Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
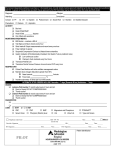
(place patient label here) Patient Name:_______________________ Order Set Directions: (√)- Check orders to a ctivate; Order s with pre-c hecked box will be fo llo we d unless lined out. Initia l each p lace in the pre-p rinted or der set where cha nges such as ad dit ions, delet ions or line o uts have been made Initia l each pa ge and Sign/Date/ Time last page PROVIDER ORDERS Diagnosis: ________________________________________________________________________________________________ Allergies with reaction type:___________________________________________________________________________________ ED Cellulitis/Skin and Skin Structure Infections Version 2 8/18/15 This order set is designed for patients that will be admitted. This order set is not intended for patients with Severe Sepsis/ Septic Shock-for these patients use the ED Sepsis order set Nursing Orders Vital signs per unit standard Vital signs non unit standard: __________ Verify that blood and wound cultures have been obtained before starting antibiotics IV/ Line Insert and/or Maintain Peripheral IV insert/maintain IV Fluids - Maintenance Sodium Chloride 0.9% IV 125 milligram/hour continuous intravenous infusion Medications Antibacterial Agents Community Onset Cellulitis/ Skin and Skin Structure Infections Benefis Community Onset Cellulitis/ Skin and Skin Structure Infections Empiric Therapy Algorithm (see attached evidence link) 95% of episodes of beta-hemolytic streptococci 5% of episodes for Staph aureus, including MRSA, but only if abscess is present First Line Treatment (No Penicillin Allergy) SELECT ALL: ampicillin-sulbactam (UNASYN) 3 gram intravenously once ; pharmacy to adjust for renal function clindamycin (CLEOCIN) 900 milligram intravenously once Penicillin Allergy Options No Cephalosporin Allergy AND No Anaphylaxis to Penicillin ceFAZolin (ANCEF) 2 gram intravenously once clindamycin (CLEOCIN) 900 milligram intravenously once SELECT ALL: Cephalosporin Allergy AND/OR Anaphylaxis to Penicillin SELECT vancomycin and clindamycin **IF vancomycin allergic SELECT one linezolid ONLY vancomycin 15 milligram/kilogram intravenously once [Max dose = 2 grams] clindamycin (CLEOCIN) 900 milligram intravenously once linezolid (ZYVOX) 600 milligram intravenously once 600 milligram tablet orally once Healthcare-associated Cellulitis/Skin and/or Skin Structure Infections Initials__________ * Page 1 of 3 (place patient label here) Patient Name: ___________________________ Order Set Directions: (√)- Check orders to a ctivate; Order s with pre-c hecked box will be fo llo we d unless lined out. Initia l each p lace in the pre-p rinted or der set where cha nges such as ad dit ions, delet ions or line o uts have been made Initia l each pa ge and Sign/Date/ Time last page PROVIDER ORDERS Benefis Healthcare Associated Cellulitis/ Skin and Skin Structure Infections Empiric Therapy Algorithm (see attached evidence link) Examples: IV site related cellulitis and surgical site infection/cellulitis Empiric coverage needed for Pseudomonas aeruginosa and MRSA First Line Treatment (No Penicillin Allergy) SELECT ZOSYN and vancomycin ** IF Vancomycin Allergic replace vancomycin with one linezolid piperacillin-tazobactam (ZOSYN) 4.5 gram intravenously once ; pharmacy to adjust for renal function vancomycin 15 milligram/kilogram intravenously once [Max dose = 2 grams] linezolid (ZYVOX) 600 milligram intravenously once 600 milligram tablet orally once Penicillin Allergy Options No Cephalosporin Allergy AND No Anaphylaxis to Penicillin: SELECT cefepime and vancomycin **IF vancomycin allergic replace vancomycin with one linezolid cefepime (MAXIPIME) 2 gram intravenously once ; pharmacy to adjust for renal function vancomycin 15 milligram/kilogram intravenously once [Max dose = 2 grams] linezolid (ZYVOX) 600 milligram intravenously once 600 milligram tablet orally once Cephalosporin Allergy AND/OR Anaphylaxis to Penicillin: SELECT aztreonam and vancomycin ** IF vancomycin allergic replace vancomycin with one linezolid aztreonam (AZACTAM) 2000 milligram intravenously once ; pharmacy to adjust for renal function vancomycin 15 milligram/kilogram intravenously once [Max dose = 2 grams] linezolid (ZYVOX) 600 milligram intravenously once 600 milligram tablet orally once Diabetes Related Foot/ Lower Extremity Infection Benefis Diabetes Related Foot/Lower Extremity Infections Empiric Therapy Algorithm (see attached evidence link) Anticipate polymicrobial mixed aerobic and anaerobic infection First Line Treatment (No Penicillin Allergy): SELECT: ampicillin-sulbactam (UNASYN) 3 gram intravenously once ; pharmacy to adjust for renal function Penicillin Allergy Options No Cephalosporin Allergy AND No Anaphylaxis to Penicillin: SELECT cefOXitin (MEFOXIN) 2 gram intravenously once Cephalosporin Allergy AND/OR Anaphylaxis to Penicillin: SELECT aztreonam and metronidazole Initials__________ Page 2 of 3 (place patient label here) Patient Name: ___________________________ Order Set Directions: (√)- Check orders to a ctivate; Order s with pre-c hecked box will be fo llo we d unless lined out. Initia l each p lace in the pre-p rinted or der set where cha nges such as ad dit ions, delet ions or line o uts have been made Initia l each pa ge and Sign/Date/ Time last page PROVIDER ORDERS and vancomycin **IF vancomycin allergic replace vancomycin with one linezolid aztreonam (AZACTAM) 2000 milligram intravenously once ; pharmacy to adjust for renal function metroNIDAZOLE (FLAGYL) 500 milligram intravenously once vancomycin 15 milligram/kilogram intravenously once [Max dose = 2 grams] linezolid (ZYVOX) 600 milligram intravenously once 600 milligram tablet orally once Laboratory Select the following only if not already done CULTURE, BLOOD x 2 from 2 different sites 5 minutes apart CULTURE, WOUND AND GRAM STAIN MIC Source: ______________________ * Provider_Signature:_____________________________________________Date:__________Time:_________ Page 3 of 3