Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
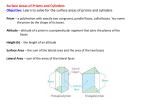
Semisolid dosage form Murat Kizaibek Ointments Ophthalmic ointments Suppository ointments Concept Ointment base Adjuvants Preparation of ointments Quality control of ointments Concept • Definition: semisolid preparations intended for external application are termed ointments. • Ingredient: drug substance +bases+ adjuvants Classification According to the dispersion system: (1) solutions type (2) suspension type (3) emulsions type (1) oleaginous dosage form (2) emulsions dosage form According to the bases: (3) pastes dosage form (4) collodions dosage form (5) ophthalmic dosage form Quality requirement the product is required smooth and uniform with certain stickiness to skin the drug in bases even distributed stability of the ointment Skin infection preparations are designed to be sterile Ointment bases Ointment bases are classified into four general groups: • (1) Hydrocarbon bases • (2) Absorption bases • (3) Water-Removable Bases • (4) Water-Soluble Bases (1) hydrocarbon bases Hydrocarbon bases (oleaginous bases) are water-free, and aqueous preparations may be incorporated into them only in small amounts and then with difficulty. Hydrocarbon bases are retained on the skin for prolonged periods, do not permit the escape of moisture from the skin to the atmosphere, and are difficult to wash off. As such they act as occlusive dressings. They do not "dry out" or change noticeably upon aging. • Petrolatum a mixture of semisolid hydrocarbons obtained from petroleum an unctuous mass, varying in color from yellow to white It may be used alone or in combination with other agents as an ointment base Commercial product is Vaseline • Paraffin A purified mixture of solid hydrocarbons obtained from petroleum. A colorless or white, more or less translucent mass that may be used to harden or stiffen oleaginous semisolid ointment bases. • Liquid paraffin • a colorless, odorless oily liquid consisting of a mixture of hydrocarbons obtained from petroleum • has the same character with paraffin • be used in combination with paraffin to adjust viscosity •Hydrophilic Petrolatum is composed of cholesterol, stearyl alcohol, white wax, and white petrolatum has the ability to absorb water, with the formation of a water-inoil emulsion. Aquaphor is a highly refined variation of Hydrophilic Petrolatum and because it can absorb up to 3 times its weight in water, it has proven useful to incorporate extemporaneously a water-soluble drug into an oleaginous base. Anhydrous Lanolin (refined wool fat) may contain no more than 0.25% of water. insoluble in water, but mixes without separation with about twice its weight of water The incorporation of water results in the formation of a water-in-oil emulsion. Lanolin (hydrous Wool Fat ) a semisolid, fatlike substance obtained from the wool of sheep. a water-in-oil emulsion that contains between 25 and 30% water. Additional water may be incorporated into lanolin by mixing. • Beeswax and spermaceti They are weak sufactants (W/O) and used as stabilization agents in O/W emulsive ointment. Mineral Oil • a mixture of liquid hydrocarbons. • It is useful as a levigating substance to wet and to incorporate solid substances into the preparation of ointments that consist of oleaginous bases as their vehicle. (2) Absorption bases Absorption bases may be of two types: (1)those that permit the incorporation of aqueous solutions, resulting in the formation of water-in-oil emulsions (e.g. Hydrophilic Petrolatum and Anhydrous lanolin) and those that are already waterin-oil emulsions (emulsion bases) that permit the incorporation of small, additional quantities of aqueous solutions (e.g. lanolin and Cold Cream). These bases are useful as emollients although they do not provide the degree of occlusion afforded by the oleaginous bases. Absorption bases are not easily removed from the skin with water washing. They are also useful pharmaceutically to incorporate aqueous solutions of drugs, e g., sodium sulfacetamide, into oleaginous bases. (3)Water-Removable Bases oil-in-water emulsions that are capable of being washed from skin or clothing with water. For this reason, they are frequently referred to as "waterwashable" ointment bases may be diluted with water or with aqueous solutions. have the ability to absorb serous discharges in dermatologic conditions. Certain medicinal agents may be better absorbed by the skin when present in a base of this type than in other types of bases. •Emulsifying agents sodium lauryl sulfate :O/W emulsion stearyl alcohol and cetyl alcohol representing the oleaginous phase of the W/O emulsion to improve the stabilization and viscosity. sodium stearate and calcium stearate. Glyceryl monostearate: weak W/O emulsifying agents and used as stabilization agents and emollient in the O/W emulsion. • Spans: W/O emulsifying agents • Tweens: O /W emulsifying agents • Peregal O and emulsive OP: O/W • Stearic acid, beewax and paraffin