Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
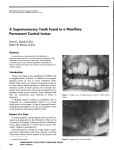
Orthodontic treatment for an unerupted and severely rotated maxillary central incisor. A case report Y. FUJITA, T. TAKAHASHI, K. MAKI ABSTRACT. Background Many reports have indicated the treatment for permanent teeth with disturbed eruption due to the presence of supernumerary teeth. However, successful treatment for an unerupted maxillary incisor with severe rotation and another maxillary incisor with disturbed eruption by a supernumerary tooth is quite rare. Case report We treated a 7-year-old Japanese male with an unerupted and severely rotated maxillary right incisor, along with a maxillary left incisor due to interference with eruption by an inverted supernumerary tooth. Orthodontic treatment using surgical exposure, traction and guidance of the rotated right incisor, and maxillary expansion following extraction of the supernumerary tooth were performed. Follow-up At 27 months following extraction of the supernumerary tooth, and comprehensive orthodontic treatment led the malposititioned central incisors to a functional position and stable occlusion KEYWORDS: Supernumerary tooth; Maxillary central incisors, Orthodontic treatment. Introduction Disturbances of eruption of permanent teeth are considered to be common anomalies that occur during teeth eruption in the mixed dentition period, and may result from a number of general and local factors, such as Down’s syndrome, cleidocranial dysostosis, prolonged retention of deciduous teeth, abnormal positioning of tooth buds, odontoma, trauma of primary teeth [Shapira et al., 2000; Angle and Rebellato, 2005; Betts and Camilleri, 1999; Batra et al., 2004; Cozza et al., 2003], and supernumerary teeth with the latter reported to be the most common cause of unerupted maxillary central incisors [Ochoa Grijalva and Kuster, 1993]. Many reports have indicated that the treatment of choice for impaction or delayed eruption of the maxillary central incisors is orthodontic traction following surgical exposure of the teeth [Batra et al., 2004; Ochoa Grijalva and Kuster, Division of Developmental Stomatognathic Function Science Department of Growth and Development for Function Kyushu Dental College, Japan e-mail:[email protected] EUROPEAN JOURNAL OF PAEDIATRIC DENTISTRY • 1/2008 1993; Agrait et al., 2003; Crawford, 1997; Thosar and Vibhute, 2006; Cozza et al., 2003]. On the other hand, several studies have found that a number of patients with impacted or delayed eruption of maxillary central incisors experienced spontaneous eruption following only removal of the causes, such as supernumerary teeth when sufficient space was available [Bryan et al., 2005; Leyland et al., 2006; Cozza et al., 2006]. However, such successful treatment for an unerupted maxillary incisor with severe rotation is quiet rare. In the present patient, we performed comprehensive orthodontic therapy including surgical treatment for the unusual condition of the maxillary left incisor due to interference of eruption by an inverted supernumerary tooth, along with an unerupted maxillary right incisor with severe rotation. Case Report A seven-year-old male came to our dental clinic, with the chief complaint of non-eruption of the permanent maxillary right incisor. The medical history of the patient was unremarkable. A clinical examination revealed the presence of early mixed 43 Y. FUJITA ET AL. edentulous area showed more fibrous gingival tissue (Fig. 1). Occlusal caries were found in both first permanent molars. A radiographic examination revealed the presence of an inverted supernumerary tooth overlapping the root of the maxillary left incisor. Further, the maxillary right incisor was completely impacted with a 90 degrees of distal rotation around its long axis. Root development of both permanent central incisors was at the initial stage (Fig, 2a, 3). Cephalometric analysis revealed normal values according to Japanese standards, except a greater inclination of the mandibular plane (Fig. 3). From these findings, the treatment plan for this case was as follows. 1. Surgical exposure and orthodontic treatment of the impacted and rotated upper right incisor. 2. Extraction of the supernumerary tooth. 3. Space regaining for proper alignment of the rotated upper central incisors. Two months after the first appointment, the patient underwent surgical exposure of the impacted right incisor. At the same time, the inverted supernumerary dentition composed of the following permanent teeth: mandibular first molars, mandibular central incisors, and maxillary left incisor. The maxillary left incisor region had an enlarged labial gingiva: the adjacent FIG. 1 - Pre-treatment intraoral photograph. a b c d FIG. 2 - Periapical radiographs of the maxillary incisors. a. Before treatment. b. Three months after surgical exposure. c. Three months after initiating orthodontic traction. d. Completion of orthodontic treatment. a b FIG. 3 - Pre-treatment panoramic (a) and cephalometric (b) radiographs. 