Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
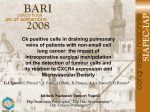
CXCR4 INHIBITION REDUCES BONE METASTASES BY AFFECTING TUMOUR GROWTH AND TUMORIGENIC POTENTIAL IN PROSTATE CANCER PRECLINICAL MODELS. Giovanni Luca GRAVINA1,2, Andrea MANCINI2, Luca VENTURA4, Luca SCARSELLA2, Ana JITARIUC2, Alessandro COLAPIETRO2, Enrico RICEVUTO6, Scott LONNING7, Ernesto DI CESARE1,2, and Claudio FESTUCCIA2 (1) Department of Biotechnological and Applied Clinical Sciences, Division of Radiation Oncology, University of L'Aquila; (2) Department of Biotechnological and Applied Clinical Sciences, Laboratory of Radiobiology, University of L'Aquila; (4) Department of Pathology, Ospedale San Salvatore, L’Aquila; (5) Department of Biotechnological and Applied Clinical Sciences, Division of Medical Oncology, University of L'Aquila; (6) Genzyme Corporation, Oncology Research Area Head. Framingham, MA 01701. Aims. The majority of prostate cancer (PCa) patient morbidity can be attributed to bone metastases posing a significant clinical obstacle. Therefore, a better understanding of this phenomenon is imperative and might help to develop novel therapeutic strategies.I woul like to study the expression of CXCR4 in human prostate cancer patients and its role in bone metastases. Methods. We analyzed the expression of CXCR4 in human tissues from prostate cancers, and tested in vitro and in vivo the capabilities of two CXCR4 receptor antagonists, Plerixafor and CTE9908 to interfere with bone metastasis. Results. Bone-derived PCa cells expressed higher CXCR4 levels than other PCa cell lines; this was also the case in human samples. SDFantagonists reduced PCa cell proliferation and was more effective when PCa were co-cultured with stromal cells, possibly due to the high levels of SDF-9908 delayed tumor growth, reduced angiogenesis and incidence of X-ray detectable bone lesions. Boneassociated tumor growth and associated bone erosion were, indeed, efficiently decreased by CXCR4 antagonist treatment with respect to controls. Kaplan-Meier analyses showed significantly improved overall survival after treatments. The reduced intra-osseous growth of PC3 tumor cells after intratibial injection correlated with decreased osteolysis and serum levels of both mTRAP and type I collagen fragments (CTX). Discussion. Although a growing body of evidence has demonstrated that CXCR4 plays an important role in cancer proliferation, dissemination and invasion and our results seem seem to confirm the role of CXCR4 in bone metastasis formation. Our report is the first in which CXCR4 antagonists have been tested to discern whether the number of tumour cells within bone marrow (intraosseous tumour burden) was a variable related to their effectiveness. Conclusions. In summary, our report provides novel information on the potential activity of CXCR4 inhibitors on the formation and progression of prostate cancer bone metastases and supports this treatment as a useful approach in men with advanced PCa with established metastatic disease or at high risk of bone lesions.