Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
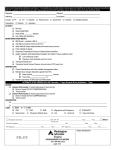
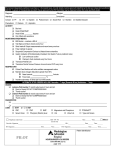
Print All &D Page &p of &P Pacemaker/ICD Postop Care General Place in Interventional Holding Place in Outpatient Extended Recovery Nonemergent procedure with continuous cardiac monitoring Discharge time: __________________________ PT. TRANSFER REQUEST ICU CVU PCU HLC Vital signs every 15 minutes for 1 hour, every 30 minutes for 1 hour, every hour for 6 hours, then every 4 hours Assessment: Risks and Safety to be completed on all patients even if currently receiving VTE prophylaxis Common Rsk Factors for VTE: Age more than 40 years old, stroke/TIA, major abdominal/pelvic/lower limb surgery, hypercoagulative state or collagen disorder, heart failure with swollen legs, malignancy, heart or respiratory failure, ICU admission, inflammatory disorder, hip, leg, or pelvic fracture, immobility more than 24 hours, chemotherapy, multiple trauma, varicose veins, prior history of VTE, central venous line/catheter, lower limb arthroplasty, obesity more than 20% over IBW, pneumonia, sepsis, pregnancy/postpartum less than 42 days, major thoracic surgery and total joints (hip and knee) VTE must be reassessed after each surgical procedure VTE Risk High risk surgery, 4060 years of age, major trauma, spinal injury, 3 or more additional risk factors present Low risk minor surgery, less than 40 years of age, patient is ambulatory, no additional risk factors present Moderate risk minor surgery, 4060 years of age, 12 additional risk factors present VTE prophylaxis not necessary, patient is low VTE risk (may not use for SCIP or Stroke patient) Individualized therapy based on the type of agent used, comorbidities, risk factors, and/or type of procedure should be used Contraindications to pharmacologic therapy Comfort care measures Medical Contraindication blood coagulation disorder, abnormal aPTT, platelets less than 50,000/dL, recent intracranial bleed, uncontrolled hypertension, active bleed, history of Heparin Induced Thrombocytopenia, untreated brain metastases Surgical Contraindication spinal tap or epidural within 12 hours, head trauma, head or eye surgery less than 3 months old Patient refused Enrolled in clinical trial Contraindications for mechanical therapy Edema of leg Patient refused Comfort care measures History of lower limb amputation Dermatitis/Cellulitis Deformity of leg Peripheral vascular disease DVT of lower extremity Original: 10/2013 Revised: 5/13 Reviewed: Form #: 2.11012 &D Page &p of &P Medications (choose only one) heparin 5000 unit subcutaneously every 12 hours enoxaparin 40 milligram subcutaneously once a day 30 milligram subcutaneously once a day if creatinine clearance is less than 30 millilter/minute rivaroxaban 10 milligram orally once a day at 1800 for Knee Replacement or Arthroplasty or History of 10 milligram orally once a day at 1800 for Hip Replacement or Arthroplasty or History of _____ milligram orally once a day at 1800 for Nonvalvular A Fib or History of _____ milligram orally once a day at 1800 for Previous Treatment of VTE _____ milligram orally once a day at 1800 for Treatment of Active VTE Laboratory Anticoagulation Laboratory Support Protocol if pharmacological therapy ordered Nursing Orders Pneumatic Comp Device (foot) Both Left Right Pneumatic Comp Device (calf) Both Left Right Other Diet REGULAR DIET CONSISTENT CARBOHYDRATE DIET 23GM NA,LOW FAT,LOW CHOL DIET Other Activity Bed rest for 6 hours Elevate head of bed 45 degrees while on bed rest Sling, Apply Order operative side upper extremity in sling until morning Activity, restrictions No ROM above shoulder level to operative upper