Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
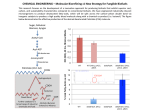
EUROSCAN, a Randomized Trial of Vitamin A and N-Acetylcysteine in Patients With Head and Neck Cancer or Lung Cancer Nico van Zandwijk, Otilia Dalesio, Ugo Pastorino, Nico de Vries, Harm van Tinteren For the European Organization for Research and Treatment of Cancer Head and Neck and Lung Cancer Cooperative Groups Background: Preclinical evidence suggests that retinoids and antioxidants may prevent or delay the occurrence of cancer in the upper or lower airways, but such effects have not been reliably established in clinical studies. To assess the chemopreventive effects of vitamin A (retinyl palmitate) and Nacetylcysteine, we conducted a large randomized intervention study in patients with head and neck cancer or with lung cancer, most of whom had a history of smoking. Methods: From June 1988 through July 1994, a total of 2592 patients (60% with head and neck cancer and 40% with lung cancer) were randomly assigned to receive 1) retinyl palmitate (300 000 IU daily for 1 year followed by 150 000 IU for a 2nd year), 2) N-acetylcysteine (600 mg daily for 2 years), 3) both compounds, or 4) no intervention. All statistical tests were two-sided. Results: Of the patients, 93.5% had smoked tobacco at sometime in their lives (and 25% continued to smoke after cancer diagnosis). After a median follow-up of 49 months, 916 patients were reported with an event (recurrence, second primary tumor, or death). No statistically significant difference was observed in overall survival or eventfree survival between patients who received retinyl palmitate and patients who did not. Similarly, no difference was seen in overall survival or event-free survival between patients who received N-acetylcysteine and patients who did not. There was a lower incidence of second primary tumors in the no intervention arm, but the difference was not statistically significant. Conclusion: A 2-year supplementation of retinyl palmitate and/or N-acetylcysteine resulted in no benefit—in terms of survival, event-free survival, or second primary tumors—for patients with head and neck cancer or with lung cancer, most of whom were previous or current smokers. [J Natl Cancer Inst 2000;92:977–86] The link between tobacco exposure and cancer of the aerodigestive tract, which accounts for more than 30% of all cancer deaths, is indisputable (1,2). Although in recent years smoking prevention and cessation programs have achieved appreciable results, the mortality from aerodigestive tract cancer is still unacceptably high. Therefore, other preventive strategies are urgently needed. Epidemiologic and experimental data (3–5) have suggested that chemoprevention of aerodigestive tract cancer is feasible, but the evidence of a beneficial effect in humans is still limited. Compounds with potential chemopreventive properties, such as retinoids and antioxidants, have been investigated by use of nearly all of the available systems for testing anticarcinogenic activity. Retinoids exert a strong regulatory effect on cell proliferation and differentiation and can inhibit malignant transJournal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 formation and suppress tumor promotion, particularly in the presence of carcinogens from tobacco smoke, such as benzo[a]pyrene (6,7). Tobacco smoke is also a source of oxidative free radicals that can damage DNA (8). Antioxidants have been shown to prevent cellular damage and the subsequent development of cancer by neutralizing free radicals (9,10). Interest has arisen, in particular, in N-acetylcysteine, an aminothiol and synthetic precursor of intracellular cysteine and glutathione, which has been widely used in the past as a mucolytic agent and antidote against paracetamol (acetaminophen)-induced hepatotoxicity. NAcetylcysteine has proven to be effective in decreasing the direct mutagenicity of several chemical compounds by inhibiting the in vivo formation of carcinogen–DNA adducts, DNA damage, and urethane-induced lung tumors in mice (11–13). The EUROSCAN Study (i.e., the European Study on Chemoprevention With Vitamin A and N-Acetylcysteine) was designed to test whether vitamin A (retinyl palmitate) and Nacetylcysteine could improve the prognosis of patients treated for head and neck cancer or for lung cancer by preventing second primary tumors (14). Both categories of patients have a high risk of developing a second cancer and represent a relevant population for secondary preventive measures (15). Two earlier, albeit relatively small, studies of 13-cis-retinoic acid and retinyl palmitate in the same groups of patients (16,17) suggested that these agents had protective activity, but large randomized chemoprevention trials with vitamin A and -carotene in smokers (18,19) failed to show any preventive effect. PATIENTS AND METHODS Study Design The two agents studied have different mechanisms of action, and the combination was judged to be feasible without dose reductions or delays. A two-bytwo factorial design was chosen to allow the simultaneous investigation of retinyl palmitate and N-acetylcysteine. Initially, the EUROSCAN Study also included a pilot study on the effectiveness of six monthly bronchoscopies as a screening tool for patients with laryngeal cancer. This part of the study was closed because only a minority of patients agreed to participate (20). Participants were randomly assigned to one of the following four arms: 1) retinyl palmitate alone (300 000 IU daily for 1 year followed by 150 000 IU for Affiliations of authors: N. van Zandwijk, O. Dalesio, H. van Tinteren, The Netherlands Cancer Institute, Amsterdam; U. Pastorino, European