Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
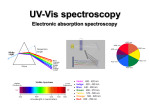
Evidence In-Sight: Best practices at service transition points Date: September, 2012 www.excellenceforchildandyouth.ca ● www.excellencepourenfantsados.ca Transitions The following Evidence In-Sight report involved a non-systematic search and summary of the research and grey literature. These findings are intended to inform the requesting organization, in a timely fashion, rather than providing an exhaustive search or systematic review. This report reflects the literature and evidence available at the time of writing. As new evidence emerges, knowledge on evidence-informed practices can evolve. It may be useful to re-examine and update the evidence over time and/or as new findings emerge. Evidence In-Sight primarily presents research findings, along with consultations with experts where feasible and constructive. Since scientific research represents only one type of evidence, we encourage you to combine these findings with the expertise of practitioners and the experiences of children, youth and families to develop the best evidence-informed practices for your setting. While this report may describe best practices or models of evidence-informed programs, Evidence In-Sight does not include direct recommendations or endorsement of a particular practice or program. This report was researched and written to address the question: What does the literature indicate are best practices at key transition points for children, youth and families from service to service and sector to sector? We prepared the report given the contextual information provided in our first communications (see Overview of inquiry). We are available at any time to discuss potential next steps. We appreciate your responding to a brief satisfaction survey that the Centre will e-mail to you within two weeks. We would also like to schedule a brief phone call to assess your satisfaction with the information provided in the report. Please let us know when you would be available to schedule a 15-minute phone conversation. Thank you for contacting Evidence In-Sight. Please do not hesitate to follow up or contact us at [email protected] or by phone at 613-737-2297. Page | 2 Transitions 1. Overview of inquiry Open Minds, Healthy Minds: Ontario’s Comprehensive Mental Health and Addictions Strategy, commits to the creation of 18 Service Collaboratives to support coordinated services for youth and adults. The Centre for Addiction and Mental Health (CAMH) is sponsoring the System Improvement through Service Collaborative (SISC) initiative to create these Service Collaboratives. The overall goal of the initiative is to support local systems to improve coordination and enhance access to mental health and addictions services. The first four Service Collaboratives have been established and are identifying gaps in the services available to children, youth, and families. One critical gap that has been identified is the smooth transition of children, youth, and their families from service to service, sector to sector, and from child to adult services. Transitions occur at a single point in time and also over time and across organizations. Children and youth transition from service to service within a continuum of care, such as from residential treatment to a community-based support service. They transition to services across sectors, such as from inpatient psychiatric care back to school or from the juvenile justice system to the community mental health system. And they transition from child and youth mental health services to adult mental health services. The issue of transitions is a complex one because best practices may vary depending on client factors and on what the actual transition entails. Given existing gaps, immediate priorities for the service collaboratives are to: 1. Establish service pathways, partnerships, and protocols that support clients with complex needs at key transition points; 2. Provide a focus on transition services for youth with co-occurring disorders; 3. Provide enhanced access to and flow of services for clients with complex needs that is inclusive for First Nations, Inuit and Métis peoples; and 4. Provide services for youth transitioning to adult care that is youth-centered, evidence-informed, community driven, and coordinated. Given these priorities, the Centre of Excellence was commissioned to conduct a brief Evidence In-Sight scan of the research and grey literature to partially inform the first two priorities and provide a starting point to answer: What does the literature indicate are best practices at key transition points for children, youth and families from service to service and sector to sector? Are there existing models of service transition that are evidence-informed? Promising approaches? Are there recommendations that are evidence-informed specifically for clients: o With complex needs? o With co-occurring disorders? 2. Summary of findings According to the Institute of Medicine at the United States National Academy of Sciences, focusing on the critical transitions of high-risk patients and their caregivers between settings within the healthcare system may enhance care coordination and improve quality of care and care outcomes. Page | 3 Transitions Literature in the area of mental health lacks clear guidelines on transitions and transitional care. While literature related to transitions in the adult mental health sector is emerging, research specific to transitions in child and youth mental health remains limited. The literature on transitional care in other fields, such as cardiovascular care, does have guidelines that may be adaptable or otherwise applicable to mental health. For example, the literature on older adults transitioning from hospital to other services suggests: o Improve communications during transitions between providers, patients, and caregivers. o Implement electronic medical records, including standardized medication elements. o Establish points of accountability for sending and receiving care. o Use case management and professional care coordination. o Implement payment systems that align incentives and include performance measures to encourage better transitions of care. Although discharge is part of the transition process, care teams should focus on transitions as client transfer with continuous care, not just a discharge. Studies on discharge planning found that such interventions can reduce re-hospitalization of adults with chronic mental health problems and improve adherence to aftercare. Recommended practice elements for discharge planning are: o Hold at least one pre-discharge meeting with all parties involved. o Include the family in pre-discharge planning. In considering the transition between inpatient and outpatient treatment for youth admitted to the emergency department for a suicide attempt, a review of studies found that transition interventions can reduce subsequent suicide attempts post-discharge. Practices include: o Provide information on risk and protective factors, alternative behaviors, and referral options. o Enable follow-up contacts (telephone or in person). o Specialized intervention within the ED with a psychiatric evaluation, and follow-up therapy including a crisis therapy session and an outpatient treatment program focused on role-playing, problem-solving, and negotiation. o Availability of a rapid-response outreach team, including psychiatrist and psychiatric nurse. Common practice elements across two medical models of transitional care are: o Improve communication between settings. o Empower clients/patients through education about self-management. o Use a health care professional who works to bridge gaps between service providers. The literature on children with disabilities suggests that while transition practices may be universal, each practice should include strategies that are individually tailored to client and family needs. Systems of Care and the Key Worker Model are two evidence-informed practices that pertain to care coordination and that can contribute to effective service transitions, and that have been used effectively in the field of child and youth mental health. An Agency for Healthcare Research and Quality review identified effective strategies for care coordination that can contribute to improved patient and client transitions. Evidence-informed coordination practices include: o Multi-disciplinary teams. o Assertive community treatment. Page | 4 Transitions o o o o o Case management. Collaborative care. Disease management. Integrated care programs. Inter-professional education. 