Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Neonatal infection wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Sarcocystis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
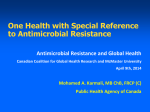
ORIGINAL ARTICLE MYCOLOGY Epidemiological study of a large cluster of fungaemia cases due to Kodamaea ohmeri in an Indian tertiary care centre A. Chakrabarti1, S. M. Rudramurthy1, P. Kale1, P. Hariprasath1, M. Dhaliwal1, S. Singhi2 and K. L. N. Rao3 1) Department of Medical Microbiology, 2) Paediatric Medicine and 3) Paediatric Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India Abstract While performing molecular confirmation of phenotypically identified Candida tropicalis isolates, we re-identified a few isolates as Kodamaea ohmeri. This led us to the present epidemiological investigation of K. ohmeri fungaemia cases. All phenotypically identified C. tropicalis blood isolates during October 2008 through to December 2009 at our advanced paediatric centre were included for molecular identification by sequencing of the internal transcribed spacer and D1/D2 regions of rDNA. After identifying a large cluster K. ohmeri fungaemia cases, a case–control study was carried out retrospectively to analyse potential risk factors for K. ohmeri fungaemia. Molecular typing of the isolates was performed using a fluorescent amplified fragment length polymorphism (FAFLP) technique. The antifungal susceptibility testing was performed as per the M27-A3 protocol of CLSI. Thirty-eight (25.7%) of 148 phenotypically identified C. tropicalis isolates were confirmed as K. ohmeri by sequencing and FAFLP. By case–control analysis, piperacillin-tazobactam was significantly associated with the K. ohmeri fungaemia. The FAFLP analysis showed that all K. ohmeri isolates had >92% similarity. The azoles and echinocandins had good in vitro activity against K. ohmeri, though 86.8% of the isolates had MIC of 1 mg/L for amphotericin B. The response to antifungal therapy could be evaluated in 27 patients and 70.4% of patients recovered after antifungal therapy. The present study reports the largest cluster of K. ohmeri fungaemia from a single centre. The study also stresses the need for accurate identification of clinical yeast isolates. Keywords: Antifungal susceptibility testing, Candida tropicalis, candidaemia, diagnosis, epidemiology, fungaemia, identification, Kodamaea ohmeri, molecular typing Original Submission: 20 March 2013; Revised Submission: 3 July 2013; Accepted: 12 July 2013 Editor: E. Roilides Article published online: 18 July 2013 Clin Microbiol Infect 2014; 20: O83–O89 10.1111/1469-0691.12337 Corresponding author: A. Chakrabarti, Department of Medical Microbiology, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, PIN 160012, India E-mail: [email protected] Introduction Nosocomial fungaemia due to Candida spp. and related yeasts has become a persistent health problem in both developed and developing countries. The incidence of fungaemia varies at 8– 10% of all nosocomial sepsis and 30–50% of these fungaemia cases occur in patients undergoing treatment in intensive care units [1–5]. The incidence and spectrum of causative agents of fungaemia varies in geographical regions. Though a higher rate of fungaemia due to non-albicans Candida species has been observed across the world, the proportion is almost 90% at certain hospitals in Asia [6–9]. While Candida glabrata and Candida parapsilosis are the leading non-albicans Candida spp. in the USA and European countries [1–5], Candida tropicalis is reported as the commonest agent in Asian countries [6–9]. The reason for the emergence of candidaemia due to C. tropicalis in Asian countries is not clear. Furthermore, large outbreaks due to unusual species like Pichia anomala, have also been reported from India [9]. While studying the molecular epidemiology of C. tropicalis candidaemia at our institute, we identified a few clinical isolates as Kodamaea ohmeri by sequencing. Those isolates had been identified earlier as C. tropicalis on