Institute of Oncology, Milan, Italy; N. de Vries, St. Lucas Hospital, Amsterdam. Correspondence to: Nico van Zandwijk, M.D., Ph.D., The Netherlands Cancer Institute, Plesmanlaan 121, 1066 CX Amsterdam, The Netherlands (e-mail: [email protected]). See “Appendix” section for list of participants in the EUROSCAN Study. See “Notes” following “References.” © Oxford University Press ARTICLES 977 the 2nd year), 2) N-acetylcysteine alone (600 mg daily for 2 years), 3) the combination of retinyl palmitate (300 000 IU daily for 1 year followed by 150 000 IU for the 2nd year) and N-acetylcysteine (600 mg daily for 2 years), or 4) no intervention (Fig. 1). The possibility of a placebo-controlled study was discarded after considering the cost aspects and the distinct characteristics (smell and side effects) of the two agents in the double-blind approach. Randomization by the minimization technique (21) was performed centrally by the European Organization for Research and Treatment of Cancer (EORTC) Data Center. The patients were stratified according to institution, sex, smoking (all tobacco) history (smokers versus nonsmokers and never smokers), previous therapy (surgery, radiotherapy, or chemotherapy), and histology and location of the primary tumor (larynx, oral cavity, or lung). Patient Eligibility To be eligible for the study, patients had to have non-small-cell lung cancer (stages pT1–2, N0–1, and T3N0, according to the 1987 edition of the tumor– node–metastasis [TNM] staging system, published by the Union Internationale Contre le Cancer (22), cancer of the larynx (Tis, T1–3, and N0–1), or cancer of the oral cavity (T1–2 and N0–1); had to have a performance status (World Health Organization [WHO]) 0–2; and had to be treated with curative intent. Patients with recurrent disease, synchronous multiple tumors, previous malignant disease, abnormal liver or renal function, hypertriglyceridemia, hypercholesterolemia, diabetes mellitus, hypertension, and recent or active peptic ulcer were considered to be unsuitable for the study. Informed consent from all patients was to be obtained according to institutional regulations. From June 1988 through July 1994, a total of 2592 patients (60% with head and neck cancer and 40% with lung cancer) from 81 institutions in 15 countries were randomly assigned. Evaluation of End Points Minimal follow-up requirements during the first 2 years after randomization consisted of three monthly follow-up visits, with chest x-rays every 6 months. For patients with laryngeal cancer, ear, nose, and throat examinations included repeated laryngoscopies. For patients with oral cancer, follow-up investigations included inspection of the oral cavity; no routine laryngoscopy was performed in this category of patients. From years 3 through 10 after randomization, follow-up was scheduled at 6-month intervals and chest x-rays were scheduled yearly. At every follow-up visit, patients were asked about pill intake, side effects, concomitant medications, and smoking habits. Patients taking retinyl palmitate were regularly checked for levels of serum enzymes, cholesterol, and triglycerides. Primary end points were event-free survival, overall survival, and the occurrence of a second primary tumor. Carcinomas of the head and neck, lung, esophagus, and urinary bladder were considered to be tobacco-related second primary tumors. The study coordinators reviewed all first events. When inconsistencies or doubts arose, additional information was requested from the responsible physician, and the study coordinators discussed the case until a consensus was reached. Statistical Considerations The sample size was chosen to provide 90% power to detect a decrease from 10% to 5% in the rate of (tobacco-related) second primary tumors at 5 years (significance level ⳱ .05; two-sided log-rank test). The number was increased to take into account a possible dilution effect caused by 10% crossing-over (e.g., 10% of the patients randomly assigned to retinyl palmitate not taking their pills and 10% of the patients assigned to the no retinyl palmitate arms taking retinyl palmitate). With continuous follow-up, sufficient number of events (recurrences, second primary tumors, and deaths) would be observed to allow the detection of a 20% reduction in the hazard ratios with 80% power (significance level ⳱ .05; two-sided log-rank test). Therefore, at least 2000 patients were to be entered and followed for at least 5 years (500 patients per arm). In the factorial design, the effect of N-acetylcysteine could be evaluated by comparing patients randomly assigned to receive N-acetylcysteine (half with retinyl palmitate and half without retinyl palmitate) with patients randomly assigned not to receive N-acetylcysteine (half with retinyl palmitate and half without retinyl palmitate). This comparison was done by stratifying by the presence or absence of retinyl palmitate. In a similar way, the effect of retinyl palmitate was evaluated by stratifying by the presence or absence of Nacetylcysteine. Event-free survival, time to second primary tumor, and survival curves were constructed by the Kaplan–Meier technique (23) and were compared by the log-rank test (24). The interaction between the effects of N-acetylcysteine and those of retinyl palmitate was tested with a proportional hazards model. Also, analyses of four arms were performed. All analyses were intention-to-treat analyses. All statistical tests were two-sided, and P values of results referred to as statistically significant were less than .05. RESULTS Patients Fig. 1. CONSORT diagram. 