extremity for two weeks Ambulate with assistance next morning after removal of pressure dressing and sling Up ad lib Up to chair Other Original: 10/2013 Revised: 5/13 Reviewed: Form #: 2.11012 &D Page &p of &P Medications Analgesics for Pain Level 1 3 acetaminophen 650 milligram orally EVERY 4 HOURS AS NEEDED FOR PAIN 13/TEMP > 100.5F 650 milligram rectally EVERY 6 HOURS AS NEEDED FOR PAIN 13/TEMP > 100.5F acetaminophencodeine #3 1 tablet orally EVERY 4 HOURS AS NEEDED FOR PAIN SCALE 13 Analgesics for Pain Level 4 6 acetaminophen 650 milligram intravenously EVERY 4 HOURS AS NEEDED FOR PAIN SCALE 46 oxyCODONEacetaminophen 5 mg325 mg tab 1 tablet orally EVERY 4 HOURS AS NEEDED FOR PAIN SCALE 46 Analgesics for Pain Level 7 10 morphine 1 milligram intravenously EVERY 4 HOURS AS NEEDED FOR PAIN SCALE 710 2 milligram intravenously EVERY 4 HOURS AS NEEDED FOR PAIN SCALE 710 Antidotes and Rescue Agents naloxone 0.2 milligram intravenously EVERY 2 MINUTES AS NEEDED FOR OPIATE REVERSAL if respiratory rate is less than 10 breaths per minute or patient is difficult to arouse Antibacterial Prophylactic Agents: Cephalosporins, 1stGeneration ceFAZolin if penicillin allergy use vancomycin and discontinue cefazolin 1 gram intravenously every 8 hours for 3 doses to be given within 24 hours of anethesia end time;if weight is less than 80 kilograms 2 gram intravenously every 8 hours for 3 doses to be given within 24 hours of anethesia end time; if weight greater than or equal to 80 kilograms and less than 120 kilograms 3 gram intravenously every 8 hours for 3 doses to be given within 24 hours of anethesia end time; if weight greater than or equal to 120 kilograms Antibacterial Prophylactic Agents: Glycopeptides vancomycin if patient has penicillin allergy 1 gram intravenously every 12 hours for 2 doses, to be given within 24 hours of anesthesia end time Antiemetics ondansetron 4 milligram intravenously EVERY 6 HOURS AS NEEDED FOR NAUSEA AND VOMITING prochlorperazine 25 milligram rectally EVERY 6 HOURS AS NEEDED FOR NAUSEA AND VOMITING if ondansetron is not effective; potentially inappropriate in patients 65 years or older Platelet Inhibitors: Salicylates aspirin 162 milligram orally once a day Other Respiratory O2 TO MAINTAIN O2 SAT @ 90% Incentive spirometry every 2 hours, while awake Original: 10/2013 Revised: 5/13 Reviewed: Form #: 2.11012 &D Page &p of &P Other Laboratory Hematology Complete blood cell count with automated white blood cell differential Fibrinogen Partial thromboplastin time (PTT), activated Prothrombin time (PT) and international normalized ratio (INR) Panels Basic metabolic panel Comprehensive metabolic panel Electrolyte panel Renal function panel Urine Studies Urinalysis (UA) with microscopy Other Diagnostic Tests Cardiology 12lead ECG stat in PACU the next day in the morning Other General Radiography PORTABLE,CHEST SINGLE VIEW stat in PACU the next day in the morning Other Consults Consult to dietitian Consult to Care Management Other Nursing Orders Assessments Assess for bleeding Cardiac monitor Contingency Notify provider if bleeding to operative site occurs, DO NOT remove dressing maintain sterility of site Interventions Wound care Do not remove pressure dressing, even if there is postoperative bleeding, and notify provider Keep incision clean and dry for next 10 days Allow steristrips to fall off on their own Other Original: 10/2013 Revised: 5/13 Reviewed: Form #: 2.11012 &D Patient/Caregiver Education Education, deepbreathing and coughing exercises Education, incentive spirometry Education, smoking cessation if patient is a smoker Education, wound care Other Original: 10/2013 Revised: 5/13 Page &p of &P Reviewed: Form #: 2.11012 Print All