3. Answer search strategy and limitations This report provides a summary of available literature and a starting point for future research related to these important questions. This Evidence In-Sight scan was limited by the condensed timeline and the relative scarcity of resources focused on transitions in the area of child and youth mental health. Further work should include an in-depth, systematic review that is complemented by insights from national and international experts in this area. We found that most of the research literature on transitions and child and youth mental health is about transitioning from youth to adult services. Our initial search using terms such as child, youth, mental health, health, transitions, and best practice produced no empirical evidence that satisfies the questions posed by the services collaboratives. There is an emerging body of work on transitions between youth and adult mental health services, but contemporary work by Dr. Simon Davidson and colleagues demonstrates that even this field is emergent. For instance, there is as yet no truly proven model that can be replicated universally. We adapted our search by casting a wider net in order to find relevant information in related fields. The broader health literature, including oncology, geriatrics, and diabetes has some research on care transitions. However, this work focuses mainly on adults and/or transitions within clinical settings and therefore has limited generalizability to community-based child and youth mental health service provision in Ontario. As the topic of transitions is related to organizational and system integration and change, we further expanded our search and included the terms continuity of care, transitional care, and quality improvement. Where we looked for information: Google Scholar; EBSCOhost (MEDLINE, CINAHL, PsycINFO), University of Ottawa Scholars Portal, NREPP database, California Evidence-based Clearinghouse for Child Welfare Search terms: transition; transitional care; transitional services; child; youth; mental health; health; continuity of care; quality improvement Note that the health literature typically uses the term “patient” when referring to its client population. The Centre, however, prefers the term “client” when referring to children and youth in care. For the purposes of this report, the term “client/patient” will be used to reflect the diverse ways these are used. 4. Findings A varied literature informed our findings. In general, the literature that is specific to transitions in mental health services for children and youth is sparse. For instance, research used to guide mental health counselors in their work with adolescents during the transition from inpatient to school settings is very limited (Clemens et al., 2010). Similarly, while there is a body of work on the requirements for continuing care after discharge, there is a lack of information about how Page | 5 Transitions to make a transition effective and smooth for children, youth, and families receiving mental health services (Simon & Savina, 2005). Since the literature did not adequately provide answers, models, or lists of best-practice recommendations to answer the questions posed by the service collaboratives and CAMH, we have summarized information from various fields that can inform the development of best-practices within a system that coordinates care across services and sectors. The literature, both research and grey, is predominantly taken from adult services, but we did find useful practices in research with children and youth with developmental disabilities and other special needs. One challenge we encountered while investigating “transitions” is that, as a concept, it nests within other very similar but distinct concepts. As the work of Burns and colleagues (2008) illustrates, Managed Transitions are one of seven independent factors that contribute to continuity of care for clients and patients. Other literature demonstrates that continuity of care is positively associated with improved client outcomes. For existing research on transitioning to adult services, refer to the policy ready paper that the Centre has published, We’ve got growing up to do: Transitioning youth from child and adolescent mental health services to adult mental health services at http://www.excellenceforchildandyouth.ca/informing-policy/policy-papers. For this report, we consider transitions as a process as well as a point in time. 5. Transitions - the conceptual whole Focusing on key transitions of clients or patients and their families across settings and among providers is a promising approach to enhance care coordination and to improve quality (Naylor, 2006). In this section we assemble literature from related fields to demonstrate how transitions are one element that contribute to enhanced care coordination, and continuity of care. The following concepts are inter-related but distinct (National Transitions of Care Coalition, 2008a and 2008b). Transitional care or transitions of care is the scenario in which a patient/client is leaving one care setting and moving to another. This frequently involves multiple persons including the patient/client, family or other caregiver, nurses, social worker, case manager, physician, and other providers. An optimal transition is well planned and timed. Transitions can occur: Within settings, such as from the emergency department to an inpatient care setting. Between settings, such as from an inpatient care setting to a residential treatment facility. Across health states, such as from requiring acute inpatient care through recovery. Between providers, such as from the care of a psychologist at one agency to the care of a social worker at another. Transitions of care are actions to ensure coordination and continuity, and are based on a comprehensive care plan. Transitions of care are a subpart of the broader concept of care coordination and are the actions designed to ensure Page | 6 Transitions coordination and continuity of care. • Care coordination refers to the deliberate organization of patient/client care activities among multiple participants, including the patient/client and the family, to facilitate the appropriate delivery of care services. It involves bringing together the appropriate resources to carry out all required patient/client care activities and is often managed by the exchange of information among participants responsible for different aspects of care. Communication is a key practice in care coordination. • Continuity of care is a term that has been used interchangeably with care coordination, but is a unique concept. Although closely related, the precise meaning in the mental health field refers to coordination of services and the stability of patient-provider relationships over time. The relationship is often established with a team rather than a single care provider, and is coordinated through a common purpose and plan. Since transitions at a single point-in-time are one step in a constant and varied context of care activities across providers and systems, best practices related to transitional care, care coordination, and continuity of care may be necessary elements to fully implement good transition practices. 