978 ARTICLES Of the 2592 patients who were randomly assigned, 19 (0.7%) were excluded from all tables and analyses because no information was received after registration as depicted in the CONSORT diagram (Fig. 1). Of the remaining 2573 patients, 1290 were assigned to retinyl palmitate arms (647 to retinyl palmitate alone and 643 to retinyl palmitate and N-acetylcysteine) and 1283 were assigned to no retinyl palmitate arms (641 to no treatment and 642 to N-acetylcysteine alone). The same patients can also be grouped with respect to treatment with N-acetylcysteine as follows: 1285 patients were assigned to N-acetylcysteine arms, and 1288 patients were assigned to no N-acetylcysteine arms. Table 1 shows the characteristics of patients as a function of treatment. Sixty percent of the patients had head and neck cancer (1065 patients had laryngeal cancer, and 485 had oral cancer), and 40% (1023 patients) had lung cancer. The majority of patients had been treated for a stage I tumor. The median age was 61 years, 13.0% were female, and 6.5% reported that they had never smoked. In the majority of patients, the primary treatment consisted of surgery alone or surgery in combination with raJournal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 Table 1. Patient characteristics at randomization and treatment Treatment* Patient characteristics at randomization Total No. (%) Retinyl + NAC Retinyl NAC No drugs Total No. of patients Male Female 643 560 83 647 563 84 642 556 86 641 559 82 Median age, y (range) 61 (23–83) 61 (23–83) 61 (28–86) 60 (19–91) 601 42 605 42 598 44 601 40 2405 (93.5) 168 (6.5) 150 74 41 143 88 39 134 87 47 127 97 38 554 (52.0) 346 (32.5) 165 (15.5) 47 55 21 56 41 26 40 50 30 51 48 20 194 (40.0) 194 (40.0) 97 (20.0) 179 53 23 196 38 20 197 39 18 204 37 19 776 (75.9) 167 (16.3) 80 (7.8) Prior treatment, No. of patients‡ Surgery RT Surgery + RT 357 202 84 376 184 87 370 183 89 372 177 92 1475 (57.3) 746 (29.0) 352 (13.7) Months between treatment and randomization Unknown <2 2–12 >12 316 230 97 331 209 107 1 337 194 110 314 219 108 1 (0.0) 1298 (50.4) 852 (33.1) 422 (16.4) No. of former/current smokers No. of never smokers Site of tumor, No. of patients† Larynx Stage I Stage II Stage III Oral cavity Stage I Stage II Stage III Lung Stage I Stage II Stage III 2573 2238 (87.0) 335 (13.0) 61 (19–91) *Retinyl ⳱ retinyl palmitate; NAC ⳱ N-acetylcysteine. †According to tumor–node–metastasis (TNM) classification (Union Internationale Contre le Cancer, 1987). ‡Eighty-seven patients (3.4%) received chemotherapy in addition to local treatment (mainly before surgery). RT ⳱ radiation therapy. diotherapy. A minority (3.4%) of patients received chemotherapy in addition to local treatment. Half of the patients were enrolled in the study shortly after treatment (within 2 months), and 16.4% of the patients had been treated for longer periods before randomization (>12 months). Follow-up In total, more than 19 000 control visits were reported. Seventy-seven percent of these visits were on schedule. The mean follow-up intensity (calculated per patient as the number of days in follow-up divided by the number of follow-up visits) was 189 days in the combined arm, 179 days in the retinyl palmitate alone arm, 186 days in the N-acetylcysteine alone arm, and somewhat longer (193 days) in the no treatment arm. The total follow-up was 8923 person-years (person-years ⳱ the total observation time added over all subjects, expressed in years) and was well balanced across treatment arms (2213 years in the retinyl palmitate alone arm, 2249 years in the retinyl palmitate and N-acetylcysteine arm, 2230 years in the N-acetylcysteine alone arm, and 2232 years in the no treatment arm). The year of last follow-up was distributed similarly across treatment arms. Of the 93.5% of the patients who enrolled in the study with a smoking history, 25% continued to smoke after the diagnosis (9.4% admitted that they continued to smoke, and 15.6% reported periods when they resumed smoking) and 72.3% had permanently stopped (no information was obtained for 2.7% of the patients). These percentages were similar in all four arms of the study. Journal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 Compliance, Side Effects, and Concomitant Medication Of the 1932 patients randomly assigned to receive trial medication, 444 (23%) did not complete the intended 2-year intervention period. Of the 643 patients randomly assigned to receive retinyl palmitate and N-acetylcysteine, 162 (25.2%) stopped treatment; of the 647 patients randomly assigned to receive retinyl palmitate only, 167 (25.8%) stopped treatment; and of the 642 patients randomly assigned to receive N-acetylcysteine only, 115 (17.9%) stopped treatment. Stopping treatment was more frequent in the two groups assigned to retinyl palmitate (P<.001). For 250 (13%) of 1932 patients, the drug intake was recorded as being irregular at least once during the 2-year intervention. Overall, retinyl palmitate elicited more side effects than Nacetylcysteine (P<.001). Side effects were reported by 45% of the patients in the two retinyl palmitate arms and by 24% of the patients in the N-acetylcysteine alone arm. Typical side effects of retinyl palmitate were mucocutaneous (dryness, desquamation, itching, bleeding, and hair loss). Side effects of the Nacetylcysteine arms were more frequently related to the digestive tract (mainly dyspepsia). Severe side effects were also more frequent in the retinyl palmitate arms (Table 2). On a few occasions, “other” side effects (e.g., anemia, dizziness, dyspnea, mental symptoms, chills, diffuse pain, and vertigo) were reported. These effects, however, were considered to be unrelated to the study medication. Co-medication was recorded on