Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
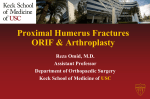
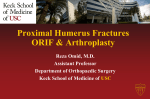
14 The surgical approach, its vascular implications and the importance of medial calcar support in maintaining fracture reduction in locked plating of proximal humerus fractures - A review. Sreevathsa Boraiah, MD, Michael J Gardner, MD, Dean G Lorich, MD. Orthopedic Trauma Service, Hospital for Special Surgery, 535 east 70 street, New York, 10021. Introduction P roximal humerus fractures are becoming increasingly common with growing elderly population. These fractures are often associated with osteoporotic bone and dysvascularised fracture fragments, which may cause difficulty in surgical fixation and poor outcomes. With the emphasis on preservation of blood supply to the bone and development of a less invasive means of obtaining fracture reduction and fixation we sought a more direct means of exposing the proximal humerus. The deltopectoral approach provides anterior exposure of the proximal humerus yet the fixation is applied laterally. When the greater tuberosity is displaced posteriorly, access for manipulation and reduction of the fragment requires wider exposure thereby increasing soft tissue stripping. We sought a more direct lateral exposure of the proximal humerus, which not only facilitates fracture reduction via a laterally based plate but also preserves an already compromised blood supply to the humeral head by avoiding injury to the anterior circumflex humeral artery. Further a more lateral approach facilitates fracture reduction by working through the fracture line laterally and permitting better access to anatomic, surgical neck and also to the displaced greater tuberosity fragment. Our first cadaver study analyses the lateral approach by describing the axillary nerve anatomy in the region and safely isolating it during plating. The next cadaver study assess the vascular preservation of the humeral head by describing the vascular anatomy and a watershed area devoid of a significant blood supply that could be disrupted during the lateral approach. The outcomes of our approach were analyzed in a clinical series, which proves that the anterior deltoid innervation was preserved after locked plating of proximal Correspondence : Sreevathsa Boraiah, MD Orthopedic Trauma Service, Hospital for Special Surgery, 535 east 70 street, New York, 10021. humerus through the lateral approach. Locked plating has offered a novel biomechanical approach to stabilizing fractures. Few clinical reports exist on results of locking plate fixation of proximal humerus fractures; short-term functional outcomes and complication rates have been variable. Locked plating is no panacea in the absence of medial calcar support. Our study, which evaluates radiographs in the immediate post operative period and subsequent follow up studies reveal the importance of medial calcar support in maintaining fracture reduction after locked plating. The surgical approach and its vascular implications. Lateral approaches to the proximal humerus have been limited by position of the axillary nerve. Extensive dissection through deltopectoral approach may further damage the remaining tenuous blood supply to the proximal humerus. We conducted two studies on the proximal humerus on the cadavers. First study describes the surgical approach and the axillary nerve and the next study describing the vascular implications of minimally invasive plating using the lateral approach to the proximal humerus. Anterolateral Acromial Approach. Poor results after plate fixation of plate of proximal humerus using traditional deltopectoral approach requiring a extensive soft tissue dissection may be related to fragment devascularization during dissection or plating, or disruption of critical blood supply to the humeral head. To develop a more biologically focused and less invasive approach to the Pb Journal of Orthopaedics Vol-X, No. 1, 2008 proximal humerus we explored an alternative surgical approach to the proximal humerus. A direct approach to the lateral proximal humerus historically has been restricted to 35 cm distal to the acromion because of the position of the axillary nerve. We hypothesized that by using an anterolateral acromial approach in cadaveric dissection the incision could be distally extended by reliably palpating and protecting the anterior axillary nerve motor branch. This depends on one anterior motor branch crossing the anterior deltoid raphe and the nerve being in a predictable location to allow safe observation, as measured from consistent bony landmarks. Twenty fresh frozen human cadaveric shoulders each from a different donor were obtained from anatomic gift registry. With