6. Transitions Transitional care or transitions of care encompasses a broad range of services and environments intended to promote safe and timely transfer across settings or among levels of care (Naylor, 2006). It is the aspect of client/patient management that promotes a series of actions to enhance continuity of care and facilitate a safe and timely transfer. While fields like cardiovascular care have well-established guidelines in this regard (e.g., see Arnold et al (2008) for a summary of guidelines published by the Canadian Cardiovascular Society), the mental health literature (particularly that which focuses on child/youth mental health) lacks clear recommendations on transitional care, but is emerging. 6.1 Research on transitional care In considering the transition between inpatient and outpatient treatment for youth admitted to the emergency department (ED) for a suicide attempt, a review of studies found that transition interventions can reduce subsequent suicide attempts post-discharge (Newton et al., 2010). This finding is important because few ED interventions on their own have been shown to reduce subsequent suicidal behavior and related hospitalizations, whereas interventions initiated in the ED combined with continued community-based treatments have been shown to impact suicide-related outcomes. The review found treatment adherence was improved when: • Treatment barriers were addressed. • Treatment expectations were discussed. • Session attendance was negotiated. A small study on the effect of a transition intervention among adults on subsequent use of outpatient services after psychiatric hospitalization found improved attendance at follow-up appointments (Batscha et al., 2011). The intervention was an adaptation of the Care Transitions Program and the Transitional Care Model, which were both designed for chronically ill high-risk older adults hospitalized for medical and surgical conditions (recommended practices from these models are summarized later in this report). Core practice elements of the two models are: • Improve communication between settings. • Empower clients/patients through education about self-management. Page | 7 Transitions • Use a health care professional who works to bridge gaps between service providers. A synthesis of the literature on transitions for children with disabilities highlights how the study of transitions is complex and there is need for evidence-based practices (Rous & Hallam, 2012). They demonstrate that practices are universal, while each practice should include strategies that are individually tailored to client and family needs. 6.2 Transitional care guidelines Looking across services for children and youth, the government of Alberta has basic guidelines for supporting children and youth at key milestones or within a variety of circumstances (Alberta Children and Youth Initiative, 2006): 1. Ensure that basic needs are met. 2. Maintain and encourage positive relationships. 3. Provide support and resources to children and youth in their new environment and modify or adapt as needed. 4. Involve the child or youth in the transition process. 5. Support the need for increased independence and help children and youth create their own identity. 6. Ensure that all transition plans are coordinated and integrated, and that information is shared with families and across sectors. 7. Prepare for the transition and ensure consistency within and between environments. A study on youth transitioning from inpatient hospital care back to school presented ideas for hospital practitioners to use during the transition process (Simon & Savina, 2005): 1. Identify the child’s needs, concerns, and resources before discharge to address them through interventions at the hospital or during the transition. 2. Explain the importance of a smooth transition to parents, and ask them to sign a Release of Information form to be able to share information between hospital and school personnel. 3. Identify a contact person within the school and direct relevant information to that person. 4. With the parent’s permission, invite the school contact person to the join in the child’s discharge meeting. 5. Provide parents and school personnel with materials explaining the transition process and factors that could undermine transition success. One study from the special needs field used a series of focus groups held across the United States with family members, administrators, and practitioners to identify practices to help children and families at key transitions (Rous et al., 2007). Practices recommended by participants include: • Have a supportive infrastructure including guidelines and policies, personnel dedicated to transition planning, and clear support from administration. • Provide support and time for communication and developing collaborative relationships across key players and agencies. • Use developmentally appropriate practices that match client abilities, making service provision and the transition process be family-centered. Of the three studies in the Newton (2010) review that looked at transition interventions, practices include: • Information post-discharge on risk and protective factors, alternative behaviors, and referral options. Page | 8 Transitions • • • Follow-up contacts (telephone or in person). Specialized intervention within the ED with a psychiatric evaluation, and follow-up therapy including a crisis therapy session and an outpatient treatment program focused on role-playing, problem-solving, and negotiation. Availability of a rapid-response outreach team, including psychiatrist and psychiatric nurse. Discharge planning is one part of transitions with evidence for improved outcomes. A systematic review of available studies on discharge planning found that such interventions can reduce re-hospitalization of adults with chronic mental health problems and improve adherence to aftercare (Steffen et al., 2009). Core recommended practice elements for discharge planning are: 1. Hold at least one pre-discharge meeting with all parties involved. 2. Include the family in pre-discharge planning. Best practices in health settings might be specific to the particular client/patient need and the medical condition, such as cardiovascular care or the transition to home nursing. Nonetheless, the Massachusetts State Quality Improvement Institute did develop common practice recommendations for effective care transitions in its Strategic Plan for Care Transitions (Bonner et al., 2010): 1. Essential clinical information is provided upon discharge. 2. Clients/patients have the opportunity to ask questions. 3. There is a seamless clinical transfer, with a responsible clinician, and there are no lapses in care. 4. There is logistical and management support for clients/patients and families. 5. There is a quality measurement process. The Massachusetts Strategic Plan also suggests seven guiding principles for transitions: 1. Information should be provided in a timely manner via standardized care plans and transition records. 2. Transitions should be supported by a communications infrastructure. 3. Clients/patients and families should be active participants in the transition planning and process. 4. Accountability for care during the transition remains with the sending providers until the receiving providers acknowledge responsibility for care. 5. Providers should be actively engaged in and agree upon transition practices. 