. Acta Otolaryngol. Dec 2004;124(10):1191-6. [Medline]. 41. Suskind DL, Park J, Piccirillo JF, et al. Conscious sedation: a new approach for peritonsillar abscess drainage in the pediatric population. Arch Otolaryngol Head Neck Surg. Nov 1999;125(11):1197-200. [Medline]. 42. Tan PT, Chang LY, Huang YC. Deep neck infections in children. J Microbiol Immunol Infect. Dec 2001;34(4):287-92. [Medline]. 43. Thompson JW, Cohen SR, Reddix P. Retropharyngeal abscess in children: a retrospective and historical analysis. Laryngoscope. Jun 1988;98(6 Pt 1):589-92. [Medline]. 44. Wang LF, Kuo WR, Tsai SM, Huang KJ. Characterizations of life-threatening deep cervical space infections: a review of one hundred ninety-six cases. Am J Otolaryngol. Mar-Apr 2003;24(2):111-7. [Medline]. 45. Weber AL, Baker AS, Montgomery WW. Inflammatory lesions of the neck, including fascial spaces--evaluation by computed tomography and magnetic resonance imaging. Isr J Med Sci. Mar-Apr 1992;28(3-4):241-9. [Medline]. 46. Yusa H, Yoshida H, Ueno E. Ultrasound-guided surgical drainage of face and neck abscesses. Int J Oral Maxillofac Surg. Jun 2002;31(3):327-9. [Medline].