the follow-up forms of 52% ARTICLES 979 Table 2. Worst degree of toxicity per patient* Treatment Retinyl + NAC Type of toxocity Gastrointestinal Skin Malaise Transient liver enzyme elevation Hypercholesterolemia Bone pain Other Retinyl NAC Grade 3 Grade 4 Total No. Grade 3 Grade 4 Total No. Grade 3 Grade 4 Total No. Grand total No. 22 23 — — 1 1 3 25 20 1 3 2 1 5 47 43 1 3 3 2 8 13 28 1 — — 2 10 19 22 4 2 2 — 5 32 50 5 2 2 2 15 19 5 1 1 — — 2 25 6 1 — — — 1 44 11 2 1 — — 3 123 104 8 6 5 4 26 *Retinyl ⳱ retinyl palmitate; NAC ⳱ N-acetylcysteine. of the patients. From these 1338 patients, a sample of 342 (26%), balanced for treatment groups and institution, was selected. The names of the co-medications were translated into generic terms according to the Anatomical Therapeutic Chemical Classification (25), and the co-medications were labeled if they belonged to a category with chemopreventive potential (vitamins, various brands of N-acetylcysteine, and other antioxidants). Of all the medications specified, 129 of 3125 compounds were found to belong to the same category as the study drugs (antioxidants or vitamin A-like). Within the sample, 15 (4%) of 342 patients were taking these co-medications. Event-Free Survival, Overall Survival, and Second Primary Tumors At 5 years, 58% of the patients with lung cancer, 83% of the patients with cancer of the larynx, and 77% of the patients with oral cancer were alive (Fig. 2). Fig. 3 presents the survival curves for groups that did or did not receive N-acetylcysteine and for groups that did or did not receive retinyl palmitate. There were 328 deaths in the groups that received N-acetylcysteine and 304 deaths in the groups that did not. There were 318 deaths in the groups that received retinyl palmitate and 314 deaths in the groups that did not. For both compounds, no statistically significant differences in survival Fig. 2. Overall survival by site of the primary tumor. 980 ARTICLES were detected (P = .925). The statistical test for interactions was not statistically significant, indicating that the effect of retinyl palmitate on survival did not depend on the presence or absence of N-acetylcysteine. Comparison of survival curves, considering the four arms of the study as separate groups, also did not show statistically significant differences. Table 3 summarizes the first events (recurrence, second primary tumor, or death) observed in the four arms. A total of 632 patients were reported dead. Among the 1290 patients randomly assigned to receive retinyl palmitate, there were 465 first events; among the 1283 patients assigned to receive no retinyl palmitate, there were 451 first events. Among the 1285 patients assigned to receive N-acetylcysteine, there were 468 first events; among the 1288 patients assigned to receive no N-acetylcysteine, there were 448 first events. After a median follow-up of 49 months, 916 (36%) of the 2573 patients were reported with at least one event. In 133 (15%) patients, the first event was death. In 572 (62%) patients, the first event was tumor recurrence. In 211 (23%) patients, the first event was a second primary tumor (116 in the N-acetylcysteine groups, 95 in the no N-acetylcysteine groups, 115 in the retinyl palmitate groups, and 96 in the no retinyl palmitate groups). In five of these patients, however, even after re-evaluation, it remained unclear whether the event was a second primary tumor or a recurrence of disease. In 154 patients (83 in the N-acetylcysteine groups, 71 in the no N-acetylcysteine groups, 77 in the retinyl palmitate groups, and 77 in the no retinyl palmitate groups), the second primary tumor was tobacco related. Twenty-nine additional second primary tumors were reported after recurrence of disease (six in the group receiving retinyl palmitate and N-acetylcysteine, seven in the group receiving retinyl palmitate, seven in the group receiving N-acetylcysteine, and nine in the group receiving no intervention). There was a lower, but not statistically significant, incidence of second primary tumors in the no intervention arm. The incidence rate for all second primary tumors was 0.027 per person per year, and the rate for tobacco-related second primary tumors was 0.019 per person per year. Table 4 summarizes the type of second primary tumor as first event by the site of the primary tumor. The most frequent sites for second primary tumor were the lung and the head and neck regions. Event-free survival curves are preJournal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 a second primary tumor from recurrent disease, analyses of time until local failure or second primary tumor were also performed. These analyses revealed no statistically significant differences when all four arms were considered individually or two by two. Analyses considering all second primary tumors, regardless of whether they occurred as a first event or after a recurrence, gave similar results (log-rank test for the global comparison of the four arms, P = .054). In an attempt to consider actual drug intake, the same analyses were also performed by taking into account compliance as baseline covariates. These analyses showed consistently similar results, suggesting that lack of compliance did not play a major role in the negativity of the results. Event-free survival, survival, and time to second primary tumor were compared by treatment (N-acetylcysteine versus no N-acetylcysteine and retinyl palmitate versus no retinyl palmitate) within subgroups. The subgroups were defined by the presence or absence of the other treatment, site of disease, prior treatment, performance status, sex, smoking habits, and interval between treatment of the primary