the basis of phenotypic characters. Kodamaea ohmeri is a rare pathogen and the ª2013 The Authors Clinical Microbiology and Infection ª2013 European Society of Clinical Microbiology and Infectious Diseases O84 Clinical Microbiology and Infection, Volume 20 Number 2, February 2014 majority of cases are reported from Asian countries. Previously known as Pichia ohmeri and Yamadazyma ohmeri, K. ohmeri is an ascosporogenous yeast and a teleomorph of Candida guilliermondii var. membranaefaciens, belongs to the class Ascomycetes and family Saccharomycetaceae. Of the five species reported under the genus Kodamaea, only K. ohmeri has the ability to grow at 37°C. The clinical importance of other Kodamaea species (K. anthrophila, K. kakaduensis, K. laetipori K. nitidulidarum) is not known [10]. Kodamaea ohmeri is reported to cause high mortality (50%) in paediatric populations [11–21]. From our tertiary care centre with 1740 beds we report a very high incidence of fungaemia (300–500 cases every year) and C. tropicalis is the commonest isolate [8,22– 24]. However, K. ohmeri fungaemia had never been reported. We therefore planned a detailed epidemiological investigation of K. ohmeri fungaemia cases. Materials and Methods Epidemiological investigation The Postgraduate Institute of Medical Education and Research is a 1740-bed multispecialty tertiary care centre in north India with an advanced paediatric centre with 243 beds. Isolates and identification. Candida tropicalis isolates (n = 148; identified conventionally earlier by germ-tube test, urease production, morphology on corn-meal agar, and sugar fermentation and assimilation tests) from blood of patients admitted to the advanced paediatric centre from August 2008 to December 2009 were included in the study. Isolates from the hands of healthcare workers, which were collected by standard bag broth technique [9] twice (October 2008 and July 2009) from the neonatal surgical intensive care unit during the same period, were also included in the study. All 148 isolates used in the present study were re-identified by sequencing the internal transcribed spacer region and D1/D2 region of 26S ribosomal DNA [25,26]. Patients. Detailed clinical histories of patients with K. ohmeri fungaemia were retrieved from the archive and noted. Case–control study. A retrospective case–control study was performed in the neonatal surgical intensive care unit (because the maximum number of cases of K. ohmeri fungaemia was identified from this area) to determine the potential risk factors of K. ohmeri infection. Consecutive patients with K. ohmeri fungaemia (30 cases), C. tropicalis fungaemia (25 cases) and patients without fungaemia who stayed in hospital for >7 days (22 cases) during October 2008 CMI to December 2009 were studied. The last two groups served as controls. Fluorescent amplified fragment length polymorphism. Molecular typing of the K. ohmeri isolates was performed using a fluorescent amplified fragment length polymorphism (FAFLP) technique [27]. The details have been provided in the Supplementary material (Supplementary text). In short, restriction enzymes MseI and HpyCH4IV (New England Biolabs, Ipswich, MA, USA) and corresponding adapters were used. Amplification was performed using per-selective primers of HpyCH4IV (5′-GTAGACTGCGTACCCGT-3′) and MseI (5′-GATGAGTCCTGACTAA-3′). HpyCH4IV primer with one selective residue (5′-GTAGACTGCGTACCCGTC-3′), and MseI primer with two selective residues were used (5′-GATGAGTCCTGACTAACA-3′) and the primers were labelled with 6-FAM. Capillary electrophoresis of the amplified products (labelled with 6-carboxy fluorescein) and LIZ 500 (standard marker) was performed in an ABI automated DNA Sequencer 3130 (Applied Bioscience, Foster City, CA, USA). Typing data were imported to BIONUMERICS v 6.6 software (Applied Maths, Ghent, Belgium). The fingerprint curves were converted into bands and correct bands of each lane were assigned using the band position of the reference dye (LIZ500). The similarity coefficient was determined by Pearson