Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
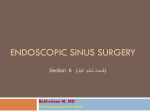
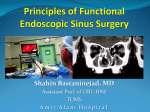
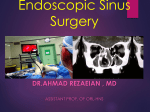
Rom J Morphol Embryol 2014, 55(3 Suppl):1099–1104 ORIGINAL PAPER RJME Romanian Journal of Morphology & Embryology http://www.rjme.ro/ The anatomo-radiological study of unusual extrasinusal pneumatizations: superior and supreme turbinate, crista galli process, uncinate process MIHAIL DAN COBZEANU1), VASILICA BÂLDEA2), MIRCEA CĂTĂLIN BÂLDEA3), PATRICIA SONIA VONICA1), BOGDAN MIHAIL COBZEANU1) 1) 2) 3) Department of Otorhinolaryngology, “Grigore T. Popa” University of Medicine and Pharmacy, Iassy, Romania Department of Otorhinolaryngology, Emergency County Hospital, Buzau, Romania Department of Oro-Maxillo-Facial Surgery, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania Abstract Introduction: One of the aspects that have an influence on rhinosinusal endoscopic surgery is extrasinusal pneumatization, which can also affect less common structures at this level. The pneumatization of the superior and supreme turbinates, uncinate process and crista galli are perfect examples of this situation. The diagnosis is made only through imaging methods. Materials and Methods: This is a retrospective anatomo-radiological study analyzing 205 CT scans of the facial sinuses performed over a three years period. All patients were symptomatic and the CT scans were performed to assess the cases prior to surgery. Ninety-seven patients were females and 108 males, aged between 18 and 91 years. Results: The prevalence of pneumatization and the prevalence of the different pneumatization types (superior and supreme turbinate, uncinate process and crista galli) were determined. Conclusions: The pneumatization of the supreme turbinate (10.24%) was less common than that of the superior turbinate (29.76%) and affected all its anatomical variations (A, B, C). Pneumatization of the crista galli process was recorded in 22.92% of the cases, especially in association with type 2, while the prevalence of pneumatized uncinate process was of only 3.41% (uni- or bilateral). Keywords: anatomo-radiological study, unusual extrasinusal pneumatization, turbinates, crista galli, uncinate process. Introduction The nasal turbinates can contain one or more aerated cells. While the pneumatization of the middle turbinate has often been described, pneumatized superior turbinates [1, 2], supreme turbinates, uncinate process and crista galli are rare [3, 4]. The superior turbinate belongs to the ethmoid bone, medially limiting the superior meatus in which the cells of the posterior ethmoid and of the sphenoid drain [5]. Usually, it is about half the length of the middle turbinate, being situated above its posterior half [6]. The ostium of the sphenoid sinus is located medially and superior to the postero-inferior portion of the superior meatus [7]. Thus, the superior turbinate serves as an essential landmark during endoscopic posterior ethmoidectomy and sphenoidectomy surgery. The superior turbinate is also known as the “forgotten turbinate” [8] as it is difficult to identify through nasal endoscopy, a preoperative CT scan being recommended. The supreme turbinate is a rare anatomic variation. It can be uni- or bilateral, sometimes pneumatized by a posterior ethmoid cell which drains into the posterior ethmoid/sphenoidal sinus, as described by Stammberger [9]. There are three types of association between the superior and supreme turbinates. Type A is the most common one, with the supreme turbinate being smaller than the superior one. Type B (superior and supreme turbinate have the same size) and type C (supreme turbinate larger than the superior one) are rare. The ISSN (print) 1220–0522 supreme meatus is located on the infero-lateral side of the supreme turbinate and contains the ostium of a posterior ethmoidal cell [3, 4, 10, 11]. The uncinate process is a thin ethmoid bone plate, which fuses inferiorly with the ethmoid process of the inferior nasal turbinate [12]. It is a key structure of the ethmoid bone and forms the semilunar hiatus at the level of the lateral nasal wall. Its pneumatization is a rare abnormality. The uncinate process occupies the free infundibular