tumor and random assignment. These analyses should be considered exploratory because they were not planned before the study was initiated. For the groups receiving N-acetylcysteine, the hazard ratios of event-free survival, survival, and tobacco-related second primary tumor are summarized in Fig. 5, A–C. For the groups receiving retinyl palmitate or no retinyl palmitate, the hazard ratios of event-free survival, survival, and tobacco-related second primary tumor are summarized in Fig. 5, D–F. The confidence intervals for all subgroups cross the no-effect line, indicating Fig. 3. A) Overall survival by treatment (N-acetylcysteine [NAC] versus no N-acetylcysteine). B) no differences beyond what could be consistent with chance for these groups. In addition, analyOverall survival by treatment (retinyl palmitate [retinyl] versus no retinyl palmitate). ses by stage of disease within the three tumor sites were performed and did not suggest any sented in Fig. 4. No statistically significant differences were particular heterogeneity of results (data not shown). observed when analyzed according to the factorial design (Nacetylcysteine versus no N-acetylcysteine, P ⳱ .631; retinyl DISCUSSION In contrast to expectations, the EUROSCAN Study has not palmitate versus no retinyl palmitate, P ⳱ .672) or when analyzed by the four separate arms (P ⳱ .750), and no statistically shown any benefit for a 2-year supplementation with retinyl significant interaction was found between retinyl palmitate and palmitate and/or N-acetylcysteine in a population at risk for second primary tumors and tumor recurrences in the upper and N-acetylcysteine (P ⳱ .365). Log-rank test results of time to second primary tumor and lower airways. This population was predominantly made up of time to tobacco-related second primary tumor for N- former or current smokers. This observation was made when the acetylcysteine versus no N-acetylcysteine stratifying for retinyl whole group was analyzed or when patients with head and neck palmitate were not statistically significantly different (P ⳱ .190 cancer or lung cancer were analyzed separately. The 2-year duand P ⳱ .394, respectively). Similar results were found for ration of the intervention and the dosage of the trial medications retinyl palmitate versus no retinyl palmitate stratifying for N- appear appropriate, considering that the relatively large number acetylcysteine (P ⳱ .173 and P ⳱ .978, respectively). The tests of patients experiencing side effects resulted in approximately a for interactions were, however, statistically significant (P ⳱ quarter of the patients not completing the 2-year intervention .012 and P ⳱ .039, respectively). When all four arms were period. No statistically significant differences in survival or considered, the number of second primary tumors (tobacco- event-free survival were found between the patients when those related and overall) was lower in the control group (log-rank receiving retinyl palmitate were compared with those receiving tests for the global comparisons of four arms P ⳱ .174 and P ⳱ no retinyl palmitate, when those receiving N-acetylcysteine were .025, respectively). Considering the difficulties in differentiating compared with those receiving no N-acetylcysteine, and when Journal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 ARTICLES 981 Table 3. Events by treatment* Retinyl + NAC Follow-up status No. % No. of patients 643 No. of deaths 161 No. of patients with at least one event Retinyl NAC No. % 100.0 647 25.0 157 231 35.9 78 60 10 54 35 29 Type of first event, No. of patients Local/regional recurrence Distant metastases Local recurrence + distant metastases SPT† Local recurrence + SPT Tobacco-related SPT (% from SPTs) Death No drugs No. % 100.0 642 24.3 167 234 36.2 33.8 26.0 4.3 23.4 92 39 7 61 39.3 16.7 3.0 26.1 64.8 12.6 42 35 68.9 15.0 Total No. % No. % 100.0 641 100.0 2573 100.0 26.0 147 22.9 632 24.6 237 36.9 214 33.4 916 35.6 68 53 16 61 1 48 38 28.7 22.4 6.8 25.7 0.4 77.4 16.0 93 45 11 32 2 29 31 43.5 21.0 5.1 15.0 0.9 85.3 14.5 331 197 44 208 3 154 133 36.1 21.5 4.8 22.7 0.3 73.0 14.5 *The numbers according to the factorial design (N-acetylcysteine [NAC] versus no NAC and retinyl palmitate [retinyl] versus no retinyl palmitate) can be obtained by adding the appropriate columns of Table 4. †STP ⳱ second primary tumor. Table 4. Site of second primary tumor as first event by the site of the initial tumor Site of initial tumor Larynx Oral cavity Lung No. % No. % No. Total 88 100.0 50 100.0 73 Tobacco-related SPTs* Head and neck Esophagus Lung Urinary bladder Kidney Unknown 16 3 37 2 1 18.2 3.4 42.0 2.3 1.1 22 2 16 44.0 4.0 32.0 8 1 39 5 1 11.0 1.4 53.4 6.8 1.4 1 2.0 46 6 92 7 2 1 21.8 2.8 43.6 3.3 0.9 0.5 5 1 10.0 2.0 12 16.4 1 1 1 2.0 2.0 2.0 1 2 1.4 2.7 4 5.5 27 3 9 5 1 12 12.8 1.4 4.3 2.4 0.5 5.7 Other SPTs Gastrointestinal Nasal cavity Lymphoma/leukemia Breast Soft-tissue sarcoma Prostate 10 2 8 2 11.4 2.3 9.1 2.3 7 8.0 % Total No. % 100.0 211 100.0 *SPT ⳱ second primary tumor. those in the four treatment groups were considered separately. The distribution of end points according to the four arms (Table 4) revealed a lower incidence of second primary tumors in the no intervention group compared with the intervention arms. The lower incidence of second primary tumors appears to be counterbalanced by a higher frequency of relapses and could perhaps also be partly explained by the lower follow-up frequency in the no intervention arm. The incidence of second primary tumors in the EUROSCAN Study was approximately what was described in previous series of patients (15,26), with the exception of a recent report (27) on a similar