are the main oleaginous bases. • propylene glycol and water representing the aqueous phase • Methylparaben and propylparaben are used to preserve the ointment against microbial growth (4) Water-Soluble Bases • contain only water-soluble components. • are water washable • Because they soften greatly with the addition of water, aqueous solutions are not effectively incorporated into these bases. Rather, they are better used for the incorporation of nonaqueous or solid substances. •Polyethylene Glycol Ointment Polyethylene glycols are polymers of ethylene oxide and water The chain length may be varied to achieve polymers having desired viscosity and physical (liquid, semisolid, or solid) form. The general formula for this base calls for the combining of polyethylene glycol 3350(a solid) and polyethylene glycol 400 (a liquid) to prepare base. Adjuvants • Antioxidants • Antimicrobial preservatives •Antioxidants preparations aqueous oleaginous Antioxidants Sodium sulfite(Na2SO3) sodium bisulfite(NaHSO3), hypophosphorous acid(H3PO2) ascobic acid( vitamin C) Alpha tocopherol(vitamin E) Butylhydroxyanisole(BHA) ascorbyl palmitate •Antimicrobial preservatives frequently require the addition of chemical antimicrobial preservatives to the formulation to inhibit the growth of contaminating microorganisms These preservatives include: para-hydroxybenzoates (parabens), phenols, benzoic acid, sorbic acid, quaternary ammonium salts and other compounds. Selection of the Appropriate Base The selection of the base to use in the formulation of an ointment depends upon the careful assessment of a number of factors, including : (a) the desired release rate of the particular drug substance from the ointment base (b) the desirability for enhancement by the base of the percutaneous absorption of the drug (c) the advisability of occlusion of moisture from the skin by the base (d) the short-term and long-term stability of the drug in the ointment base (e) the influence, if any, of the drug on the consistency or other features of the ointment base. (f) patient factors also play an important role in a base's selection Preparation of Ointments Both on a large and a small scale, ointments are prepared by three general methods: (1) incorporation method (2) fusion method (3) emulsification method The method for a particular preparation depends primarily upon the nature of the ingredients (1) incorporation the components of the ointment are mixed together by various means until a uniform preparation has been attained. On a small scale, the pharmacist may mix the components of an ointment in a mortar with a pestle, or a spatula and an ointment slab (a large glass or porcelain plate) may be used to rub the ingredients together. (2) fusion By the fusion method, all or some of the components of an ointment are combined by being melted together and cooled with constant stirring until congealed. Those components not melted are generally added to the congealing mixture as it is being cooled and stirred. Naturally, heat-labile substances and any volatile components are added last when the temperature of the mixture is low enough not to cause decomposition of volatilization of the components. (3) emulsification • In the preparation of ointments having an emulsion type of formula, the general method of manufacture involves a melting process as well as an emulsification process. the water-immiscible components such as the oil and waxes are melted together in a steam bath to about 70 to 75°C Meantime, an aqueous solution of all of the heat-stable, water-soluble components is being prepared in the amount of purified water specified in the formula and heated to the same temperature as the oleaginous components. Then the aqueous solution is slowly added, with constant stirring (usually with a mechanical stirrer), to the melted oleaginous mixture, the temperature is maintained for 5 to 10 minutes to prevent crystallization of waxes the mixture is slowly cooled with the stirring continued until the mixture is congealed. Notice: • If the aqueous solution were not the same temperature as the oleaginous melt, there would be solidification of some of the waxes upon the addition of the colder aqueous solution to the melted mixture. Emulsification ointments Ⅱophthalmic ointments • Concept semisolid preparations intended for application to the eye are specially prepared and are termed ophthalmic ointments. •Preparation of ophthalmic ointments The methods of preparation just like ointments,but under the aseptic condition for prevent eye infection. •The bases must be non-irritating to the eye and must permit the diffusion of the medicinal substance throughout the secretions bathing the eye. Ointment bases utilized for ophthalmics have a melting or softening point close to body temperature. In most instances, mixtures of petrolatum and liquid petrolatum (mineral oil) are utilized as the ointment base. Sometimes a water-miscible agent as lanolin is added. This permits water and water-insoluble drugs to be retained within the delivery system. •The advantage and disadvantage The primary advantage of an ophthalmic ointment over an ophthalmic solution is the increased ocular contact time of the drug. One disadvantage to ophthalmic ointment use is the blurred vision which occurs as the ointment base melts and is spread across the lens. Suppositories 1.Definition Suppositories are semisolid dosage forms intended for insertion into body orifices where they melt, soften, or dissolve and exert localized or systemic effects. 