zones and may generate areas of mucosal contrast [13]. The prevalence of this anatomic variation is estimated between 0.4–13% by different authors [14–17]. The crista galli is an endoscopic surgical landmark in frontal sinus approach and pituitary surgery. It can be pneumatized resulting in a small-aired sinus with no clinical echo. The excessive pneumatization can lead to ENT-related headache or may be the origin of neurological symptoms with frontal lobe implications [3, 4]. When pneumatization is associated with congenital malformations involving midline defects (meningocele or defective embryological development of the ectoderm near crista galli), the clinical manifestations become obvious [18]. The study purpose was to determine the general prevalence and that of the less common types of extrasinusal pneumatization: superior nasal turbinate, supreme nasal turbinate, uncinate process, crista galli, and if their different associations vary with age, gender, chronic recurrent rhinosinusitis. ISSN (on-line) 2066–8279 1100 Mihail Dan Cobzeanu et al. Materials and Methods We retrospectively investigated the preoperative CT scans performed in the Iassy and Buzău (Romania) outpatient or emergency departments, in the interval January 2008–June 2010, in 205 patients with ENTrelated symptoms. The subjects were aged 18–91 years, 97 females (47.32%) and 108 males (52.68%); informed consent was obtained. The results refer to ENT symptomatic patients and not general population. Spiral tomography technique was used to expose the facial sinuses for better image accuracy, allowing complex bone reconstruction. Pneumatization of every air cell found at this level was considered, no matter its size or location. Table 1 – Estimated parameters in patients vs. presence of superior turbinate pneumatization (df=1) χ 2 2 0.4273801 Pearson’s Correlation factor (Spearman’s rank r) 0.0995907 p (95% CI) 0.51328 0.51564 Figures 3–6 present the different types of superior turbinate pneumatization according to extension, localization and drainage type. Results Superior turbinate pneumatization Superior turbinate pneumatization was identified in 61 subjects, the prevalence being 29.76% (61/205). Thirty (27.78%) were men and 31 (31.96%) women (Figure 1). Thirty-six (17.56%) were bilateral, 25 (12.2%) unilateral, 14 (6.83%) left and 11 (5.37%) right (Figure 2). Figure 3 – CT scan of the paranasal sinuses, coronal reconstructions. Bilateral superior turbinate pneumatization: 1. Small size pneumatization without rhinosinusitis; 2. Hyperpneumatization with left mucocele. Figure 4 – CT scan of the paranasal sinuses, coronal and axial slices. Bilateral superior turbinate pneumatization: 1. Coronal section; 2. Axial section; 3. Bilateral pneumatized superior turbinate drainage on the sphenoid sinus. Figure 1 – Gender distribution of cases by the presence/ absence of superior turbinate pneumatization. Figure 5 – CT scan of the paranasal sinuses, coronal sections. Anatomic variations of superior turbinate pneumatization: 1. Left superior turbinate pneumatization with uncinate process insertion and right pneumatization of the superior turbinate; 2. Right superior turbinate pneumatization, type C; 3. Left superior turbinate pneumatization with drainage on the suprabullar recess. Figure 2 – Distribution of cases by superior turbinate pneumatization type. Statistical results (Table 1) show that in our patients there was no significant association between gender and superior turbinate pneumatization (χ2=0.427, p=0.51328, 95% CI). Figure 6 – CT scan of the paranasal sinuses. Pneumatization of the left superior turbinate revealed by all types of sections: 1. Coronal slice: hyperpneumatization with septum and uncinate process mucosal contact; 2. Sagittal section: the pneumatization of the posterior part of the superior turbinate and association with left unpneumatized supreme turbinate; 3. Axial section: the left superior turbinate pneumatization. The anatomo-radiological study of unusual extrasinusal pneumatizations: superior and supreme turbinate… Superior turbinate is best studied on coronal sections, but it also can be identified on axial and sagittal sections as in Figure 6. Supreme turbinate pneumatization Supreme turbinate was identified in 61/205 cases, prevalence of 29.76%, of which 43 (20.97%) were bilateral and 18 (8.78%) unilateral. Its pneumatization was found in 21/205 (10.24%) subjects. Of these, 10/205 (4.88%) were bilateral and 11/205 (5.37%) unilateral, six (2.93%) left and five (2.44%) right (Figure 7). 