6. Transitions should be assessed using standardized process and outcome measures. 7. The incentives of providers and clients/patients should be aligned by payment processes from funders. Geriatric medicine has been particularly active in researching transitional care. For instance, the National Coordinating Centre for Integrating Care for Populations and Communities in the United States has developed an entire toolkit to help clients/patients, families, and communities achieve improved transitions between care settings and the home. The toolkit is freely available at http://www.cfmc.org/integratingcare/toolkit.htm. The National Transitions of Care Coalition built on previous work by the Institute of Medicine to develop transitional care recommendations: 1. Improve communications during transitions between providers, clients/patients, and caregivers. Page | 9 Transitions 2. 3. 4. 5. Implement electronic medical records, including standardized medication elements. Establish points of accountability for sending and receiving care. Use case management and professional care coordination. Implement payment systems that align incentives and include performance measures to encourage better transitions of care. 6.3 Two models of transitional care We did identify two existing models of transitional care with supporting evidence. They were both developed within the context of medical care for older adults, but the central guiding principles could be adapted to other settings, and at least one study has adapted one of the models to apply it to mental health services for adults. The Care Transitions Program is an evidence-informed model that has been developed for transitions of older adults from hospital to other settings and has been through a randomized control trial. A randomized controlled trial of the program found that encouraging patients and their caregivers to assert a more active role in their care transitions resulted in reduced re-hospitalization rates (Coleman et al., 2006). Essential components of the 4-week program are: • Patients with complex care needs receive specific tools. • Patients receive support from a Transitions Coach. • Patients learn self-management skills to ensure their needs are met during the transition from hospital to home. • A pre-discharge meeting with the patient is used to identify and address barriers to attendance at follow-up care and to determine familiarity with available services. An appointment reminder letter is provided, and an outpatient service provider is present at the discharge meeting. The lead developer of the Care Transitions Program, Dr. Eric Coleman, is actively involved in transitions research and policy development, and has developed recommendations pertaining to accountability and information in transitional care. Accountability - Health care organizations should (Coleman and Fox, 2004): 1. Establish policies and procedures for patients undergoing transitions and educate contracted or affiliated providers and facilities about relevant policies and procedures. 2. Ensure that patients undergoing care transitions have an identified and responsible practitioner at all times. 3. Establish performance standards for care transitions, and monitor performance. 4. Only contract with or work with practitioners and other organizations that satisfy predefined standards. 5. Develop collaborative relationships among providers to commonly establish performance expectations and share in monitoring quality. Information - Health care organizations should (Coleman and Fox, 2004): 1. Define the essential data elements required to provide high quality care to transitioning patients. 2. Assure that the essential data elements are conveyed to the receiving practitioners. 3. Develop and maintain user-friendly information systems to communicate and share information across the continuum of care. The following are core functions for meeting the needs of patients in transition (Coleman and Fox, 2004). Both the sending and receiving care teams should: Page | 10 Transitions • • • Focus on the process as a patient transfer with continuous management, not a patient discharge. Incorporate patient and caregiver preferences into the care plan. Identify the patient’s system of social support and baseline level of function, which will inform how effectively they might care for themselves after discharge. • Communicate and collaborate with practitioners across settings to formulate and execute a common care plan. • Use a shared, preferred mode of communication with collaborators. The sending health care team should ensure that: • The patient is stable enough to be transferred to the next care setting • The patient and caregiver understand the transfer purpose • The receiving organization is capable of and prepared to meet patient needs • All relevant transfer information is complete. • The care plan, orders, and a clinical summary precede the patient’s arrival to the next care setting. • The patient has a timely follow-up appointment with an appropriate professional. • A professional from the sending care team is available for several days after discharge to the patient, caregiver, and receiving care team to discuss the care plan. The receiving care team should ensure that: • Transfer forms, clinical summary, discharge summary, and physician’s orders are reviewed prior to or upon the patient’s arrival. • The patient’s goals and preferences are incorporated into the care plan. • Discrepancies or confusion about the care plan, patient status, or medications are clarified with the sending care team. The Transitional Care Model is very similar to the Care Transitions Program. It focuses on patient and caregiver understanding and was developed for older adults transitioning from hospital medical care to other settings. Key elements are (Transitional Care Model): 1. Use a Transitional Care Nurse as the primary coordinator of care to assure consistency of provider across the entire episode of care (note that this element was omitted in the Batchsa et al. (2011) adaptation). 2. In-hospital assessment, preparation, and development of an evidence-based plan of care. 3. Comprehensive, holistic focus on each patient’s needs including complicating or coexisting events. 4. Active engagement of patients and their family and informal caregivers. 5. Emphasis on early identification and response to risks and symptoms. 6. Multidisciplinary approach that includes the patient, family, informal and formal caregivers. 7. Physician-nurse collaboration. 8. Communication to, between, and among the patient, family, and health care providers and other professionals. 