2. Body orifices for using Suppositories are commonly employed rectally, vaginally and occasionally urethrally. They have various shapes and weights depending upon the density of the base and the medicaments present in it, and the individual manufacturer's product. Rectal using Vaginal using Shape of suppositories 3.character of action 1)Local Action Rectal suppositories are most frequently employed to relieve constipation or the pain, irritation, itching, and inflammation associated with hemorrhoids or other anorectal conditions. Vaginal suppositories or inserts are employed mainly as contraceptives, antiseptics in feminine hygiene, and as specific agents to combat an invading pathogen. Urethral suppositories may be used as antibacterial and as a local anesthetic preparative to urethral examination. 2)Systemic Action administered rectally in the form of suppositories for systemic effects include: (a) for the relief of nausea and vomiting and as a tranquilizer (b) for narcotic analgesia (c) for the relief of migraine syndrome (d) anti-inflammatory analgesic and antipyretic. 3) advantages over oral therapy (rectal route for achieving systemic effects ) (a) drugs destroyed or inactivated by the pH or enzymatic activity of the stomach or intestines need not be exposed to these destructive environments; (b) drugs irritating to the stomach may be given without causing such irritation; (c) drugs destroyed by portal circulation may bypass the liver after rectal absorption (drugs enter the portal circulation after oral administration and absorption); (d) the route is convenient for administration of drugs to adult or pediatric patients who may be unable or unwilling to swallow medication; (e) it is an effective route in the treatment of patients with vomiting episodes. 4.Quality control of suppository The shape and size of a suppository must be such that the medicaments and base mixed uniformly with certain hardness under condition of shipment and storage capable of being easily inserted into the intended body orifice without causing undue distension. once inserted, the base melts, softens, or dissolves, distributing the medicaments it carries to the tissues of the region. It must be retained for the appropriate period of time for local effects or quickly absorbed for systemic effects . Ⅱ Ingredients of suppositories contains drug,base and other adjuvant ,which the affecting factors for preparation are the physicochemical nature of the drug, the nature of the suppository vehicle and its capacity to release the drug and clinical desired effects from administration 。 Drug properties as the relative solubility of the drug in lipid and in water , the particle size of a dispersed drug. Base 1.requisites for a suppository base is that : 1)it remains solid at room temperature but softens, melts, or dissolves readily at body temperature so that the drug it contains may be made fully available soon after insertion 2)with certain hydrophilic or hydrophobic character 3)melting point near to solidifying point 4) easily ejectable from mold 5) don’t irritate to the mucous membranes 2.Classification of Suppository Bases According to bases physical characteristics the bases can be classified into (1) fatty or oleaginous bases (2)water-soluble or water-miscible bases (1) fatty or oleaginous bases: Fatty bases are perhaps the most frequently employed suppository bases . A lipophilic drug that is distributed in a fatty suppository base in low concentration has less of a tendency to escape to the surrounding aqueous fluids than would a hydrophilic substance present in a fatty base to an extent approaching its saturation. fatty bases contains: (a) Cocoa Butter and (b) compounds of glycerin (a) Cocoa Butter the fat obtained from the roasted seed of theobroma cacao. At room temperature it is a yellowish, white solid having a faint, agreeable chocolate-like odor. Chemically, it is a triglyceride (combination of glycerin and one or different fatty acids) primarily of oleopalmitostearin and oleodistearin. It melts between 30℃ to 36 ℃, an ideal suppository base, melting just below body temperature and yet maintaining its solidity at usual room temperatures. because of its triglyceride content, cocoa butter exhibits marked polymorphism, or different crystalline forms α, β,β’,γ. Because of this, when cocoa butter is hastily or carelessly melted at a temperature greatly exceeding the minimum required temperature and then quickly chilled, As a