1101 four (1.95%) men and three (1.46%) women. Bilateral uncinate process pneumatization was present in 3/205 (1.46%) subjects, and unilateral in 4/205 (1.95%) (Figure 10). All cases of unilateral uncinate process pneumatization where found only on the left side. The mean age of patients with this anatomical variation was 45.67±26.39 years [3, 4]. Figure 10 – Uncinate process pneumatization. Figures 11–13 show various types of pneumatized uncinate processes. Figure 7 – Supreme turbinate pneumatization. Figures 8 and 9 present different imaging appearances of supreme turbinate pneumatization variations depending on location, extension or drainage. Figure 8 – CT scan of the paranasal sinuses. Anatomic variations of supreme turbinate pneumatizations: 1. Right pneumatization type C; 2. Left pneumatization type C; 3. Bilateral pnematization type C, with left drainage on the sphenoid sinus; 4. Left pneumatization type A associated with lamelar pneumatzation of ipsilateral superior turbinate. Figure 11 – CT scan of the paranasal sinuses, coronal sections: 1. Bilateral uncinate proces pneumatization with pathological process on the left; 2. Left uncinate process pneumatization associated with right uncinate medialization. Figure 12 – CT scan of the paranasal sinuses, coronal section: 1. Bilateral uncinate process pneumatization. Figure 9 – CT scan of the paranasal sinuses, sagittal reconstructions, successive sections: 1. Superior turbinate pneumatization; 2. Supreme turbinate pneumatization. Uncinate process pneumatization Uncinate process pneumatization (uncinate bulla) is one of the anatomical variations of this surgical landmark, possibly associated with diminished sinus ventilation, especially of the frontal recess, anterior ethmoid, ethmoidal infundibulum region. We identified 7/205 (3.41%) cases, Figure 13 – CT scan of the paranasal sinuses, axial sections: 1. Left uncinate process pneumatization associated with type 5 ipsilateral septal deviation (Mladina classification); 2. Left uncinate process pneumatization associated with ipsilateral concha bullosa. 1102 Mihail Dan Cobzeanu et al. Crista galli pneumatization We first identified the three types of crista galli according to their location to the ethmoidal lamina cribriformis, finding the following prevalences: type I – crista galli situated entirely above the lamina cribriformis, 48/205 (23.41%) cases; type II – crista galli situated less than 1/2 of its height under the lamina cribriformis, 127/205 (61.65%) cases; type III – crista galli situated more than 1/2 of its height under the lamina cribriformis, 30/205 (14.64%) cases [4]. Pneumatization was found in all types of crista galli, but in different proportions: pneumatized type I – 9/205 (4.39%) cases; pneumatized type II – 27/205 (13.17%) cases; pneumatized type III – 11/205 (5.36%) cases [4]. The prevalence of crista galli, both in pneumatized and unpneumatized forms are presented in Figure 14. Figure 14 – Distribution of cases by crista galli pneumatization type. Figures 15–17 present different imaging appearances of variations of crista galli. Figure 17 – CT of the paranasal sinuses, coronal reconstructions. Crista galli pneumatization: 1. Type II with symmetric ethmoid roof; 2. Type I associated with superior turbinate pneumatization; 3. Type III. Dotted line: cribriform plate of the ethmoid bone. Discussion Superior turbinate pneumatization In the few published studies on superior turbinate pneumatization the prevalence is different probably because of the different evaluation methods. The highest prevalence is reported by direct visualization in cadaver studies. Van Alyea studied the ethmoid labirinth of 100 cadavers finding pneumatization in 57% (the highest value), unrelated to rhinosinusitis [19]. This relationship was reported by other authors following endoscopic studies. In 1991, Stammberger found rhinosinusitis and significant superior turbinate pneumatization in a small group