shoulder in 00 abduction a skin incision was made anterolateral acromion, extending approximately 8-10 cm distally. The subcutaneous tissue layer was then bluntly dissected to identify the avascular raphe separating the anterior and middle heads of deltoid (Fig 1, 3a). The superior most part of the raphe was incised and the surgeon's finger was inserted to sweep the undersurface of the deltoid. Once the axillary nerve was palpated the incision in the raphe was carefully extended down protecting the axillary nerve and the posterior circumflex humeral artery (Fig 2, 3b). Fig-1. Anterior and middle heads of deltoid after incising the skin and the fascia. Fig-2 Axillary nerve safely dissected out using the intermuscular raphe between anterior and middle heads. Surgical approach-proximal humeral fractures 15 Fig-3a,b. Schematic representation of the deltoid, the septum and the axillary nerve dissected out through this septum. Two separate observers made anatomical observations. Axillary nerve was palpable as a cord like structure in the loose areolar tissue between the deltoid and the raphe several cm distal to the incision, and was distinct in all specimens to both observers. The distance from the lateral prominence of the greater tuberosity to the superior edge of the nerve was 35.5mm(range, 32.1-42.5 mm; 99% confidence interval, 34.0-37.omm), and the average distance from the undersurface of the undersurface of the acromion to the superior border of the nerve measured 63.3mm (range, 53.270.4 mm 99% confidence interval, 60.2-66.4mm). The nerve could be elevated from the bone on an average of 13.4mm before becoming taut. Reflection of the deltoid revealed that no nerve branches other than the anterior axillary trunk crossed the anterior deltoid raphe in any specimen. The last branch of the nerve to the middle deltoid head raised an average of 9.8mm before crossing the raphe. The feasibility of the anterolateral acromial approach was confirmed initially by the anatomic portion of this study. The axillary nerve was readily palpated and subsequently protected in all specimens by both observers. The axillary nerve arises from the posterior cord of the brachial plexus and passes through the quadrilateral space, dividing into anterior and posterior branches. The anterior motor branch wraps around the neck of the humerus and gives variable innervations to the three heads of the deltoid. At the junction of the anterior and middle head of the deltoid exists an avascular raphe. The course of the axillary nerve distal to the quadrilateral space has been described, but its precise position as it crosses the anterior raphe has not been elucidated. The anterior motor branch of the axillary nerve crosses the humerus transversely at a variable distance as a single nerve and penetrated the fascia before or after dividing into small Boraiah et al. 16 branches. Most importantly, we found that no other branches of the axillary nerve crossed at the level of the fibrous raphe other than the results described above. This allowed the deltoid to be split between the anterior and middle branch after identification of the anterior branch without placing the small branches at risk. Once the anterior branch was identified a safe plane for splitting the deltoid to access the proximal humerus was established. Vascular implications of minimally invasive plating of proximal humerus fractures Poor outcomes of proximal humerus fractures treated with traditional plating may due to devasucularisation of the fracture fragments with subsequent delayed union, or avascular necrosis (AVN) of the humeral head. This devascularization may be due to trauma itself and/or surgical dissection. Sturzenegger et al reported a more than 3 fold increase of AVN after plating compared with minimally invasive plating, and implicated additional iatrogenic vascular insult with open reduction causing this result. AVN rates have been reported between 4 and 10 % however the follow up ranged only from 2 to 18 months. The standard deltopectoral (DP) approach necessitates significant surgical dissection and muscle retraction to gain adequate exposure to lateral aspect of the humerus because it is an indirect approach to the plating zone. Additionally, crucial blood supply to the humeral head, the anterior circumflex humeral artery (AHCA), courses laterally along the inferior border of subscapularis tendon directly in the surgical field. This may place it at risk during the DP approach, particularly with a distorted anatomy as a result of fracture. Six fresh-frozen cadaveric upper extremity specimens were obtained from the anatomic gift registry. With the shoulder in neutral rotation, an approximately 10 cm incision was made beginning