Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
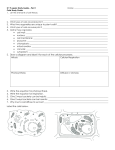
SPRING LIGAMENT • Normally the hindfoot stability and maintenance of the medial longitudinal arch rely on both dynamic and static stabilizers. • Spring ligament is an important static stabilizer for the longitudinal arch of the foot (in conjuntion with the plantar fascia and the superficial fibers of the deltoid ligament). • The main dynamic stabilizer of the ankle is the posterior tibial tendon (PTT). • The spring ligament (plantar calcaneonavicular ligament) serves as a stringlike structure, wrapping under the talar head from its calcaneal origin to its navicular insertion. • When this ligament fails the result is the so-called pes planovalgus deformity or adult-acquired flatfoot deformity. Components of Spring ligament The spring (calcaneonavicular) ligament complex forms the medial and plantar margins of the articular cavity of the head of the talus and has 3 components. v The superomedial is the strongest component. q The inferoplantar longitudinal. ü The medioplantar oblique. Components of Spring ligament The superomedial fascicle extends from the sustentaculum tali to the dorsal aspect of the medial navicular. The posterior tibial tendon lies immediately superficial. This component is usually seen on routine axial and coronal MR images. Axial oblique images of the ankle are also helpful q q The inferoplantar layer extends from the coronoid fossa of the calcaneus just anterior to the sustentaculum tali and inserts at the the inferior beak of the navicular. This component may be seen on coronal routine protocol sequences and particularly performing axial oblique images q The medioplantar component originates at the coronoid fossa of the calcaneus just anterior to the inferoplantar and has a medial oblique course attaching at the medioplantar navicular, just plantar to the navicular tuberosity. It is seldom seen on a routine MR images and it is usually necessary to perform transverse oblique images. Original anatomic illustration of the Spring ligament complex demonstrating their 3 fascicular components with its insertion sites. Original anatomic illustration showing the 3 ligament layers of the Spring ligament complex MRI protocols • We strongly suggest the application of 1.5 or 3 Tesla scanners. • We perform a routine ankle protocol including axial, sagital and coronal T1, T2 and DP FS or STIR sequences with 4-mm slice thickness and 0.4 mm spacing. • We also add transverse oblique images along the sagital plane in order to improve the recognizion of the 3 componentes. If neccessary, we also sum up thin slices. Superomedial portion of Spring ligament complex. STIR weighted axial and sagittal sequences. This fascicle is seen immediately deep to the posterior tibial tendon (arrows) Inferoplantar longitudinal component of the spring ligament complex. Fat suppressed T2 weighted axial oblique image. Medioplantar oblique layer of the spring ligament complex. T1 weighted axial oblique image. TIBIOSPRING LIGAMENT The tibiospring ligament is the anterior, superficial portion of the deltoid ligament complex and fuses with the superior margin of the superomedial layer. PTT SML STIR weighted coronal image and original anatomic illustration showing the posterior tibial tendon and its relations with the superomedial fascicle and the tibiospring component (red arrow) Clinicalpresenta-on • Spring ligament injuries have a high association with posterior tibial tendon tears. They are also most commonly seen in middle-aged women and as a result of chronic degeneration. • Early in the disease process, patients may complain of activity-related pain at the medial ankle and difficulty with balance. Later they mention activity related pain around the sinus tarsi and lateral malleolus, presumably because of impingement of lateral structures. With the development of subtalar osteoarthritis; pain, stiffness, and swelling are present. • Isolated as well as acute injuries of the spring ligament are extremely rare Pathology of the Spring ligament complex • The superomedial (SM) is the most important spring ligament component for providing functional stability of the arch and is also the most frequently injured. • In almost all instances accompanying posterior tibial tendon abnormalities are present. • Published reports give a mean thickness for the SM ranging from 2.5 mm to 4.7mm. In pathologic states it frequently thickens to a level greater than 5 mm. • The most specific finding of a ligament tear is a fluid-signal filled discontinuity of the ligament on T2 or STIR-weighted sequences, representing a tear through the full thickness. They most commonly occur at the distal or proximal attachment sites. • The inferoplantar and medioplantar components are less frequently torn. Of the two, the medioplantar is more susceptible to injury due to its close proximity to the SM. Pathology of SM fascicle of SLC. T2 FS weighted axial and coronal images demonstrates an abnormally lax and thickened superomedial layer along its anterior fibers (arrows). There is also thickening of PTT with increase fluid within the tendon sheath (red arrows). A) B) Pathology of SM fascicle of SLC. A) STIR weighted axial image showing superomedial layer thickening and with signal intensity changes (arrow). B) T2 FS weighted axial image shows similar changes (arrow). Bone marrow edema within the head and body of the astragalus with microtrabecular fractures are also visible (red arrows). Discontinuity of the Spring ligament. STIR weighted axial image showing the superomedial portion diffusely thinned and with a tear at the level of the astragalus neck (arrow). PTT is also affected (red arrow) Avulsion-Tear of superomedial fascicle. PD FS Axial oblique sequence using thin slices showing this layer being detached and thinned near its insertion at the navicular bone (arrow). It is associated with a thickened posterior tibial tendon within a partial tear along the deep surface (arrowhead) Avulsion-Tear of PTT with normal Spring ligament complex. PD FS and T1weighted axial oblique sequences using thin slices demonstrate abnormal thickening and increased signal intensity of the PTT (white arrow) with an avulsion tear at the level of its distal insertion (blue arrow) There is a normal appearance of the superomedial portion of the spring ligament (red arrows), which is seen deep to the posterior tibial tendon. SUMMARY • Posterior tibial tendon tears are a frequent cause of flatfoot deformity. Nevertheless, in many cases, an associated tear of the spring ligament is present. • Spring ligament tears usually involve the superomedial calcaneonavicular ligament portion, which is the most important static stabilizer of the longitudinal arch. • MRI is the modality of choice providing optimal visualization of the spring ligament, having to perform to its best definition specific sequences. • Proper knowledge of anatomy of the spring ligament complex enables the careful MR reader to diagnose its pathology and relation with other structures. • This in turn allows the surgeon to provide a more complete and functional repair of the longitudinal arch.