group of patients with lung cancer who had a considerably higher rate. Differentiation between second primary tumors and recurrences (especially when the new lesion occurs near the original tumor site) or between second primary tumor and solitary metastasis (in case of similar histology) is difficult and sometimes impossible (15). Ideally for a definite diagnosis, new molecular methods (28) should have been used. However, this technology was not yet available for implementation in a large multicenter trial, such as the EUROSCAN Study. Al982 ARTICLES though all first events in the study were centrally reviewed, a certain degree of misclassification cannot be excluded. Therefore, emphasis was put on incontestable end points, such as overall survival and event-free survival. Results of the EUROSCAN Study do not confirm the positive outcomes of previous studies with retinyl palmitate (17) and 13-cis-retinoic acid (16), suggesting preventive activity in patients who have had non-small-cell lung cancer or head and neck cancer treated with curative intent. These studies were small and had a shorter follow-up (32 and 46 months versus 49 months) and a shorter intervention period. Two other relatively small studies (29,30) in which patients with head and neck cancer were treated with retinoids (retinyl palmitate and etretinate) have also failed to show a decrease in the number of second primary tumors. It is, therefore, not surprising that doubt about the potential of vitamin A to prevent cancer has increased (31). Other large-scale prevention studies in noncancer populations have pointed to the complexity of the chemoprevention approach. An unexpected high frequency of lung cancer was found in the intervention arms of two major placebo-controlled trials of -carotene in populations of predominantly cigarette smokers— the Alpha-Tocopherol, Beta-Carotene (ATBC) Cancer Prevention Study and the Beta-Carotene and Retinol Efficacy Trial (CARET) (18,19). In a third large double-blind study of 22 071 healthy males, who were mainly nonsmokers, again no preventive effect of long-term (12 years) supplementation with -carotene was observed (32). In this study, an increased incidence of lung cancer associated with -carotene prescription was not observed, which led to the conclusion that -carotene might elicit adverse effects only in smokers (33). Recent animal experiments (34) seem to confirm this suggestion. In addition, in the EUROSCAN Study, a negative effect of the prescription of retinyl palmitate or N-acetylcysteine on the incidence of second primary tumors cannot be excluded. The fact that fewer second primary tumors were seen when the N-acetylcysteine and retinyl palmitate were combined, however, suggests an artifact, perhaps caused by the multiplicity of analyses and a consequent increase in the probabilities of error. In the 1980s when the EUROSCAN Study was planned, comparative trials with traditional clinical end points were considered the best means to test candidate chemopreventive agents. In the light of current knowledge, it might be questioned at what Journal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 Data management and statistics: A. Kirkpatrick (European Organization for Research and Treatment of Cancer [EORTC] Data Center, Brussels, Belgium); O. Dalesio, J. Dijkstra, and H. van Tinteren (The Netherlands Cancer Institute, Amsterdam); and R. Parentela (Istituto dei Tumori, Milan, Italy) Advisor: S. Piantadosi (The Johns Hopkins Hospital, Baltimore, MD) The study took place during the chairmanships of G. B. Snow and J.-L. Lefebvre (EORTC Head and Neck Cooperative Group) and J. G. McVie, N. van Zandwijk, and G. Giaccone (EORTC Lung Cancer Cooperative Group). The participants who collaborated in the EUROSCAN Study are, in order of number of patients accrued in the study, as follows: G. B. Snow, M. P. Copper, and N. de Vries (Free University, Amsterdam, The Netherlands); G. J. Hordijk and H. Lubsen (Academic Hospital, Utrecht, The Netherlands); U. Pastorino, C. Grandi, M. Infante, and P. Salvatori (Ist Nazionale per la studio dei Tumori, Milan, Italy); F. J. M. Hilgers, A. J. M. Balm, and N. van Zandwijk (The Netherlands Cancer Institute, Amsterdam); J. Jerman (University of Ljubljana, Slovenia); I. Spasova (Institute of Respiratory Diseases, Prague, Czechoslovakia); R. G. J. R. A. Vanderschueren (St. Antonius Ziekenhuis, Nieuwegein, The Netherlands); F. Lunghi (Monselice Hospital, Padua, Italy); J. Castella (Hospital de la Santa Creu I Sant Pau, Barcelona, Spain); G. Chiesa and M. Maioli (Ospedale Niguarda Ca Granda, Milan, Italy); G. P. M. ten Velde (Academic Hospital Maastricht, The Netherlands); M. Maffioli and R. Piantanida (Ospedale di Circolo, Varese, Italy); H. Maier (Universität Heidelberg, Germany); H. Szpirglas (Centre Hospitaliere Universitaire Pitié Salpétrière, Paris, France); J. P. van Meerbeeck (Universitair Ziekenhuis Antwerpen, Edegem, Belgium); A. Dundar (Gulhane M. Medical Academy, Ankara, Turkey); J. Pawlega, M. Krzysztof, and K. Krzemieniecki (Institut Onkologii, Krakow, Poland); P. Giannobi (Nuovo Ospedale San Gerardo, Monza, Italy); L. Barzan (Centro di Riferimento Oncologico, Aviano Pordenone, Italy); E. Jassem (Medical Academy of Fig. 4. A) Time to first event by treatment (N-acetylcysteine [NAC] versus no N-acetylcysteine). Gdánsk, Poland); Z. Skacel (2nd Clinic for TuberB) Time to first event by treatment (retinyl palmitate [retinyl] versus no retinyl palmitate). culosis and Chest Diseases, Prague, Czechoslovakia); V. M. S. A. Vieira (Hospital Pulido Valente, Lisbon, stage large-scale, randomized studies should be initiated. Recent Portugal); M. Virag (Klinici Bolnicki