at the AL corner of the acromion and carried distally. The fascia of the deep deltoid was split superiorly to expose the raphe between the anterior and the middle heads of the deltoid. After splitting the raphe 6cm distally in the wound the axillary nerve was identified and protected. A three hole 3.5-mm locking proximal humerus plate (LCP< Syntese, Paoli, PA) was slid distally under the axillary nerve, and positioned 8 mm distal to the rotator cuff insertion centered on the greater tuberosity, as recommended by the manufacturer. Screws were placed into the shaft and head to stabilize the plate (Fig 4). Fig-4. Locked plating performed after the safe isolation of the nerve. After plating of the specimens, the axillary artery was found in the axilla and cannnulated with a 14 gauge plastic catheter and secured. The brachial artery was found distally in the region of the mid humeral shaft and ligated. Black labeled PMC 780 polymer (smooth-on, Inc., Easton, PA) was slowly injected into the axillary artery using a ratcheting cement gun to allow continuous ante grade perfusion of the latex and to ensure adequate perfusion of the end arterioles of the circumflex humeral system. Latex was allowed to polymerize for 18 hours. Deltoid and the pectoral muscles were then dissected and reflected to allow complete visualization of the anterior and the posterior circumflex humeral arteries (Fig 5). Pb Journal of Orthopaedics Vol-X, No. 1, 2008 Surgical approach-proximal humeral fractures 17 Clinical outcomes of locked plating of proximal humerus. Fig-5. Proximal Humerus with soft tissue stripping showing intact vasculature after plating. The ascending branch of the ACHA was visualized proximally at the bicipital groove as the plates were being applied. Further dissection after latex polymerization revealed that adequate perfusion of the end branches of both anterior and posterior circumflex vessels was achieved in all cases. Tracing the course of the vessels revealed that no vascular injury had occurred using this approach. A bare spot was identified on the proximal lateral region of the humerus in the region of the plate. This was a hypovascular area on the greater tuberosity (Fig 6). Fig-6. Bare spot on proximal Humerus. A prospective cohort study was designed for all patients undergoing open reduction and internal fixation of a proximal humerus fracture using the anterolateral acromial approach. Between May 2002 and July 2006 67 patients were treated with this approach. 40 patients were followed up for at least one year and formed the cohort of the study. The mean patient age was 65.3 yrs (range, 21 to 84 yrs: median, 68 years). Five patients were younger than 6o years. Fractures were classified by senior surgeon, a fellowship trained orthopedic traumatologist, according to the system of Neer. Seven patients had 2- part fractures, 25 patients had 3- part fractures, 8 patients had 4-part fracture. Surgical indications were 2 part fracture with 100% displacement or varus mal alignment and comminution which were deemed to be unstable, as well as all three part and four part fractures. Nine patients had humeral locking nail and 31 patients had proximal humerus locking plate using the technique described above. Average clinical follow-up was 28 months (range 12-49 months), and 12 of the 40 patients had follow up greater than 2 years. Patient's outcomes were assessed using the Quick DASH scale. This is a 11- item scale which has similar discriminant ability, cross-sectional and retest reliability as the full length DASH. Scores were calculated on a scale of 0100, similar to DASH, with higher scores indicating greater disability. Quick DASH scores were also used to determine an excellent (score< 20), good (20 –39), fair (40-60), or poor (> 60) clinical outcomes. In addition a focused physical examination was performed to assess active range of motion, for which humeral forward flexion and abduction were measured with strict scapular stabilization. Manual testing of forward flexion strength was measured on a scale of 0-5 compared to the contra lateral side, which was used as an indicator of anterior deltoid and axillary nerve function. In all cases, the anterolateral the approach was performed and the axillary nerve was identified without difficulty. All fractures healed, and no patients developed avasular necrosis (AVN) of the humeral head. The average quick DASH score for the entire group was 25.2 (range, 0 to 65.9; median, 22.7). Thirty-three patients had good or excellent results, three patients had poor results. Forward flexion range of motion averaged 122 degrees (range, 20 to 180). One patient, an 84year-old male developed early painful stiffness and at final evaluation had flexion