7. Care Coordination Care coordination has been identified by the Institute of Medicine (IOM,) the independent health arm of the United States National Academy of Sciences, as a key strategy to improve the effectiveness and efficiency of health care systems. According to the IOM, focusing on the critical transitions of high-risk patients and their caregivers between settings within the healthcare system may enhance care coordination and improve quality (Naylor, 2006). Page | 11 Transitions An Agency for Healthcare Research and Quality (2007) technical review found that while many care coordination programs have not been evaluated, the strongest evidence does show benefit from care coordination for clients with severe mental illness. It also proposed a working definition of care coordination (McDonald et al, 2007): Care coordination is the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of health care services. Organizing care involves the marshaling of personnel and other resources needed to carry out all required patient care activities, and is often managed by the exchange of information among participants responsible for different aspects of care (page 41). Care coordination may involve service integration. According to Brechman-Tousaint and Kogler (2010), integrated service delivery means different things to different people and can operate differently in different contexts. For instance, in the Australian context, some integration efforts are top down with government policies and funding models supporting an integrated across-agency approach, while in others integration occurs at the local and regional level via interagency service agreements and local protocols. There is disagreement about which of these general approaches is most advantageous when it comes to creating effective change (Brechman-Tousaint and Kogler, 2010). The following are two evidence-informed practices that pertain to care coordination and that can contribute to effective service transitions: Key Worker model Description The Key Worker model involves a single person acting as a point of contact for a family and helping them to coordinate care within and across systems. The main goal of this approach is to empower parents by providing them with support, resources and information tailored to meet their unique family needs. It is similar to traditional case management, although the key worker model emphasizes empowering parents and involving them in decision making, and also in working across multiple systems rather than just the particular area of health need. Evaluation Limited. The literature indicates that some evaluation exists, typically on user satisfaction. Some recent evaluation work in the UK and British Columbia found promising process findings and suggested strategies to improve the Key Worker program in their jurisdictions. Systems of care and System-of-care Description Systems of care are a set of principles and practices developed in the United States. It is a service delivery approach that builds partnerships to create a broad, integrated process for meeting families’ multiple needs (Whitson et al, 2010). The approach is based on interagency collaboration, individualized and strengths-based care practices for clients, cultural competence, community-based services, accountability, and the full participation of families and youth. Systems of care focus on building the infrastructure needed to result in positive outcomes for children, youth, and families. Systems of care is an overarching philosophy, while a local system-of-care is a unique model that incorporates an array of services and supports in a coordinated network of integrated care planning and management. The Child and Youth Mental Health Network in Ottawa conducted a practice review and then implemented a system of care in 2007-2011. The initiative includes representation from Page | 12 Transitions Evaluation multiple child and youth mental health and substance abuse serving agencies in the Ottawa region, with Coordinated Access at the center of activities, including intake, triage, and case resolution. More than 70,000 children and their families have received services through system of care programs in the United States, and outcomes research is mixed. One study found that system of care communities provided more family-focused care, supportive collaboration, individualized plans, adequate access, and less restrictive services than comparison sites. Another study found that although service access and amount increased in a system of care, children who did not receive services improved at the same rate as those who did. However, another outcomes study found fewer internalizing and externalizing symptoms in children who received system of care services, and greater family satisfaction (Whitson et al, 2010). The University of South Florida worked together with the Coordinated Access network in Ottawa to conduct a baseline System of Care Practice Review using a tool specifically intended to measure the experiences of children with severe emotional disturbances and their families, to document adherence to the system of care philosophy by direct service providers and system, and to assess the degree to which the system of care philosophy is implemented at the practice level and generate recommendations for improvement. A Canadian Health Services Research Foundation report analyzed ten local mental health networks from 2003 to 2006 to develop a descriptive framework of the governance mechanisms used to develop systems of coordinated care (Wiktoowicz, 2009). The paper identified three governance models: corporate structure, alliance, and voluntary mutual adjustment. General findings were: Care coordination is facilitated by local mental health networks that foster relationships among clinical, addictions, rehabilitation and housing services Implementing coordinated care involves translating policy into client-related activities mediated by numerous organizations. Cooperation among mental health organizations determines the degree of care coordination. A network executive committee is instrumental in developing a shared vision and offers a forum to align contributions and strategically focus resources. An alliance model of governance fosters cooperation in most small- to mid-size urban and rural local networks. Metropolitan networks face the greatest challenges in developing an alliance since achieving a common vision and dialogue among many organizations is complex. Metropolitan networks with an alliance model require greater administrative support to develop a common vision and foster coordination. Metropolitan networks with a psychiatric hospital experience challenges in coordinating care as hospitals offer a range of programs and have less need to connect to their network. Issues of confidentiality may pose obstacles to care coordination among organizations. Dividing budget and planning authority between the provincial government and network (or regional) governance could impede coordination. Other key drivers of service integration include: Centralized access and intake. Page | 13 Transitions A shared information system to track pathways of care by facilitating providers’ access to client files, including medication information, admission information, and services that have supported the client. Involvement of psychiatric hospitals, so that the entire care network can leverage the specialized care that they offer. The home healthcare literature suggests three essential ingredients for care coordination (Naylor, 2006): 1. Relationships. Home healthcare nurses are an example of key players who are recognized as strong advocates for patients and families. This suggests that, at a systems level, key individuals should be a consistent presence over time for patients, and that they can act as relationship builders between relevant services. 2. Management. The use of risk screens upon admission can help match the skill level of clinicians and the nature of services to the client. Systems of care management should anticipate the changing needs of clients. 3. Information. Clinicians should be actively involved in using information systems and forms that assist in the transfer of information across settings. Previous research has found that the use of a case or discharge summary that details patient goals, progress, and recommendations and that is provided to the patient/caregiver and all involved physicians can facilitate effective transitions. An Agency for Healthcare Research and Quality review of systematic reviews that focused entirely on care coordination found 13 reviews that focused on patients with mental health problems (McDonald et al., 2007). Effective strategies for care coordination were: Multi-disciplinary teams. Assertive community treatment. Case management. Collaborative care. Disease management. Integrated care programs. Inter-professional education. 