Centar, Zagreb, Croatia); G. developments in molecular biology have provided the opportu- Andry (Institut Jules Bordet, Brussels, Belgium); F. M. L. H. G. Palmen nity for carefully designed developmental protocols through (St. Elizabeth Ziekenhuis, Tilburg, The Netherlands); C. Domenge (Inwhich potential chemopreventive agents could be guided stitute Gustave Roussy, Villejuif, France); F. Cianfriglia (Istituto through phase I and II studies using intermediate end points that Regina Elena, Rome, Italy); G. Scagliotti (Universita di Torino, Orbassano, Italy); S. Staemars (Mutterhaus der Borromaerinnen, Trier, could lead to a more rational selection of agents for comparative Germany); A. Personeni (Ospedali Riuniti di Bergamo, Italy); T. S. van studies (35). der Werf (Akademisch Ziekenhuis, Groningen, The Netherlands); Carcinogenesis is a multistep process occurring over many C. Berardi (Ospedale di Garbagnate Milanese, Milan, Italy); P. Drings years, with a latent period (i.e., the period between the start of (Thoraxklinik Rohrbach, Heidelberg, Germany); B. Cottier (Clattercarcinogenesis and the occurrence of clinical cancer) that has bridge Hospital, Merseyside, U.K.); K. Bujko (Oncology Centre Instibeen estimated to be at least 10 years long. Therefore, subjects tute, Warszawa, Poland); G. Ralza (Clinica ORL, Trieste, Italy); S. J. in cancer prevention trials, such as the EUROSCAN Study, Brockmeier (Klinikum rechts der Isar, Munich, Germany); T. Lewinski should be followed for periods of at least 10 years to reach (M. Slodowska-Curie Cancer Center, Warszawa, Poland); P. Espana (Clinica Puerta de Hierro, Madrid, Spain); R. Bastus (Hospital de definite conclusions. Mutua de Terrassa, Barcelona, Spain); A. Ravaioli and E. Pasquini APPENDIX: PARTICIPANTS IN THE EUROSCAN STUDY (Ospedale Civile Rimini Div Oncologia, Italy); M. Clerici (Ospedale San Carlo Borromeo, Milan, Italy); J.-M. Brechot (Hôtel-Dieu de Study coordinators: U. Pastorino (European Institute of Oncology, Paris, France); W. Bergler (Klinikum der stadt Mannheim, Germany); Milan, Italy), N. de Vries (St. Lucas Hospital, Amsterdam, The Neth- J.-L. Lefebvre (Centre Oscar Lambert, Lille, France); G. S. Kho erlands), and N. van Zandwijk (The Netherlands Cancer Institute, Am- (Dijkzigt Hospital, Rotterdam, The Netherlands); J. Dolensky (Thosterdam). mayer’s Teaching Hospital, Prague, Czechoslovakia); F. van Breukelen Journal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 ARTICLES 983 Fig. 5. A–C) Event ratios by treatment (N-acetylcysteine [NAC] versus no N-acetylcysteine) within subgroups of patients. A) First event. B) Mortality. C) Second primary cancer (tobacco related). For each subgroup and each end point, the ratio of the appropriate hazard rates of the treatment (N-acetylcysteine) versus the control (no Nacetylcysteine) is plotted as a solid square. Its size is proportional to the amount of information concerned, so that subgroups with more patients and events are represented by larger squares. The vertical lines correspond to ratios of 1.0 that appear when results of treatment and control are similar. Ranges smaller than 1.0 (to the left of the vertical lines) are compatible with better results in the treatment arm; ranges larger than 1.0 favor the control arm. A confidence interval (99% for each subgroup) is depicted for every ratio as a horizontal line through the square. If a confidence interval contains the 1.0, then the vertical 1.0 line and the confidence interval line cross and the comparison of treatment results in the particular group is not statistically significant at 1%. This level of significance was chosen to take into account the increased probability of error due to multiple testing. The overall result of N-acetylcysteine versus no N-acetylcysteine and its 95% confidence interval is plotted as a diamond. D–F) Event ratios by treatment (retinyl palmitate [retinyl] versus no retinyl palmitate) within subgroups of patients. D) First event. E) Mortality. F) Second primary cancer (tobacco related). Obs ⳱ observed events; Exp ⳱ expected events; O – E ⳱ observed minus expected; CI ⳱ confidence interval; RT ⳱ radiation therapy; PS ⳱ Eastern Cooperative Oncology Group/World Health Organization performance status. **Time since treatment of primary tumor. 984 ARTICLES Journal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 Journal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000 ARTICLES 985 (Spaarne Ziekenhuis, Haarlem, The Netherlands); and X. Panis (Centre Jean Godinot, Reims, France). (22) REFERENCES (23) (1) Peto R, Lopez AD, Boreham J, Thun M, Heath C Jr. Mortality from tobacco in developed countries: indirect estimation from national vital statistics. Lancet 1992;339:1268–78. (2) Peto R, Lopez AD, Boreham J, Thun M, Heath C, Doll R. Mortality from smoking worldwide. Br Med Bull 1996;52:12–21. (3) Fontham ET. Protective dietary factors and lung cancer. Int J Epidemiol 1990;19 Suppl 1:S32–42. (4) Hong WK, Endicott J, Itri LM, Doos W, Batsakis JG, Bell R, et al. 13cis-Retinoic acid in the treatment of oral leukoplakia. N Engl J Med 1986; 315:1501–5. (5) Lippman SM, Batsakis JG, Toth BB, Weber RS, Lee JJ, Martin JW et al. Comparison of low-dose isotretinoin with beta carotene to prevent oral carcinogenesis. N Engl J Med 1993;328:15–20. (6) Taylor Mayne S, Lippman SM. Retinoids and carotenoids. In: De Vita VT Jr, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. Philadelphia (PA): Lippincott-Raven; 1997. p. 585–98. (7) Lotan R. Effects of vitamin A and its analogs (retinoids) on normal and neoplastic cells. Biochim Biophys Acta 1980;605:33–91. (8) Pryor WA. Cigarette smoke radicals and the role of free