of patients, all with indication for functional endoscopic sinus surgery (FESS) [9]. He also described a bilateral pneumatization extending between the middle turbinate and the nasal septum causing mucosal contact and thus causing headache and hyposmia or anosmia by olfactive fossa block. In 1996, Clerico reported three cases of extensive superior turbinate pneumatization with severe migraines not responding to usual medication [8]. Turbinate pneumatization is still a rare cause of headache [1, 10], this being also supported by our research (Figure 5). CT imaging studies [20] for rhinosinusitis found a prevalence of 48% for the superior turbinate pneumatization (27% unilateral and 21% bilateral), comparable to that found by Van Alyea in cadaver studies (57%). In our radio-anatomical research, the prevalence was 29.75% (61/205 cases), lower than in the two previous studies by Van Alyea [19] or Ariyürek et al. [20], with similar prevalence for bilateral and unilateral cases. The superior turbinate is a constant landmark for identifying both the sphenoethmoid recess and the superior resection border of the natural sphenoid ostium [21]. Supreme turbinate pneumatization Figure 15 – CT scan of sinuses, axial slice (1) and coronal reconstructions (2 and 3). Unpneumatized crista galli types: 1. Type I; 2. Type II; 3. Type III. Figure 16 – CT scan of sinuses, axial (1 and 2) and coronal (3) sections. Crista galli pneumatization: 1. Type I; 2. Drainage of the partial pneumatized crista galli type I on the frontal sinus; type II associated with ethmoidal roof asymmetry. When it exists, the supreme turbinate serves as a surgical landmark for the posterior ethmoid and sphenoid approach [22–24]. It is less used as a landmark than the superior turbinate, because it is inconstant. The inferior supreme turbinate attachment is lateral to the sphenoid ostium. Usually the ostium is identified between the inferior attachment of supreme turbinate situated laterally and nasal septum medially. The sphenoid ostium has a round or oval shape. The opening of the sphenoid ostium can be hidden by the medial part of supreme turbinate, which is bent downwards [25]. The sphenoid ostium is located on the anterior wall of sphenoid sinus, 1.5 cm above the floor; the optic nerve and internal carotid artery can often lie on the lateral sides of the sinus [26]. The anatomo-radiological study of unusual extrasinusal pneumatizations: superior and supreme turbinate… Orhan et al. [27] developed a study based on microscopy of 20 adult cadavers for the anatomical variants of superior and supreme turbinates. They found a prevalence of 60% for the supreme turbinate (the highest value reported) and described the types. The radio-anatomical studies report a lower prevalence for supreme turbinate than direct microscopic visualization studies. Orhan et al. [27] found 58% prevalence for type A and 41.7% for type B and type C. In types B and C, the supreme turbinate can easily be damaged being similar to other structures and difficult to recognize, in those cases causing hyposmia or anosmia. In our study using imaging material, we obtained a prevalence of the supreme turbinate of only 29.75% because the small turbinates (less than 2 mm) were ignored. Bilateral forms were predominant, 60.65% of the supreme turbinates presenting pneumatization. Uncinate process pneumatization Pneumatized uncinate process (uncinate bulla), as one of the variants of uncinate process that favor an inflammatory pathology or increase the surgical risk (difficult orientation during uncinectomy) can decrease sinus ventilation [28]. Imaging studies reveal that the pneumatization of the uncinate process is due to overpneumatization of the agger nasi cell [29]. Pneumatization of the uncinate process occurs by the extension of the agger nasi cell into the anterior-superior part of the uncinate process [14, 30]. Many studies give a small percentage to this anatomical variation, between 0.4% and 13%. Kennedy and Zinreich [15] found the presence of uncinate bulla in 1/230 patients (0.4%, the lowest value). Bolger et al. [14] also found a low value of 2.5% on 202 CT scans. Arslan et al. [29] found a prevalence of 4%, Earwaker [16] of 9.1%, and Riello and Boasquevisque [17] of 