of 30 degrees, abduction of 20 and a quick DASH score of 62.5. In conclusion, the anterolateral acromial approach allows minimally invasive access for the treatment of proximal humerus fractures. The key aspect of this approach, the identification and the protection of the 18 Boraiah et al. axillary nerve, does not appear to have any deleterious effects on the nerve function. On the contrary, nerve exploration may reveal entrapment at the fracture site and allow mobilization, as was the case in two patients in the series. The direct access to the fracture site avoids exposure of the anterior critical humeral head vascularity, and may decrease the rate of AVN. The importance of medial calcar support in maintaining fracture reduction. Few clinical reports exist on the results of locking plate fixation of the proximal humerus fractures, and short-term functional outcomes and complications have been variable. When locking plates are placed on the lateral proximal humerus, the mechanical environment is such that fixed angle screws are required to act as perpendicular struts to support the humeral head fragment and resist varus displacement. These forces may be exaggerated when there is lack of medial column support, and the ability of these screws to perform this function is unknown. Guidelines have not been provided about the appropriate placement of locking screws such the mechanical advantage is optimized. We studied the radiographic behavior of proximal humerus fractures treated with locking plates in a consecutive series of patients with acute fractures. In addition we sought to determine what patient factors, fracture patterns, reduction variables, and implant placement affect the stability of fracture fixation. We hypothesized that mechanical support of the medial column would be particularly important for establishing a stable construct. Medical records and radiographs of 35 consecutive patients treated at our institution from March 2003 to February 2006 and who met the inclusion criteria were analyzed. The “ humeral head height” relative to the plate was measured for each radiograph, both initially and at the final follow up, which allowed for subsequent loss of reduction. Drawing 2 lines, both perpendiculars to the shaft of the plate, did this measurement; one was placed at the top edge of the plate and one was placed at the superior edge of the humeral head and the distance between the 2 lines was measured and designated as head height (Fig- 7). Fig-7. Measurements for the humeral head height. The change in this height from immediate postoperative radiographs to the final follow up, at which time all fractures were healed, was calculated. All radiographic measurements were standardized for magnification with known implant size and were performed by an independent observer. All cases were subdivided into 2 groups according to the presence or absence of medial mechanical support of the proximal humeral head fragment. The fracture was considered adequate considered support (+ MS group) if (1) the medial pillar of the proximal humerus was not comminuted and anatomically reduced (2) The shaft was medialised and impacted into the head fragment; or (3) an oblique locking screw was placed directly into the inferomedial quadrant of the proximal humeral head fragment within 5mm of the subchondral bone (Fig-8). Conversely, fractures that did not fulfill one of these criteria were designated as having inadequate medial support (- MS group) (Fig-9). Pb Journal of Orthopaedics Vol-X, No. 1, 2008 Fig-8. Radiograph showing the inferomedial screws, which augment medial calcar. Fig-9. Radiograph demonstrating the loss of reduction of humeral head .The image on the left demonstrates the inferomedial screw, which was not placed (image on the right). Average patient age was 62 years (range 23 to 89 years; median, 62 years). Overall there were 6 two-part, 15 threepart, and 14 four- part fractures according to Neer classification. Average follow up was 7 months (range, 6 to 77 weeks: median, 25 weeks). Eighteen patients were considered to have medial support and were designated in the + MS group. The average age of this group was 55 years. 