correlation with negative similarities clip to zero. Cluster analysis was performed by Unweighted Pair Group Method with Arithmetic Mean using BIONUMERICS software. Antifungal susceptibility testing. The MICs of the K. ohmeri isolates were determined by reference microbroth dilution antifungal susceptibility testing of yeasts as per document M27-A3 of CLSI [28]. The antifungal drugs included in the study were amphotericin B (Sigma Aldrich, Bangalore, India), fluconazole (Sigma Aldrich, India), itraconazole (Janssen Research Foundation, Beerse, Belgium), voriconazole (Pfizer Central Research, Tadworth, UK), posaconazole (Merck Sharp and Dohme, Gurgaon, India) and caspofungin (Merck Sharp and Dohme, India). Statistical analysis. The results of the study for the patient and the control groups were compared by multivariate analysis test. Normalcy of the three groups was determined by Kolmogorov–Smirnov test. Variables like age, duration of hospital stay and the time after which infection occurred were described in terms of means. The non-parametric Mann– Whitney U-test was applied to compare the differences between the groups. Qualitative variables like the sex of patient, risk factors, and antibiotics and antifungals used were compared using the Pearson chi-squared test. All the statistical tests were carried out using an a error of 5% and a b error of ª2013 The Authors Clinical Microbiology and Infection ª2013 European Society of Clinical Microbiology and Infectious Diseases, CMI, 20, O83–O89 CMI Chakrabarti et al. 20%. A p value <0.05 was considered statistically significant. All analyses used SPSS (version 19.0 for Windows) software. Kodamaea ohmeri fungaemia O85 patients with K. ohmeri fungaemia were neonates and 79% (30/ 38) of them were from the neonatal surgical intensive care unit. The response to antifungal therapy could be evaluated in 27 patients, because eight patients died before the start of antifungal therapy and three patients left the hospital against medical advice. Twenty-three (85.1%) patients received fluconazole and four received caspofungin; 15 (65.2%) patients receiving fluconazole and all four patients receiving caspofungin recovered (the details of individual patients are available in the Supplementary material) (Table S2). Results Isolates and identification Of 398 culture-proven fungaemia cases that occurred during the study period of 17 months (August 2008 to December 2009) at the advanced paediatric centre, 148 isolates had been identified previously as C. tropicalis on the basis of biochemical and morphological tests. During the present study 38 (25.7%) of those 148 isolates were re-identified as K. ohmeri by genotypic characters. The K. ohmeri isolates had 98–100% identity with the sequence of standard strains (ATCC 46053, CBS 5367). The DNA sequences of the representative isolates have been deposited in the EMBL nucleotide sequence database with the Accession nos HG313954 to HG313978. Monthwise distribution of cases in pediatric ward is provided in Table S1. The details of each patient and isolate are presented in the Supplementary material (Table S2). During the same period, 47 yeasts were isolated from the hands of healthcare workers at the neonatal surgical intensive care unit and one isolate was identified as K. ohmeri (n = 1, 2%). Other yeasts were identified as: C. parapsilosis (n = 26, 55%), C. albicans (n = 8, 17%), C. glabrata (n = 5, 11%), Pichia guilliermondii (n = 3, 6%) and C. tropicalis (n = 1, 2%), Kluveromyces marxianus (n = 1, 2%), Wickeromyces anomalus (n = 1.2%), and Clavispora lusitanae (n = 1, 2%). The identity of all K. ohmeri isolates including the hand isolates was further confirmed as same species by FAFLP, because all those isolates showed a similarity coefficient of >92% [29]. Case–control study Risk factor analysis is presented in Table 1. In comparison to the C. tropicalis fungaemia, the only significant risk factor for acquiring K. ohmeri fungaemia in the hospital was piperacillin-tazobactam use (p 0.032). Whereas comparing the