result a metastable crystalline form (α crystals) with a melting point much lower than the original cocoa butter that the cocoa butter will not solidify at room temperature. Since the form represents a metastable condition, there is a slow transition to the more stable β form of crystals having the greater stability and the higher melting point. Cocoa butter must be slowly and evenly melted. Preferably over a water bath of warm water, to avoid the formation of the unstable crystalline form and ensure the retention in the liquid of the more stable β crystals that will constitute nuclei upon which the congealing may occur during chilling of the liquid. Substances such as phenol and chloral hydrate have a tendency to lower the melting point of cocoa butter when incorporated with it. If the mp is lowered to such an extent that it is not feasible to prepare a solid suppository using cocoa butler alone as the base, solidifying agents like cetyl esters wax (about 20%) or beeswax (about 4%) may be melted with the cocoa butter to compensate for the softening effect of the added substance. However, the additions of hardening agents must not be so excessive as to prevent the melting of the base after the suppository has been inserted into the body, nor must the wax material interfere with the therapeutic agent in any way so as to alter the efficacy of the product. (b) compounds of glycerin The higher molecular weight fatty acids, such as palmitic and stearic acids, may be found in fatty suppository bases. Such compounds as glyceryl monostearate and glyceryl monopalmitate are examples of this type of agent. (2) water-soluble or water-miscible bases (a) Glycerinated gelatin This base is slower to soften and mix with the physiologic fluids , therefore provides a more prolonged release; Because it have a tendency to absorb moisture due to the hygroscopic nature of glycerin, the suppository must be protected from atmospheric moisture in order for them to maintain their shape and consistency Due also to the hygroscopicity of the glycerin, the suppository may have a dehydrating effect and be irritating to the tissues upon insertion. The water present in the formula for the suppositories minimizes this action; however, if necessary, the suppositories may be moistened with water prior to their insertion to reduce the initial tendency of the base to draw water from the mucous membranes and irritate the tissues. A glycerinated gelatin base is most frequently used in the preparation of vaginal suppositories, where the prolonged localized action of the medicinal agent is usually desired. vaginal suppositories are much more easily inserted than suppositories with a cocoa butter base, owing to the brittleness of cocoa butter and its rapid softening at body temperature. (b) Polyethylene glycols They are available in a number of molecular weight ranges, the more commonly used being polyethylene glycol 200,400, 600,1000,1500,1540, 3350, 4000,6000, and 8000. The numerical designations refer to the average molecular weights of each of the polymers. Various combinations of these polyethylene glycols may be combined by fusion, using two or more of the various types to achieve a suppository base of the desired consistency and characteristics. Polyethylene glycol suppositories do not melt at body temperature but rather dissolve slowly in the body's fluids. If the polyethylene glycol suppositories do not contain at least 20%of water to avoid the irritation of the mucous membranes after insertion, they should be dipped in water just prior to use. (c) polyoxyl 40 stearate a surface-active agent with the average polymer length being equivalent to about 40 oxyethylene units. The substance is a waxy, white to light tan solid that is water-soluble. Its melting point is generally between 39℃ and 45 ℃. Ⅲ Preparation of Suppositories Suppositories are prepared by two methods: (1) Preparation by compression (2) Fusion or preparation by mold (1) Preparation by Compression: Suppositories may be prepared by forcing the mixed mass of the suppository base and the medicaments into special molds using suppository making machines. In preparation for compression into the molds, the suppository base and the other formulative ingredients are combined by thorough mixing, the friction of the process causing the base to soften into a paste-like consistency. (a)cold Compression: The process of compression is especially suited for the making of suppositories containing medicinal substances that are heat labile and for suppositories containing a great deal of substances insoluble in the base. (b) hand rolling and shaping: With the ready availability of suppository molds of accommodating shapes and sizes, there is little requirement for today's pharmacist to shape suppositories by hand. Hand rolling and shaping is a historic part of the art of the pharmacist. (2) Fusion or preparation by mold The method is most frequently employed in the preparation of suppositories both on a small scale and on