44 EUROPEAN JOURNAL OF PAEDIATRIC DENTISTRY • 1/2008 ORTHODONTIC TREATMENT OF INCISORS a b c b a FIG. 5 - Post-treatment intraoral photographs. tooth was removed. Three months later, bilateral central incisors erupted spontaneously. The periapical radiograph revealed appreciable movement of the impacted permanent right incisor, though the rotation remained (Fig. 2b). Therefore a button was bound to the labial surface of the upper right incisor. One week later, orthodontic traction was initiated. An additional auxiliary spring was soldered to the base arch, and a power chain was applied between the attachment and the auxiliary spring. At that point, the power chain was applied from the medial side of the crown in order to correct the rotation. Three months after initiating orthodontic traction, the rotation of the upper right incisor was nearly completely corrected (Fig. 2c, 4a), therefore both lingual arch and labial button were removed. One week later, a quad helix was applied to the upper arch for labial movement of the right incisor (Fig. 4b). One month later, a lingual arch was applied to the lower arch in order to correct linguoversion of the mandibular lateral incisors. Six months after initiating labial movement of the upper right incisor, a lack of available space for the upper incisors was apparent. Therefore, a rapid expansion device was applied in order to create adequate space (Fig. 4c). EUROPEAN JOURNAL OF PAEDIATRIC DENTISTRY • 1/2008 FIG. 4 - Intraoral photographs taken during treatment. a. Three months after initiating the orthodontic traction. b. Immediately after application of a quad helix. c. Prior to maxillary expansion. d. Three months after expansion of the maxillary dental arch. b c Three months after initiating maxillary expansion, adequate space for teeth alignment was obtained and the upper incisors reached the occlusal plane. Bands were placed on the upper first permanent molars and brackets were bonded from the lateral incisors. A 0.016-inch Ni-Ti wire was placed on the upper first molars and between the lateral incisors, and alignment of the upper anterior teeth was initiated (Fig. 4d). After wire adjustment for 6 months, the periapical radiograph revealed that root development of the upper left incisor was completed, though that of the upper right incisor was not (Fig. 2d). Further, the upper central incisors were aligned in the proper position and stable occlusion was achieved (Fig 5). Thereafter, the patient used a removable Hawley retention appliance for the following 6 months. Discussion Supernumerary teeth are reported to occur in permanent dentition in 1.5% to 3.36% of the general population, while they are found in 0.03% to 0.66% of the population in primary dentition. Most supernumerary teeth are located within the maxillary central incisor region with complications of 45 Y. FUJITA ET AL. uneruption of the permanent incisors, midline diastema, rotation and displacement of the incisors [Luten, 1967; Buenviaje and Rapp, 1984; Tay et al., 1984; Tyrologou et al., 2005]. For treatment of maxillary central incisors that interfere with eruption due to supernumerary teeth, Bryan et al. [2005] and Leyland et al. [2006] proposed that in the majority of cases spontaneous eruption will occur, if sufficient space is available, following only removal of the supernumerary teeth. Mason et al. [2000] reported that nearly 75% of incisors with an immature root erupted spontaneously after removal of an associated supernumerary tooth. On the other hand, several authors have reported cases of supernumerary tooth removal and orthodontic traction for impacted maxillary permanent incisors [Ochoa Grijalva et al., 1993; Thosar and Vibhute, 2006; Cozza et al., 2003]. In the present case, an inverted supernumerary tooth was found in the maxillary left incisor region. However, incomplete root development of the permanent left incisor, inadequate space for eruption of the left incisor, and the vertical eruption of the left incisor were noted. Therefore, we considered that the eruption disturbance would be solved by extraction of the supernumerary tooth alone. In the present patient, delayed eruption of a maxillary permanent right incisor with severe rotation was also found. Several causes of delayed eruption and rotation of permanent teeth have proposed, such as traumatic injury of a primary tooth causing damage to the corresponding permanent tooth or an abnormal position of the tooth bud. However, our patient had no apparent dental or alveolar trauma. Therefore, the cause of delayed eruption and rotation in this case may be the presence of a supernumerary tooth. A number of successful treatments for delayed eruption and rotation of permanent teeth have been reported including the use of techniques such as orthodontic repositioning and surgical reimplantation [Shapira et al., 2000; Angle and Rebellato, 2005; Betts and Camilleri, 1999; Batra et al., 2004]. However, cases of a delayed tooth eruption accompanied with severe rotation are extremely rare. Initially, we considered that correction of the rotation would be quite difficult. Orthodontic