K. ohmeri fungaemia and non-fungaemia groups, prolonged hospital stay (p 0.037), piperacillin-tazobactam use (p 0.044), endotracheal intubation (p 0.002) and mechanical ventilation (p 0.033), were significant risk factors for the development of K. ohmeri fungaemia. Mortality was also significantly higher (50%) in K. ohmeri fungaemia patients compared with patients with C. tropicalis fungaemia (24%) or non-fungaemia (18.2%) groups. The attributable mortality in K. ohmeri fungaemia cases was 31.8%. FAFLP Thirty-eight isolates (37 from patients and one from the hands of a healthcare worker) were included for the FAFLP analysis. FAFLP profiles yielded fragments ranging from 40 to 500 bp but only fragments in the range of 50–250 bp were included for the analysis. A total of ~110 fragments were analysed. All K. ohmeri isolates had >92% similarity co-efficient. The FAFLP profile yielded eight clusters (Fig. 2). The similarity of ‘A’ ‘B’ and ‘C’ clusters was >96% with inter-cluster difference of >1%. The ‘D’, ‘E’, ‘F’ ‘G’ and ‘H’ clusters had 91–95% similarities. Except for one isolate (K5), all blood isolates from 2008 were in one cluster, including the hand isolate (cluster H). The hand isolate (isolated during October 2008) was close to two blood Patients The distribution of K. ohmeri cases during the study period is given in Fig. 1. The median age of the patients was 7 days, mean 87 days, range 1 day to 8 years with male preponderance (male : female ratio 2.4 : 1). The majority (87%) of the 6 5 Neonatal surgery Intensive care unit 4 Paediatric medicine 3 Paediatric pulmonology 2 Paediatric Intensive care unit Dec-09 Oct-09 Nov-09 Sep-09 Jul-09 Aug-09 Jun-09 Apr-09 May-09 Mar-09 Jan-09 Feb-09 Dec-08 Oct-08 Nov-08 fungaemia cases in different paediatric wards. Sep-08 0 FIG. 1. The distribution of Kodamaea ohmeri Aug-08 1 ª2013 The Authors Clinical Microbiology and Infection ª2013 European Society of Clinical Microbiology and Infectious Diseases, CMI, 20, O83–O89 O86 CMI Clinical Microbiology and Infection, Volume 20 Number 2, February 2014 TABLE 1. Evaluation of potential risk factors for Kodamaea ohmeri infection among patients of a neonatal surgical intensive care unit in a case–control study Factor analysed K. ohmeri (n = 30) No. (%) Number (%) Candida tropicalis (n = 25) No. (%) Non-candidaemia (n = 22) No. (%) K. ohmeri vs. Candida tropicalis p value K. ohmeri vs. non-candidaemia Steroid intake Prematurity Lower segment caesarean section Home delivery Intrauterine growth retardation Revised surgery Prolonged hospital stay Central line H/o Intravenous infusion in community Malnourishment Gastroenteritis Prolonged antibiotic use Piperacillin-tazobactum use Vancomycin use Urinary catheter insertion Endotracheal intubation Mechanical ventilation Total parenteral nutrition Intravenous fluid infusion Renal failure Haemodialysis Anaemia Death 10 (33.3) 6 (20) 6 (20) 4 (13.3) 0 (0) 2 (6.7) 30 (100) 11 (36.7) 0 (0) 0 (0) 2 (6.7) 26 (86.7) 5 (16.7) 14 (46.7) 23 (76.7) 20 (66.7) 14 (46.7) 1 (3.3) 30 (100) 0 (0) 0 (0) 2 (6.7) 15 (50) 9 (37.5) 4 (16) 7 (28) 7 (28) 2 (8) 2 (8.0) 24 (96.0) 12 (48) 0 (0) 2 (8.0) 0 (0) 24 (96.0) 0 (0) 7 (28.0) 17 (68.0) 11 (44) 11 (44) 0 (0) 24 (96.0) 0 (0) 0 (0) 0 (0) 6 (24) 3 (13.6) 3 (13.6) 4 (18.2) 3 (13.6) 0 (0) 3 (14.3) 19 (86.4) 6 (27.3) 1 (4.5) 6 (27.3) 1 (4.5) 20 (90.9) 0 (0) 6 (27.3) 13 (59.1) 5 (22.7) 4 (18.2) 0 (0) 22 (100) 2 (9.1) 0 (0) 0 (0) 4 (18.2) 0.750 0.702 0.487 0.176 0.115 0.850 0.269 0.396 – 0.115 0.118 0.231 0.032* 0.156 0.472 0.091 0.843 0.357 0.269 – – 0.188 0.048* 0.105 0.652 0.869 0.975 – 0.368 0.037* 0.476 0.238 0.002* 0.746 0.636 0.044* 0.156 0.175 0.002* 0.033* 0.387 – 0.092 – 0.217 0.019* *p <0.05 statistically significant with Pearson chi-squared test. isolates of 2008 (K2 and K6) with variation of <4%. The C. tropicalis isolate had only 40% similarity with K. ohmeri isolates. Antifungal susceptibility testing The in vitro activities of each antifungal agent against the K. ohmeri isolates including the range of MIC, geometric mean, MIC50 and