13%. Due to its rarity, there are also authors who found no cases in some study groups [14]. Kantarci et al. [13] reported a prevalence of 5% assessed on 512 CT scans. These authors consider that changes of the uncinate process can cause an important functional blockage of the osteomeatal complex. In our study, the prevalence of uncinate process pneumatization of 3.41% (7/205 cases) is comparable to that of Bolger et al. [14]. The prevalence of 4% found by Arslan et al. [31] is also close to our finding. Most cases (85.71%) showed various radiological signs of former rhinosinusitis indicating a possible role in the pathogenesis of rhinosinusitis. When associated with other anatomical variations that cause the narrowing of ethmoid infundibulum (Haller cell, middle turbinate abnormalities, concha bullosa), the risk of recurrent chronic rhinosinusitis increases. These anatomical variations were also often identified in our study. Crista galli pneumatization Crista galli is a median ridge of bone that projects from the cribriform plate of the ethmoid bone, and serves as a landmark in endoscopic surgery. It can be pneumatized, containing a cell usually coming from anterior ethmoid. Usually, this anatomical variation has no clinical response and can only be revealed on preoperative radiographs. The identification of crista galli, 1103 pneumatized or not, can be done in both axial and coronal planes, but relevant considerations are better made with the last mentioned. Anatomical variations of this surgical landmark regard various aspects of morphology in relation to the cribriform plate of the ethmoid or its pneumatization. All forms described morphologically can be pneumatized. Hajiioannou et al. [18] describe in their studies a crista galli classification in three categories and give a prevalence of pneumatization of 14.1%. The research could determine the prevalence for each type of crista galli pneumatization, the rates found by us being comparable to those in the mentioned studies, type II having the highest prevalence of 61.95% (127/205). Crista galli pneumatization was observed in 47 (47/205) cases, with a prevalence of 22.92%, slightly higher than in other studies [3]. Conclusions Pneumatization of the superior and supreme turbinate can only be diagnosed by imaging, best by coronal sections. Its prevalence is 29.76% and 10.24%, respectively, all types being identified and bilateral variations more common. Pneumatization of uncinate process, rare anatomical variation, unilateral or bilateral (3.41%) with predominantly unilateral forms, is often associated with anterior rhinosinusitis (85.71%). Crista galli pneumatization, identified in all three types (I, II, III) is a rare anatomical variation, with a prevalence of 22.92%, type II being the most commonly seen. Coronal sections are preferred to detect the pneumatization of all investigated structures, but axial and sagittal ones may also be useful, because they allow a better assessment of the degree of extension and location, and the association of other anatomical variations at this level. Acknowledgments This study is part of the “Anatomical variations of surgical landmarks used in the diagnosis and endoscopic rhinosinusal approach” project, and has been approved by the Research Ethics Committee of the “Grigore T. Popa” University of Medicine and Pharmacy, Iassy, Romania, No. 15368/09.08.2011. Author contribution All authors have equally contributed to the manuscript. References [1] Braun H, Stammberger H, Pneumatization of turbinates, Laryngoscope, 2003, 113(4):668–672. [2] Christmas DA, Ho SY, Yanagisawa E, Concha bullosa of a superior turbinate, Ear Nose Throat J, 2001, 80(10):692–694. [3] Bâldea V, Variante anatomice ale reperelor chirurgicale utilizate în diagnosticul şi abordul endoscopic rino-sinusal, Teză de doctorat, Iaşi, 2010, 229–288. [4] Bâldea V, Bâldea MC, Cobzeanu DM, Marinescu AN, Variante anatomice ale reperelor chirurgicale endoscopice rino-sinusale – studii imagistice şi clinice, Colecţia “Esculap”, Ed. Junimea, Iaşi, 2013, 231–296. [5] Marks SC, Anatomy of the nose and sinuses. In: Marks SC, Nasal and sinus surgery, W.B. Saunders, Philadelphia, 2000, 3–30. [6] Hollinshead WH, Rosse C, The ear, orbit, and nose. In: Hollinshead WH, Rosse C (eds), Textbook of anatomy, Harper & Row, Philadelphia, 1985, 943–986. 