treatment after surgical exposure was simply completed instead of prosthetic treatment, because of the request of the parents. Successful alignment of an impacted tooth depends on its position and direction, degree of root completion, and presence of space for the impacted tooth [Bryan et al., 2005]. In the present case, root development of the impacted upper incisor was immature. By using a lingual arch and quad helix, 46 severe rotation was nearly completely corrected after surgical exposure of the upper right incisor. Because of lack of available space for the erupted upper incisors, an anterior and bilateral rapid expansion device was applied. After obtaining adequate space, we placed brackets on the upper incisors and applied orthodontic force to the upper incisors. Thus, the severe rotation of the upper right incisor was completely corrected. The main complication following treatment of rotation is relapse. It has been reported that early treatment and a longer retention period were necessary to reduce the possibility of relapse [Ahrens et al., 1981]. The present patient also had a risk of relapse of the upper right incisor after rotational correction, therefore, we planned a long-term retention for the maxilla by wearing removable Hawley appliance. Two years after initial treatment, the upper central incisors reached a normal position and stable occlusion in the early mixed dentition period. However, long-term monitoring for the bone growth of this patient is necessary until normal permanent occlusion is reached. Conclusion We treated a rare case of an unerupted maxillary right incisor with severe rotation, and the unusual condition of a maxillary left incisor due to interference with eruption by the presence of an inverted supernumerary tooth in the early mixed dentition. We performed the comprehensive orthodontic treatment using surgical exposure, traction and guidance of the right incisor, and maxillary expansion following extraction of the supernumerary tooth. As a result, the maxillary incisors were aligned into a functional position and stable occlusion. Acknowledgements We are grateful to late Dr. Reiji Seo for valuable comments in the preparation of the manuscript. References Agrait EM, Levy D, Gil M, Singh GD. Repositioning an inverted maxillary central incisor using a combination of replantation and orthodontic movement: a clinical case report. Pediatr Dent 2003; 25:157-160. Ahrens DG, Shapira Y, Kuftinec MM. An approach to rotational relapse. Am J Orthod 1981; 80:83-91. Angle AD, Rebellato J. Dental term management for a patient with cleidocranial dysostosis. Am J of Orthod Dentofacial Orthop 2005; 128:110-117. EUROPEAN JOURNAL OF PAEDIATRIC DENTISTRY • 1/2008 ORTHODONTIC TREATMENT OF INCISORS Batra P, Duggal R, Kharbanda OP, Parkash H. Orthodontic treatment of impacted anterior teeth due to odontomas: a report of two cases. J Clin Pediatr Dent 2004; 28:289-294. Betts A, Camilleri GE. A review of 47 cases of unerupted maxillary incisors. Int J Paediatr Dent 1999; 9:285-292. Bryan RA, Cole BO, Welbury RR. Retrospective analysis of factors influencing the eruption of delayed permanent incisors after supernumerary tooth removal. Eur J Paediatr Dent 2005; 6:84-89. Buenviaje TM, Rapp R. Dental anomalies in children: a clinical and radiographic survey. J Dent Child 1984; 51:42-46. Cozza P, Gatto R, Marino A, Mucedero M. Case report: two nasal floor compound odontomas associated with impacted maxillary incisor. Eur J Paediatr Dent. 2003; 4:99-102. Cozza P, Mucedero M, Ballanti F, De Toffol L. Supernumerary teeth and mental retardation: the importance of early surgical intervention. Eur J Paediatr Dent. 2006; 7:45-49. Crawford LB. Impacted maxillary central incisor in mixed dentition treatment. Am J Orthod and Dentofacial Orthop 1997; 112:1-7. Leyland L, Batra P, Wong F, Llewelyn R. A retrospective evaluation of the eruption of impacted permanent incisors after extraction of supernumerary teeth. J Clin Pediatr Dent 2006; EUROPEAN JOURNAL OF PAEDIATRIC DENTISTRY • 1/2008 30:225-231. Luten JR. The prevalence of supernumerary teeth in primary and mixed dentitions. J Dent Child 1967; 34:346-353. Mason C, Azam N, Holt RD, Rule DC. A retrospective study of unerupted maxillary incisors associated with supernumerary teeth. Br J Oral Maxillofac Surg 2000; 38:62-65. Ochoa Grijalva JF, Kuster CG. Supernumerary teeth removal and orthodontic tooth repositioning: a case report. J Clin Pediatr Dent 1993; 17:95-98. Shapira J, Chaushu S, Becker A. Prevalence of tooth transposition, third molar agenesis, and maxillary canine impaction in individuals with Down syndrome. Angle Orthod 2000; 70:290296. Tay F, Pang A, Yuen S. Unerupted maxillary anterior supernumerary teeth: report of 204 cases. J Dent Child 1984; 51:289-294. Thosar NR, Vibhute P. Surgical and orthodontic treatment of an impacted permanent central incisor: A case report. J Indian Soc Pedod Prev Dent 2006; 24:100-103. Tyrologou S, Koch G, Kurol J. Location, complications and treatment of mediodentes—a retrospective study in children. Swed Dent J 2005; 29:1-9. 47