8. Continuity of Care Continuity of care is different from but complementary to coordination of care. Although the two concepts are closely related, the precise meaning of continuity of care in mental health refers to the stability of services and the patientprovider relationship over time. The relationship is often established with a team rather than a single care provider, and is coordinated through a common purpose and plan. Care coordination is more about the organization of services so that continuity is assured. Continuity of care in mental health services emphasizes coordination of services and the stability of patient-provider relationships over time (Haggerty et al., 2003). It reflects a coherent and connected series of care events, and should be consistent with the individual context and needs of the client. Continuity of care is team-oriented and extends to other services, with case managers appointed to facilitate services across health and social domains such as housing, substance abuse treatment, and employment support. Access to services is often included as a dimension of continuity, and issues of continuity and accessibility are closely tied. Page | 14 Transitions A recent study illustrates why continuity of care is important for achieving good outcomes for children and youth in mental health services. A retrospective analysis of data in the United States found that most adolescents admitted to the emergency department for deliberate self-harm were released to the community at discharge and did not receive mental health assessments or follow-up outpatient mental health services (Bridge et al., 2012). For the sample in this study, admission to the hospital was related to several known risk factors for suicide. Continuity of care can be organized into three dimensions: 1. Informational continuity – use of information on past events and client circumstances to inform current care. 2. Interpersonal continuity – an ongoing therapeutic relationship. 3. Management continuity – a consistent and coherent approach to managing care needs in response to a client’s changing needs. The state of Rhode Island’s Safe Transitions Project has evidence-informed guidelines on communication between hospitals and physician offices to facilitate continuity of care through the transition from hospital to community care. They developed these practice recommendations to improve care transition outcomes (Baier et al., 2011): Hospitals should: 1. Notify community physicians about the ED visit and hospitalization. 2. Upon discharge, provide the receiving community physician with the hospital physician contact information. 3. Provide effective education to patient prior to discharge. 4. Provide written discharge instructions to patient prior to discharge. 5. Provide follow-up telephone number to patient prior to discharge. 6. Schedule outpatient follow-up appointment prior to discharge. 7. Upon discharge, provide community physician office with summary clinical information. Community physician offices should: 1. Provide the ED with clinical information when referring patients for evaluation. 2. Respond to time-sensitive ED and hospital clinical questions. 3. Provide ED and hospital clinicians with access to outpatient clinical information, if needed. 4. Confirm outpatient receipt of discharge information from the hospital. 5. Outreach to high-risk patients via telephone after ED or hospital discharge. 6. Conduct follow-up visit with patients discharged to the community. A systematic review found that increased provider continuity is associated with improved patient outcomes and satisfaction, although it is unclear the degree to which information and management affects outcomes (Walraven et al., 2010). Other research has found a positive association between overarching systems integration and client continuity of care (Durbin et al., 2006). The best results occurred in systems integration efforts characterized by: Strong management arrangements. Fewer service sectors. System wide implementation of intensive case management. Centralized access to services. Page | 15 Transitions The overarching concept of continuity of care can be broken down into multiple independent but inter-related concepts, including transitions (Burns et al., 2008). The quality improvement literature also informs continuity of care and provides some recommendations on good practice during health transitions. Using specified domains of transitions of care, Cotter and colleagues (2002) defined five activities: 1. Conduct a comprehensive and accurate assessment of patient needs. 2. Educate the patient and their family regarding the health condition and post-discharge and self-care requirements. 3. Make arrangements for care after discharge. 4. Communicate the care plan among the patient, family, current care provider, and community based care provider. 5. Implement and adjust the care plan. 9. Special populations Youth Justice In the youth justice sector, transitioning from incarceration to the community is commonly called “reentry". Reentry programs are meant to prepare out-of-home placed juveniles for reintegration into the community and to smooth the transition. A comprehensive reentry process begins after sentencing, continues during incarceration and/or intervention (for instance in a residential facility), and goes into the period of release back into the community. Reentry requires the creation of a seamless set of systems and a continuum of community services to prevent the reoccurrence of antisocial behavior (U.S. Department of Justice). There is evidence that transition planning is correlated with reduced rates of recidivism among mentally ill juvenile offenders. For instance, a study by Trupin and colleagues (2004) found that community transition planning, including the coordination and provision of community services, was a component of community reintegration that was associated with lower rates of recidivism during the first year post-discharge. The mental health status of participants was measured using the Child and Adolescent Functional Assessment Scale (CAFAS). Mental health services did not include provision of evidence-based programs and the authors note that using client-appropriate evidence-based interventions could potentially improve outcomes. A search of repositories of evidence-based programs did not yield any programs that are specifically intended for the transition point between incarceration and release. We did identify one promising program: Family Integrated Transitions (FIT), in Washington State. A pilot evaluation found reduced recidivism in felony offences. At this point it remains a promising program and further evaluation is required. The program is a family-based intervention for youth with co-occurring disorders who are transitioning from incarceration back into the home. It integrates existing evidence-based programs within multiple contexts (individual, family, community, school) (Trupin et al, 2011): Multi-systemic therapy – the core treatment model Page | 16 Transitions Dialectical behavior therapy Motivational enhancement training Relapse prevention/Community reinforcement A parent training element Elements of FIT are delivered in multiple contexts over time. Family strength-based services begin 2 months prior to release to ensure engagement and strengthen supports. Fit continues for 4 months post-release. Family engagement and behavioral change in the home environment are key tasks. Masters-level clinicians/coaches are available at all times and address family and community involvement. Caseload is 4-6 families per clinician. Weekly supervision for clinicians is provided by