radicals in chemical carcinogenicity. Environ Health Perspect 1997;105 Suppl 4:875–82. (9) Stone KK, Bermudez E, Pryor WA. Aqueous extracts of cigarette tar containing the tar free radical cause DNA nicks in mammalian cells. Environ Health Perspect 1994;102 Suppl 10:173–8. (10) Kensler TW. Chemoprevention by inducers of carcinogen detoxication enzymes. Environ Health Perspect 1997;105 Suppl 4:965–70. (11) De Flora S, Cesarone CF, Balansky RM, Albini A, D’Agostini F, Bennicelli C, et al. Chemopreventive properties and mechanisms of NAcetylcysteine. The experimental background. J Cell Biochem Suppl 1995; 22:33–41. (12) Van Zandwijk N. N-Acetylcysteine (NAC) and glutathione (GSH): antioxidant and chemopreventive properties, with special reference to lung cancer. J Cell Biochem Suppl 1995;22:24–32. (13) van Zandwijk N, Maas LM, Breedijk A, Godschalk RW, Sakai H, Wigbout G, et al. Aromatic DNA adduct levels in alveolar macrophages and lymphocytes of smoking volunteers: effects of N-acetylcysteine (NAC) supplementation [abstract]. Proc Am Assoc Cancer Res 1997;38:371. (14) de Vries N, van Zandwijk N, Pastorino U. The EUROSCAN Study. EUROSCAN Steering Committee. Br J Cancer 1991;64:985–9. (15) de Vries N. The magnitude of the problem. In: de Vries N, Gluckman JL, editors. Multiple primary tumors in head and neck. Stuttgart (Germany): Thieme; 1990. p. 1–25. (16) Hong WK, Lippman SM, Itri LM, Karp DD, Lee JS, Byers RM, et al. Prevention of second primary tumors with isotretinoin in squamous-cell carcinoma of the head and neck. N Engl J Med 1990;323:795–801. (17) Pastorino U, Infante M, Maioli M, Chiesa G, Buyse M, Firket P, et al. Adjuvant treatment of stage I lung cancer with high-dose vitamin A. J Clin Oncol 1993;11:1216–22. (18) The Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med 1994;330:1029–35. (19) Omenn GS, Goodman GE, Thornquist MD, Balmes J, Cullen MR, Glass A, et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N Engl J Med 1996;334:1150–5. (20) Rachmat L, Vreeburg GC, de Vries N, Hordkjk GJ, Lubsen H, Manni JJ, et al. The value of twice yearly bronchoscopy in the work-up and follow-up of patients with laryngeal cancer. Eur J Cancer 1993;29A:1096–9. (21) Pocock SJ, Simon R. Sequential treatment assignment with balancing for 986 ARTICLES (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) prognostic factors in the controlled clinical trial. Biometrics 1975;31: 103–15. Hermanek P, Sobin LH, editors. TNM Classification of Malignant Tumors, 4th fully revised ed. Berlin (Germany): Springer-Verlag; 1987. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;53:457–81. Peto R, Pike MC, Armitage P, Breslow NE, Cox DR, Howard SV, et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. Analysis and examples. Br J Cancer 1977;35: 1–39. Guidelines for ATC classification and DDD assignment. World Health Organization Collaborating Center for Drug Statistics Methodology; 1996. Johnson BE. Second lung cancers in patients after treatment for an initial lung cancer. J Natl Cancer Inst 1998;90:1335–45. Lippman SM, Lee JJ, Karp DD, Vokes EE, Benner SE, Goodman GE, et al. Phase III intergroup trial of 13-cis-retinoic acid to prevent second primary tumors in stage I non-small cell lung cancer (NSCLC): interim report of NCI #I91-0001 [abstract]. Proc ASCO 1998;17:456a. Leong PP, Rezai B, Koch WM, Reed A, Eisele D, Lee DJ, et al. Distinguishing second primary tumors from lung metastases in patients with head and neck squamous cell carcinoma. J Natl Cancer Inst 1998;90:972–7. Jyothirmayi R, Ramadas K, Varghese C, Jacob R, Nair MK, Sankaranarayanan R. Efficacy of vitamin A in the prevention of loco-regional recurrence and second primaries in head and neck cancer. Eur J Cancer 1996;32B:373–6. Bolla M, Lefur R, Ton Van J, Domenge C, Badet JM, Koskas Y, et al. Prevention of second primary tumours with etretinate in squamous cell carcinoma of the oral cavity and oropharynx. Results of a multicentric double-blind randomised study. Eur J Cancer 1994;30A:767–72. Vainio H, Rautalahti M. An international evaluation of the cancer preventive potential of vitamin A. Cancer Epidemiol Biomarkers Prev 1999;8: 107–9. Hennekens CH, Buring JE, Manson JE, Stampfer M, Rosner B, Cook NR, et al. Lack of effect of long-term supplementation with beta carotene on the incidence of malignant neoplasms and cardiovascular disease. N Engl J Med 1996;334:1145–9. Pastorino U. Beta-carotene and the risk of lung cancer. J Natl Cancer Inst 1997;89:456–7. Wang XD, Liu C, Bronson RT, Smith DE, Krinsky NI, Russell RM. Retinoid signaling and activator protein-1 expression in ferrets given betacarotene supplements and exposed to tobacco smoke. J Natl Cancer Inst 1999;91:60–6. Lippman SM, Benner SE, Hong WK. Cancer chemoprevention. J Clin Oncol 1994;12:851–73. NOTES The authors are the writing committee for the EUROSCAN Study. The writing committee assumes responsibility for the integrity of this manuscript on behalf of the participants in the EUROSCAN Study (see “Appendix” section preceding “References”). The EUROSCAN Study was funded by support from the European Organization for Research and Treatment of Cancer (EORTC) to the EORTC Data Center and from The Netherlands Cancer Institute to the Biometrics Department and by three separate grants from the European Commission—Directorate General V—Programme “Europe Against Cancer.” Financial support for meetings was received from Zambon (Milan, Italy). Zambon provided N-acetylcysteine, and Mucos (Geretsried, Germany) provided retinyl palmitate. Manuscript received July 19, 1999; revised March 29, 2000; accepted April 13, 2000. Journal of the National Cancer Institute, Vol. 92, No. 12, June 21, 2000