MIC90 and cumulative percentage of the isolates inhibited at the MIC at various concentrations of antifungal agents are presented in Table 2 and Table S3. MIC90 of azoles and echinocandins were ≤0.50 mg/L. However, 33 (86.8%) isolates had MIC of 1 mg/L against amphotericin B. Only one isolate had high MICs against azoles (fluconazole MIC >64 mg/L, voriconazole 8 mg/L, itraconazole 8 mg/L, and posaconazole 4 mg/L). The response to antifungal therapy in the patient harbouring the K. ohmeri isolate with high MIC against azoles could not be evaluated because the patient left against medical advice. Discussion The present series of K. ohmeri fungaemia is the largest cluster (38 cases) of such cases from a single centre reported and the majority (78.9%) of those were reported from a neonatal surgical intensive care unit. The infection was often serious and fatal (attributable mortality 31.8%). Kodamaea ohmeri is rarely reported to cause human infection [11–21]. Before the present report, only 39 cases of K. ohmeri infection had been reported. Among them, 30 (76.9%) cases presented as bloodstream infections [11,12,16,19], and the remaining occurring as peritonitis (two cases), endocarditis (three cases), urinary tract infection (one case), polymicrobial wound infection (one case) and oral ulcer (three cases) [13,17,18,20]. The majority (75%) of those patients were immunosuppressed when they acquired the infection and had 38% mortality. Kodamaea ohmeri fungaemia may not be rare in India, as the fungus was isolated from ~1% of fungaemia cases from nine of 27 intensive care units in a recently conducted study across India (unpublished observation). A high incidence of fungaemia due to non-albicans Candida species has been reported from Asian countries including India [6–8,22–24], and C. tropicalis is reported as the commonest non-albicans Candida species in contrast to C. glabrata and C. parapsilosis in the USA and Europe[1–5]. The emergence of C. glabrata is linked to widespread use of azole antifungal agents and C. parapsilosis is linked with catheter use [1–3]. However, such an explanation could not be provided for the emergence of our C. tropicalis isolates, as the resistance to azoles in those isolates was not beyond 10% [8,22,23]. This could be a result of suboptimal infection control practices in hospitals in developing countries [30]. Similarly, the majority (97.3%) of K. ohmeri isolates in the present study had low MIC against azoles and echinocandins. To investigate the reasons for emergence we conducted a case–control analysis. Prolonged hospital stay, endotracheal intubation and mechanical ventilation were significantly associated with K. ohmeri fungaemia. These risk factors are already ª2013 The Authors Clinical Microbiology and Infection ª2013 European Society of Clinical Microbiology and Infectious Diseases, CMI, 20, O83–O89 CMI Chakrabarti et al. Kodamaea ohmeri fungaemia O87 FIG. 2. Fluorescent amplified fragment length polymorphism analysis of 38 Kodamaea ohmeri isolates. Only bands in the range of 50–250 bp are included for the analysis. The numbers indicate the isolate number, ward where it was isolated and month and year of isolation. TABLE 2. In-vitro antifungal susceptibility data (MIC, mg/L) of 38 Kodamaea ohmeri isolates against six antifungal agents Antifungal agent Range GM 50% 90% Amphotericin B Itraconazole Voriconazole Posaconazole Fluconazole Caspofungin 0.25–1 0.06–4 0.03–8 0.06–4 0.5–64 0.12–1 0.89 0.24 0.09 0.11 0.89 0.32 1 0.25 0.06 0.12 1 0.25 1 0.50 0.12 0.25 2 0.5 GM, geometric mean. known as risk factors for fungaemia [1–3]. The other common risk factors for fungaemia, such as central line and surgery, were not found to be significant in this risk factor analysis. However, while comparing commonly occurring C. tropicalis candidaemia cases, piperacillin-tazobactam use was found to be a significant risk factor for K. ohmeri fungaemia. This single risk factor could not explain the emergence of K. ohmeri fungaemia. Moreover, we did not find any change of clinical and