an industrial scale. Mold shape Molds in common use today are made from stainless steel. The molds, which separate into sections, generally longitudinally, are opened for cleaning before and after the preparation of a batch of suppositories. Care must be exercised in cleaning the mold for the desired smoothness of the resulting suppositories. LUBRICATION OF THE MOLD Depending upon the formulation, suppository molds may require lubrication before the melt is poured to facilitate the clean and easy removal of the molded suppositories. Lubrication is seldom necessary when the suppository base is cocoa butter or polyethylene glycol. Lubrication is usually necessary when glycerinated gelatin suppositories are prepared. Any materials which might cause irritation to the mucous membranes should not be employed as a mold lubricant. the steps in molding (a) the melting of the base (b) incorporating of any required medicaments (c) pouring the melt into molds (d) allowing the melt to cool and congeal into suppositories (e) removing the formed suppositories from the mold. Notice:Suppositories of cocoa butler, glycerinated gelatin, polyethylene glycol, and most other suppository bases are suitable for preparation by molding. pouring the melt into molds removing the formed suppositories CALIBRATION OF THE MOLD Each individual mold is capable of holding a specific volume of material in each of its openings. If the material is changed, the weight of the resulting suppositories will differ from the weight of suppositories prepared in the same mold because of the difference in the densities of the materials. Similarly, any added medicinal agent would further alter the densities of the bases, and the weights of the resulting suppositories would be different from those prepared with base material alone. It is important that the pharmacist calibrate each of his suppository molds for the suppository bases that he generally employs in order that he may prepare medicated suppositories each having the proper quantity of medicaments. First step : to prepare molded suppositories from base material alone. After removal from the mold, the suppositories are weighed, and the total weight and the average weight of each suppository are recorded as G Second step : to prepare molded suppositories from base and drug. After removal from the mold, the suppositories are weighed, and the total weight and the average weight of each suppository are recorded as M Third step : to calculate the displacement value by the equation below: W DV G (M W ) y x (G )n DV G W M G-(M-W) For example: Prepare the suppositories using cocoa buffer. The average weight of each blank suppository is 3.5g. Then adding 1.5g drugs into cocoa buffer and preparing a medicated suppository. The weight of the medicated suppository is 4.2g. Please calculate the dosage of cocoa buffer if 10 medicated suppositories, every medicated suppositories contain 1.0g drug, want to be prepared. Ⅳ Packaging and Storage Most commercially available suppositories are: individually wrapped in either foil or a plastic material. Some are packaged in a continuous strip with suppositories being separated by tearing along perforations placed between suppositories Suppositories are also commonly packaged in slide boxes or in plastic boxes. maintain in a cool place. stored in environments of fitting humidity flash1 flash2 Ⅴ Treating role and Clinical applying systemic action: medicaments may be intended to be absorbed for the exertion of systemic effects local action :medicaments may be intended for retention within the cavity for localized drug effects. Systemic Action For systemic effects, the mucous membranes of the rectum and vagina permit the absorption of many soluble drugs. Although the rectum is utilized quite frequently as the site for the systemic absorption of drugs, the vagina is not as frequently used for this purpose. Absorption route: According to the course of venous flow, a drug absorbed in the lower part of the rectum should enter the vena cava; A drug placed in the upper part of the rectum should diffuse into blood vessels which lead to the liver. Affecting factors for absorption The factors affecting the rectal absorption of a drug administered in the form of a suppository may be divided into : (1)physiologic factors: colonic contents, circulation route, and the pH and lack of buffering capacity of the rectal fluids (2) physicochemical factors of the drug and the base: The lipid-water partition coefficient;particle size; nature of the bases Glossary Ointments bases; oleaginous; hydrocarbon bases; absorption bases; water-removable bases;water-soluble bases ; Petrolatum ; Vaseline; Paraffin ; Anhydrous lanolin ; Hydrophilic; Antioxidants; incorporation method; fusion method; emulsification method; ophthalmic ointments; Suppositories; Body orifices ; Rectal; Vaginal; melting point ; Cocoa Butter ; polymorphism; hygroscopicity; Glycerinated gelatin ; Polyethylene glycols; polyoxyl 40 stearate; displacement value