a program expert. Family members are included in assessing the performance of clinicians. Clients with complex needs In 2008 a Pediatric Complex Care Coordination Expert Panel developed guidelines for implementing and assessing care coordination. The summary report of the panel findings provides a framework for complex care coordination, a proposed general model, suggested performance measures, and implementation guidelines (Report of the Paediatric Complex Care Coordination Expert Panel, 2008). Recommended key enablers of a successful approach include: Data collection and technology elements. A complex care coordination role (a key worker) as single point for care coordination, working in close concert with the family. A “most responsible” physician. Share overall care between local health care team and secondary and tertiary centres. The expert panel recommended using a community-based model of coordination rather than basing coordinated activities out of a tertiary care facility. Being community-based, coordination workers would work out of either a mandated clinic or a participating organization. Actual care centers would have multiple services on site. 10. Evaluation Considerations Measures of care transitions are typically based upon agreed standards of care and practice (National Transitions of Care Coalition, 2008a). The National Transitions of Care Coalition suggests considering the following elements if developing and/or using care transition measures: 1. Whether to evaluate the transition process for all patients or only those identified as high risk. 2. Whether the evaluation measures are relevant to all care organization settings and providers, or to a defined subset. 3. What types of measure to use: structure, process, outcome, patient experience, efficiency, and/or effectiveness. 4. Whether to focus the measures on the patient’s perspective or experience, and/or the provider’s perspective or experience. Page | 17 Transitions 5. What is the feasibility of data sources and data collection. 6. What is the unit of measurement: organization/facility/practice, individual health care professionals, multidisciplinary teams, system level, communities, population. Assessments of care coordination typically use five types of measures (McDonald et al, 2007): 1. Patient outcomes. 2. Cost outcomes. 3. Care delivery process measures. 4. Coordination mechanism measures. 5. Patient/family perception of coordination. McDonald and colleagues (2007) summarized four existing conceptual frameworks of care coordination from the literature and identified the common concepts across them. These concepts could be useful for evaluating care coordination interventions and programs because they fit three general areas that could be used to develop an analytic framework. The three domains are: 1. Baseline assessment of the setting, the client population, and other factors that might influence the amount of coordination that is needed. 2. The actual coordination mechanisms within the coordination network. 3. The outcomes that the coordination effort are intended to achieve. When taken together the frameworks demonstrate a general approach to applying concepts that help systems level decision makers and service level leaders characterize and assess care coordination approaches. The general approach includes (McDonald et al., 2007): 1. Assess the needs for coordination by reviewing baseline characteristics for a given practice setting and patient population. 2. Identify the options for improving coordination by reviewing potential coordination mechanisms and considering their fit with the demands of the particular circumstances. 3. Select and implement one of the alternatives. 4. Evaluate to determine effects on coordination and outcomes of care. 5. Repeat if needed to test alternative solutions. 11. Next steps and other resources Transitions are a topic with significance to system transformation and care integration, so we encourage the collaboratives to consider how best practices in implementation and evaluation can contribute to integrating new practices into organizations and a connected system. This report incorporates information on transitional care, care coordination, continuity of care, quality improvement, and evaluation considerations. The National Transitions of Care Coalition, a body based in the U.S., “provides tools and resources to patients, caregivers, health care professionals and policy makers who seek to address challenges in meeting the needs of patients transitioning between care settings.” Resources can be accessed at http://www.ntocc.org/Home.aspx. Page | 18 Transitions The children with disabilities literature is much more developed, in terms of key transitions, than the child and youth mental health literature. For a handbook on transitional planning, see Bridging Early Services for Children with Special Needs and Their Families at http://clas.uiuc.edu/fulltext/cl04154/cover-chpt1.pdf. Dr. Simon Davidson, at the Children’s Hospital of Eastern Ontario and the Centre of Excellence, is conducting work specific to best practices and effective models of transition from child to adult care. He is available to discuss his particular part of the overall transitions set of questions. The Centre is currently developing engagement activities specific to practitioners working with priority (underserved) populations (i.e., First Nations, Inuit and Métis; ethno-culturally diverse; and Francophone communities). In each of these populations, needs and strengths related to transitions planning are diverse, and therefore require a specific focus that is beyond the scope of this report. These priority areas are complex and beyond the scope of Evidence In-Sight, so reviews of the literature will not be conducted at this time. Youth and family engagement are priority topics for the Centre. We can provide existing resources on youth engagement and youth- and family-centred services, including literature that was used to develop a training program. You will receive an email from the Centre within the next two weeks, with a link to a survey to help us understand whether the information provided in this report is useful and relevant to your needs and how Evidence In-Sight can be improved to better serve agencies such as yours. Please take a moment to respond when you receive the link, as your feedback is important to us. Thank you. Knowing what works and receiving training on an evidence-informed practice or program is not sufficient to actually achieve the outcomes that previous evaluations indicate are possible. A program that has been shown to improve mental health outcomes for children and youth but that is poorly implemented will not achieve successful outcomes (Fixsen et al, 2005). In order for a program to be evidence-informed, it needs to be applied with fidelity to the design and it needs to be implemented using supportive “drivers” related to staff competency, organizational leadership and organizational capacity. These drivers include assessing and monitoring the outcomes of your practice using evaluation or performance measurement frameworks, which are particularly important when there is insufficient evidence in the literature to guide clinical decisions. Choosing a practice is an initial step toward implementation, but the implementation drivers are essential to ensure that the program reaches appropriate clients, that outcomes are successful and that clinical staff members are successful in their work. The Ontario Centre of Excellence for Child and Youth Mental Health has a number of resources and services available to support agencies with implementation, evaluation, knowledge mobilization, youth engagement and family engagement. For more information, visit: http://www.excellenceforchildandyouth.ca/what-we-do or check out the Centre’s resource hub at http://www.excellenceforchildandyouth.ca/resource-hub. For general mental health information, including links to resources for families: http://www.ementalhealth.ca Page | 19 Transitions References AACAP Official Action. (2007). Practice Parameter on Child and Adolescent Mental Health Care in Community Systems of Care. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 2. 284-299. Alberta Children and Youth Initiative. (2006). Guidelines for Supporting Successful Transitions for Children and Youth. Arnold, J.M., Howlett, J.G., Ducharme, A., Ezekowitz, J.A., Gardner, M.J., Giannetti, N., Haddad, H., Heckman, G.A., Isaac, D., Jong, P., Liu, P., Mann, E., McKelvie, R.S., Moe, G.W., Svendsen, A.M., Tsuyuki, R.T., O’Halloran, K., Ross, H.J., Sequeira, E.J., White, M. (2008). Canadian Cardiovascular Society Consensus Conference guidelines on heart failure – 2008 update: Best practices for the transition of care of heart failure patients, and the recognition, investigation and treatment of cardiomyopathies. Canadian Journal of Cardiology, 24, 1, 21–40. Baier, R., Gardner, R., Gravenstein, S., Besdine, R. (2011). Partnering to Improve Hospital-Physician Office Communication through Implementing Care Transitions Best Practices. Rhode Island Medical Society, 94, 6, 178- 182. Accessed at http://www.rimed.org/medhealthri/2011-06/2011-06-178.pdf on August 6, 2012. Batscha, C., McDevitt, J., Weiden, P., Dancy, B. (2011). The Effect of an Inpatient Transition Intervention on Attendance at the First Appointment Postdischarge From a Psychiatric Hospital. Journal of the American Psychiatric Nurses Association, 17, 5, 330-338. Bonner, A., Schneider, C.D., Weissman, J.S., (2010). Massachusetts Strategic Plan for Care Transitions. Massachusetts State Quality Improvement Institute. Massachusetts Executive Office of Health and Human Services. Accessed at http://www.mahealthdata.org/resources/Documents/Strategic%20Plan%20for%20Care%20Transitions_2-112010%20%282%29.pdf on August 8, 2012 Brechman-Tousaint, M. & Kogler, E. (2010). A review of integrated service models for young people in the preadolescent and adolescent years: Benefits, barriers and enablers. Australian Research Alliance for Children and Youth. Available at: http://www.aracy.org.au/cmsdocuments/Review_of_international_and_national_integrated_service_models.pdf Bridge, J.A., Marcus, S.C., Olfson, M. (2012). Outpatient Care of Young People After Emergency Treatment of Deliberate Self-Harm. Journal of the American Academy of Child and Adolescent Psychiatry, 51,2, 213-222. Burns, T., Catty, J., White, S., Clement, S., Ellis, G., Jones, I.R., Lissouba, P., McLaren, S., Rose, D., Wykes, T. (2008). Continuity of care in mental health: Understanding and measuring a complex phenomenon. Psychological Medicine, 39, 313-323. Clemens, E.V., Welfare, L.E., Williams, A.M. (2010). Tough Transitions: Mental Health Care Professionals’ Perception of the Psychiatric Hospital to School Transition. Residential Treatment for Children & Youth, 27, 243-263. Page | 20 Transitions Coleman, E.A., Fox, P.D. (2004). One Patient, Many Places: Managing Health Care Transitions, Part I: Introduction, Accountability, Information for Patients in Transition. Annals of Long-Term Care, 12, 9, 25-32. Coleman E.A., Parry C., Chalmers S., Min S.J. (2006). The care transitions intervention: results of a randomized controlled trial. Archives of Internal Medicine, 166, 1822-28. Cotter, J.J., Smith, W.R., Boling, P.A. (2002). Transitions of care: the next major quality improvement challenge. British Journal of Clinical Governance, 7, 3, 198-205. Durbin, J., Goering, P., Streiner, D.L., Pink, G. (2006). Does Systems Integration Affect Continuity of Mental Health Care? Administration and Policy in Mental Health and Mental Health Services Research, 33, 705-717. Haggerty, J.L., Reid, R.J., Freeman, G.K., Starfield, B.H., Adair, C.E., McKendry, R. (2003). Continuity of care: a multidisciplinary review. British Medical Journal, 327, 1219-1221. Law, M., Rosenbaum, P., Jaffer, S., Plews, N., Kertoy, M., & King, S. (2004). Service Coordination for Children and Youth With Complex Needs. CanChild Centre for Childhood Disability Research. Report for the Ministry of Children and Youth Services. McDonald, K.M., Sundaram, V., Bravata, D.M., Lewis, R., Lin N., Kraft, S., McKinnon, M., Paguntalan, H., Owens, D.K. (2007). Care Coordination. Vol 7 of: Shojania, K.G, McDonald, K.M, Wachter, R.M, Owens, D.K, editors. Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies. Technical Review 9 (Prepared by the Stanford University-UCSF Evidence-based Practice Center under contract 290-02-0017). AHRQ Publication No. 04(07)-0051-7. Rockville, MD: Agency for Healthcare Research and Quality. National Transitions of Care Coalition. (2008a).Transitions of Care Measures. Accessed at http://www.ntocc.org/Portals/0/PDF/Resources/TransitionsOfCare_Measures.pdf on August 3, 2012. National Transitions of Care Coalition. (2008b). Improving on Transitions of Care: How to Implement and Evaluate and Plan. Accessed at http://www.ntocc.org/Portals/0/PDF/Resources/ImplementationPlan.pdf on August 3, 2012. Naylor, M. (2006). Transitional Care: A Critical Dimension of the Home Healthcare Quality Agenda. Journal for Healthcare Quality, 28, 1, 20-28. Newton, A.S., Hamm, M.P., Bethell, J., Rhodes, A.E., Bryan, C.J., Tjosvold, L., Ali, S., Logue, E., Manion, I.G. (2010). Pediatric Suicide Related Presentations: A Systematic Review of Mental Health Care in the Emergenc Department. Annals of Emergency Medicine, 56, 6, 649-659. Report of the Paediatric Complex Care Coordination Expert Panel. (2008). Ontario Ministry of Health and Long Term Care. Page | 21 Transitions Rous, B., Hallam, R.A. (2012). Transition Services for Young Children With Disabilities: Research and Future Directions. Topics in Early Childhood Special Education, 31, 4, 232-240. Rous, B., Myers, C.T., Stricklin, S.B. (2007). Strategies for Supporting Transitions of Youth Children with Special Needs and Their Families. Journal of Early Intervention, 30, 1, 1-18. Simon, J.B., Savina, E.A. (2005). Facilitating hospital to school transitions: Practices of hospital-based therapists. Residential Treatment for Children & Youth, 22, 49-66. Steffen, S., Kosters, M., Becker, T., Puschner, B. (2009). Discharge planning in mental health care: a systematic review of the recent literature. Acta Pyschiatrica Scandinavica, 120, 1-9. Transitional Care Model. Accessed at http://www.transitionalcare.info/AbouKeyE-1804.html on August 10, 2012. Trupin, E.J., Kerns, S.E., Cusworth Walker, S., DeRobertis, M.T., Stewart, D.G. (2011). Family Integrated Transitions: A Promising Program for Juvenile Offenders With Co-Occurring Disorders. Journal of Child and Adolescent Substance Abuse, 20, 421-436. Trupin, E. W., Turner, A. P., Stewart, D., & Wood, P. (2004). Transition planning and recidivism among mentally ill juvenile offenders. Behavioral Sciences and the Law, 22, 599–610. U.S. Department of Justice, Office of Juvenile Justice and Delinquency Prevention. OJDDP Model Programs Guide. Reentry. Accessed at www.ojjdp.gov/mpg/reentry.aspx?continuum=reentry on August 6, 2012. Whitson, M.L, Kaufman, J.S., & Bernard, S., (2010). Systems of Care and the Prevention of Mental Health Problems for Children and their Families: Integrating Counseling Psychology and Public Health Perspectives. Prevention in Counseling Psychology, 1, 3(1), 3-9. Wiktorowicz, M.E., Fleury, M.J., Adair, C.E., Lesage, A., Goldner, E., & Peters, S. (2009). Mental health network governance and coordination: Comparative analysis across 10 Canadian regions. International Journal of Integrated Care, 10, e60. Page | 22