laboratory procedures and hospital care practices during the study period. Kodamaea ohmeri is commonly used in the food industry, especially in the preparation of pickles because of its fermentation capability [10]. Though Indians are fond of pickles, they are not usually supplied in the diet of hospitalized children. Therefore, it is difficult to ascertain the actual reason for the emergence of K. ohmeri fungaemia. The patients with K. ohmeri fungaemia had significantly higher (50%) mortality than those with C. tropicalis fungaemia and than patients without fungaemia. The high mortality due to K. ohmeri infection may be related to the virulence factors of the organism, though no study has yet been conducted to confirm this. We performed molecular typing of the K. ohmeri isolates both from patients and the hand isolate. In an earlier study, pulsed-field gel electrophoresis was used to type K. ohmeri clinical isolates, which differentiated 13 isolates into six different types [11]. As amplified fragment length polymorphism is a more robust technique, we employed the fluorescence-based technique to differentiate the isolates. The resulting FAFLP pattern indicates that the majority (63.2%) of the isolates (Group A and B) had a possible clonal origin with >96% similarity. Interpretation of the ª2013 The Authors Clinical Microbiology and Infection ª2013 European Society of Clinical Microbiology and Infectious Diseases, CMI, 20, O83–O89 O88 Clinical Microbiology and Infection, Volume 20 Number 2, February 2014 FAFLP data has no clear guidelines. Savelkol et al. mentioned that patterns with 90–100% homology are considered to be derived from identical strains whereas patterns with 60–90% homology indicate different strain from the same species [29]. However, these percentages are arbitrary and may be influenced by many technical variations and imperfections. The minimal change among the isolates of 2008 and 2009 may be due to chromosomal instability or rearrangement. We could not ascertain the method of spread of the organism in our hospital because it was a retrospective study and we had only one hand isolate. Reports in the literature reveal that K. ohmeri isolates have low MIC to all antifungal agents except for a high range of MIC against fluconazole in a few isolates [11–13,21]. Similarly, all isolates in the present study, except one, had low MIC to azoles and caspofungin. However, 86.8% of our isolates had moderately high MIC (MIC 1 mg/L) to amphotericin B, in contrast to earlier reported cases [13,21]. This observation is relevant because amphotericin B deoxycholate is a commonly used systemic antifungal agent in India despite its toxicity due to low cost. One isolate (K6) with high MIC to three commonly used azoles was isolated in 2008. Fortunately that strain either did not spread or underwent loss of fitness. This high MIC isolate was closely related (99% similarity) to another isolate (K2) that had a low MIC to all the azoles tested, and was isolated from the same ward during the same period. Though echinocandins are recommended for management of candidaemia in intensive care units [31] and most (84.2%) of the patients were from ICUs in the present study, 85.1% of patients were treated with fluconazole and 65.2% of patients responded to fluconazole therapy. It is possible that clinicians prescribed fluconazole because of its low cost and that the isolates had low MICs against fluconazole. The difference in phenotypic characteristics of K. ohmeri and C. tropicalis is minimal. Inclusion of raffinose and D-xylose in the routine panel of sugars that is used in the assimilation test for yeast identification may differentiate the two species, as K. ohmeri can assimilate raffinose but not D-xylose whereas C. tropicalis can assimilate D-xylose but not raffinose (Table S4) [10]. However, the majority of laboratories in India do not perform a full battery of sugar assimilation tests when identifying Candida species. The commercial systems Vitek-2 (bioMérieux, Inc., Hazelwood, MO, USA) and API 