1104 Mihail Dan Cobzeanu et al. [7] Donald PJ, Anatomy and histology. In: Donald PJ, Gluckman JL, Rice DH (eds), The sinuses, Raven Press, New York, 1995, 25–48. [8] Clerico DM, Pneumatized superior turbinate as a cause of referred migraine headache, Laryngoscope, 1996, 106(7):874– 879. [9] Stammberger H, Functional endoscopic sinus surgery: the Messerklinger technique, B.C. Decker, Philadelphia, 1991. [10] Hollinshead WH, Anatomy for surgeons, Hoeber Medical Division, Harper & Row, New York, 1968. [11] Christmas DA, Mirante JP, Yanagisawa E, Supreme nasal turbinate as a landmark during endoscopic sphenoid sinus surgery, Ear Nose Throat J, 2004, 83(2):84–85. [12] Mafee MF, Endoscopic sinus surgery: role of the radiologist, AJNR Am J Neuroradiol, 1991, 12(5):855–860. [13] Kantarci M, Karasen RM, Alper F, Onbas O, Okur A, Karaman A, Remarkable anatomic variations in paranasal sinus region and their clinical importance, Eur J Radiol, 2004, 50(3):296–302. [14] Bolger WE, Butzin CA, Parsons DS, Paranasal sinus bony anatomic variations and mucosal abnormalities: CT analysis for endoscopic sinus surgery, Laryngoscope, 1991, 101(1 Pt 1): 56–64. [15] Kennedy DW, Zinreich SJ, The functional endoscopic approach to inflammatory sinus disease: current perspectives and technique modifications, Am J Rhinol, 1988, 2(3):89–96. [16] Earwaker J, Anatomic variants in sinonasal CT, Radiographics, 1993, 13(2):381–415. [17] Riello APFL, Boasquevisque EM, Anatomical variants of the ostiomeatal complex: tomographic findings in 200 patients, Radiol Bras, 2008, 41(3):149–154. [18] Hajiioannou J, Owens D, Whittet HB, Evaluation of anatomical variation of the crista galli using computed tomography, Clin Anat, 2010, 23(4):370–373. [19] Van Alyea OE, Ethmoid labyrinth: anatomic study, with consideration of the clinical significance of its structural characteristics, Arch Otolaryngol, 1939, 29(6):881–902. [20] Ariyürek OM, Balkanci F, Aydingöz U, Onerci M, Pneumatised superior turbinate: a common anatomic variation? Surg Radiol Anat, 1996, 18(2):137–139. [21] Orlandi RR, Lanza DC, Bolger WE, Clerico DM, Kennedy DW, The forgotten turbinate: the role of the superior turbinate in endoscopic sinus surgery, Am J Rhinol, 1999, 13(4):251–259. [22] Yanagisawa E, Yanagisawa K, Christmas DA, Endoscopic localization of the sphenoid sinus ostium, Ear Nose Throat J, 1998, 77(2):88–89. [23] Bolger WE, Keyes AS, Lanza DC, Use of the superior meatus and superior turbinate in the endoscopic approach to the sphenoid sinus, Otolaryngol Head Neck Surg, 1999, 120(3): 308–313. [24] Kim HU, Kim SS, Kang SS, Chung IH, Lee JG, Yoon JH, Surgical anatomy of the natural ostium of the sphenoid sinus, Laryngoscope, 2001, 111(9):1599–1602. [25] Stammberger H, Wolf G, Headaches and sinus disease: the endoscopic approach, Ann Otol Rhinol Laryngol Suppl, 1988, 134:3–23. [26] Ozcan KM, Selcuk A, Ozcan I, Akdogan O, Dere H, Anatomical variations of nasal turbinates, J Craniofac Surg, 2008, 19(6): 1678–1682. [27] Orhan M, Govsa F, Saylam C, A surgical view of the superior nasal turbinate: anatomical study, Eur Arch Otorhinolaryngol, 2010, 267(6):909–916 [28] Zinreich SJ, Abayram S, Benson ML, Oliveiro PJ, The ostiomeatal complex and functional endoscopic surgery. In: Som PM, th Curtin HD (eds), Head and neck imaging, 4 edition, Mosby, St. Louis, 2003, 149–174. [29] Laine FJ, Smoker WR, The ostiomeatal unit and endoscopic surgery: anatomy, variations, and imaging findings in inflammatory diseases, AJR Am J Roentgenol, 1992, 159(4):849– 857. [30] Som PM, Curtin HD, Chronic inflammatory sinonasal diseases including fungal infections. The role of imaging, Radiol Clin North Am, 1993, 31(1):33–44. [31] Arslan H, Aydinlioğlu A, Bozkurt M, Egeli E, Anatomic variations of the paranasal sinuses: CT examination for endoscopic sinus surgery, Auris Nasus Larynx, 1999, 26(1):39–48. Corresponding author Mihail Dan Cobzeanu, Professor, MD, PhD, Department of Otorhinolaryngology, “Grigore T. Popa” University of Medicine and Pharmacy, 16 Universităţii Street, 700115 Iassy, Romania; Phone +40722–628 390, e-mail: [email protected] Received: December 3, 2013 Accepted: November 7, 2014