20 (bioMérieux SA, Marcy-l’Etoile, France) may differentiate the two species. Sequencing of the internal transcribed spacer region and D1/D2 region of ribosomal DNA accurately identifies most yeast species. However, commercial systems and molecular identification are rarely employed in public sector hospitals in India because of their high cost and CMI laboratories mostly rely on restricted biochemical tests and morphological identification of yeasts. As K. ohmeri has the potential to cause outbreaks in hospitals [11], it is important to identify this fungus. In conclusion, the present study highlights the epidemiology of the largest cluster of K. ohmeri fungaemia from a tertiary care centre in Asia. The study also emphasizes the need for accurate identification of clinical yeast isolates. Funding This work was supported by the Indian Council of Medical Research (ICMR), New Delhi under the project ‘Centre of Advanced Research in Medical Mycology’. Acknowledgements We acknowledge the support of Dr Corne H Kallassen, Canisius Wilhelmina Hospital, Nijmegen, the Netherlands for his input while analysing the FAFLP results. Parts of the results were presented in IDSA 2010 and TIMM 2011. Transparency Declaration The authors have no conflicts of interest. Supporting Information Additional Supporting Information may be found in the online version of this article: Table S1. Monthwise distribution of Kodamaea ohmeri isolates at different wards in the Advanced Paediatric Centre of the Institute. Table S2. The clinical details of 38 patients with Kodamaea ohmeri fungaemia. Table S3. Minimum inhibitory concentrations (in lg/mL) of Kodamaea ohmeri isolates against different antifungal agents. Table S4. Phenotypic characters of Kodamaea ohmeri and Candida tropicalis. References 1. Pappas PG, Rex JH, Lee J et al. A prospective observational study of candidemia: epidemiology, therapy, and influences on mortality in hospitalized adult and paediatric patients. Clin Infect Dis 2003; 37: 634– 643. ª2013 The Authors Clinical Microbiology and Infection ª2013 European Society of Clinical Microbiology and Infectious Diseases, CMI, 20, O83–O89 CMI Chakrabarti et al. 2. Zaoutis TE, Argon J, Chu J, Berlin JA, Walsh TJ, Feudtner C. The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: a propensity analysis. Clin Infect Dis 2005; 41: 1232–1239. 3. Horn DL, Neofytos D, Anaissie EJ et al. Epidemiology and outcomes of candidemia in 2019 patients: data from the prospective antifungal therapy alliance registry. Clin Infect Dis 2009; 48: 1695–1703. 4. Bassetti M, Taramasso L, Nicco E, Molinari MP, Mussap M, Viscoli C. Epidemiology, species distribution, antifungal susceptibility and outcome of nosocomial candidemia in a tertiary care hospital in Italy. PLoS ONE 2011; 6: e24198. 5. Tragiannidis A, Fegeler W, Rellensmann G et al. Candidaemia in a European Paediatric University Hospital: a 10 year observational study. Clin Microbiol Infect 2012; 18: E27–E30. 6. Wu JQ, Zhu LP, Ou XT et al. Epidemiology and risk factors for non-Candida albicans candidemia in non-neutropenic patients at a Chinese teaching hospital. Med Mycol 2011; 49: 552–555. 7. Xess I, Jain N, Hasan F, Mandal P, Banerjee U. Epidemiology of candidemia in a tertiary care centre of north India: 5-year study. Infection 2007; 35: 256–259. 8. Chakrabarti A, Chatterjee SS, Rao KL et al. Recent experience with fungaemia: change in species distribution and azole resistance. Scand J Infect Dis 2009; 41: 275–284. 9. Chakrabarti A, Singh K, Narang A et al. Outbreak of Pichia anomala infection in the paediatric service of a tertiary-care centre in Northern India. J Clin Microbiol 2001; 39: 1702–1706. 10. Kurtzman CP, Fell JW, Boekhout T. The Yeasts: a taxonomic study, 5th edn. Amsterdam: Elsevier, 2011. 11. Lee JS, Shin JH, Kim MN, et al. Kodamaea ohmeri isolates from patients in a university hospital: identification, antifungal susceptibility, and pulse-field gel electrophoresis analysis. J Clin Microbiol 2007; 45: 1005–1010. 12. De Barros JD, Do Nascimento SM, De Arau′jo FJ, et al. Kodamaea (Pichia) ohmeri fungemia in a paediatric patient admitted in a public hospital. Med Mycol 2009; 47: 775–779. 13. Yang BH, Peng MY, Hou SJ, Sun JR, Lee SY, Lu JJ. Fluconazole-resistant Kodamaea ohmeri fungemia associated with cellulitis: case report and review of the literature. Int J Infect Dis 2009; 13: e493–e497. 14. Chiu CH, Wang YC, Shang ST, Chang FY. Kodamaea ohmeri fungaemia successfully treated with caspofungin. Int J Antimicrob Agents 2010; 35: 98–99. 15. Shaaban H, Choo HF, Boghossian J, Perez G. Kodamaea ohmeri fungemia in an immunocompetent patient treated with micafungin: case report and review of the literature. Mycopathologia 2010; 170: 223–228. 16. Al-Sweih N, Khan ZU, Ahmad S et al. Kodamaea ohmeri as an emerging pathogen: a case report and review of the literature. Med Mycol 2011; 49: 766–770. 17. Menon T, Herrera M, Periasamy S, Palanivelu V, Sikhamani R, Wickes B. Oral candidiasis caused by Kodamaea ohmeri in a HIV patient in Chennai, India. Mycoses 2009; 53: 458–459. Kodamaea ohmeri fungaemia O89 18. Santino I, Bono S, Borruso L et al. Kodamaea ohmeri isolate from two immunocompromised patients: first report in Italy. Mycoses 2013; 56: 179–181. 19. Janvier F, Bensalah M, Abi R, Gil C, Soler C, Merens A. Invasive infection due to Kodamaea ohmeri. Med Mal Infect 2012; 42: 527–529. 20. Sundaram PS, Bijulal S, Tharakan JA, Antony M. Kodamaea ohmeri tricuspid valve endocarditis with right ventricular inflow obstruction in a neonate with structurally normal heart. Ann Pediatr Cardiol 2011; 4: 77–80. 21. Shang ST, Lin JC, Ho SJ, Yang YS, Chang FY, Wang NC. The emerging life-threatening opportunistic fungal pathogen Kodamaea ohmeri: optimal treatment and literature review. J Microbiol Immunol Infect 2010; 43: 200–206. 22. Chakrabarti A, Ghosh A, Batra R, Kaushal A, Roy P, Singh H. Antifungal susceptibility pattern of non-albicans Candida species and distribution of species isolated from candidaemia cases over a 5-y period. Indian J Med Res 1996; 104: 171–176. 23. Chakrabarti A, Mohan B, Shrivastava SK, Marak RS, Ghosh A, Ray P. Change in distribution and antifungal susceptibility of Candida species isolated from candidaemia cases in a tertiary care centre during 1996– 2000. Indian J Med Res 2002; 116: 5–12. 24. Chakrabarti A, Rao P, Tarai B, Shivaprakash MR, Wig J. Candida in acute pancreatitis. Surg Today 2007; 37: 207–211. 25. Sugita T, Takashima M, Poonwan N, Mekha N. Candida pseudohaemulonii Sp. Nov., an Amphotericin B- and azole-Resistant yeast species, isolated from the blood of a patient from Thailand. Microbiol Immunol 2006; 50: 469–473. 26. Linton CJ, Borman AM, Cheung G et al. Molecular identification of unusual pathogenic yeast isolates by large ribosomal subunit gene sequencing: 2 years of experience at the United Kingdom mycology reference laboratory. J Clin Microbiol 2007; 45: 1152–1158. 27. Chakrabarti A, Shivaprakash MR, Curfs-Breuker I, Baghela A, Klaassen CH, Meis JF. Apophysomyces elegans: epidemiology, amplified fragment length polymorphism typing and in vitro antifungal susceptibility pattern. J Clin Microbiol 2010; 48: 4580–4585. 28. CLSI. Reference method for broth dilution antifungal susceptibility testing of yeasts; approved standard-third edition; CLSI document M27-A3. Wayne: Clinical and Laboratory Standards Institute, 2008. 29. Savelkoul PH, Aarts HJ, de Haas J et al. Amplified-fragment length polymorphism analysis: the state of an art. J Clin Microbiol 1999; 37: 3083–3091. 30. Chowdhary A, Becker K, Fegeler W et al. An outbreak of candidemia due to Candida tropicalis in a neonatal intensive care unit. Mycoses 2003; 46: 287–292. 31. Hope WW, Castagnola E, Groll AH et al. ESCMID guideline for the diagnosis and management of Candida diseases 2012: prevention and management of invasive infections in neonates and children caused by Candida spp. Clin Microbiol Infect 2012; 18(Suppl 7): 38–52. ª2013 The Authors Clinical Microbiology and Infection ª2013 European Society of Clinical Microbiology and Infectious Diseases, CMI, 20, O83–O89