9 patients had an anatomic reduction of the medial cortex without comminution, and 6 had 1 or 2 inferomedial screws placed; three patients had both. In three patients Norian bone substitute was placed. The average height loss of humeral Surgical approach-proximal humeral fractures 19 head was 1.2mm(SD, 1.4mm), and the maximum was 4.1mm. One 61-year-old patient with a 3 part comminuted surgical neck and greater tuberosity fracture, had an inferomedial screw placed but had screw penetration through the humeral head and required revision surgery for screw removal at 3 months postoperatively. All patients healed without any delayed union. There were 17 patients remaining in the –MS group. The breakdown of fracture types in this group were 2 two-part, 7 three-part, and 8 four-part, which was not significantly different between the groups. Twelve patients had malreduction with lateral displacement of the shaft fragment, without opposition of the medial cortex, and 5 had significant comminution; no patient had a screw placed in the inferomedial region. Humeral head height loss in this group averaged 5.8mm (SD, 3.9mm), which was significantly greater than in the +MS group. The maximal humeral height loss was 13.6mm, and 9 patients had greater than 5mm of height loss (p <0.001). Of the 17 patients without medial support, 5 had screw penetration of the articular surface and, 2 of who had loosening of other screws and 2 of who underwent revision surgery for screw removal. Despite the fracture migration and implant cutout in this group, all fractures achieved solid bony union in timely fashion. The mechanical performance of proximal humeral locking plate has been variable according to previous authors. A preliminary report of a multi center study of 147 patients found a 14% incidence of mechanical complications, and this was closely related to mechanical varus malreduction. The locking plate may be adjusted slightly proximally or distally, and is often placed where it best fits the anatomy of lateral cortex and greater tuberosity, without particular attention to the location of screws in the proximal fragment. But ultimately, according to our results, if the position of the plate is not chosen by ensuring that the inferomedial screws will be placed in the proper location, screws can be easily misplaced and early mechanical failure may become more likely. It seems that constructs that have screws only superiorly in the humeral head without fixation-anchored inferomedially, especially when medial communition or malreduction is present, may be ineffective in maintaining fracture reduction. In cases where stable bony medial column support cannot be achieved secondary to fracture comminution we have sought to support our fixed construct with additional endosteal support. This stable additional endosteal support was achieved by placing either an intramedullary plate which was locked in by the screws running from the extramedullary laterally based locking plate (Fig-10), or more recently by placing an allograft fibula endosteally and locking it with laterally placed locking plate (Fig-11). A clinical series of this pattern of medial calcar augmentation is the latest study in the spectrum of treatment of proximal humerus fractures. The result of this study shows that the fracture reduction can be maintained within 1mm margin. Boraiah et al. 20 margin of 1mm. With the treatment of proximal humerus fractures still evolving, good reduction of medial cortex and augmentation of medial calcar may be a solution for better outcomes. Fig-10. Radiograph showing the augmentation of medial calcar with an endosteal plate locked by the screws running from the laterally based locking plate. Fig-11. Radiograph showing the augmentation of medial calcar with an allograft fibula placed in the intramedullary cavity locked with screws from locking plate. In conclusion, minimally invasive plating using a direct lateral approach is a safe and effective way of plating the proximal humerus fractures with very little vascular insult. We had no reported incidence of axillary nerve palsy, particularly the branch that supplied the anterior head of deltoid. Also after understanding the importance of medial calcar support, our prospective study evaluating the outcomes of augmentation of medial calcar shows that the fracture reduction of the humeral head can be maintained within a References 1. Gardner MJ, Griffith MH, Dines JS, Briggs SM, Weiland AJ, Lorich DG. The extended anterolateral acromial approach allows minimally invasive access to the proximal humerus. Clinical orthopaedics and related research 2005:123-9. 2. Gardner MJ, Voos JE, Wanich T, Helfet DL, Lorich DG. Vascular implications of minimally invasive plating of proximal humerus fractures. Journal of orthopaedic trauma 2006;20:602-7. 3. Gardner MJ, Weil Y, Barker JU, Kelly BT, Helfet DL, Lorich DG. The importance of medial support in locked plating of proximal humerus fractures. Journal of orthopaedic trauma 2007;21:185-91. 4. Kristiansen B, Christensen SW. Plate fixation of proximal humeral fractures. Acta Orthop Scand 1986;57:320-3. 5. Sturzenegger M, Fornaro E, Jakob RP. Results of surgical treatment of multifragmented fractures of the humeral head. Archives of orthopaedic and trauma surgery 1982;100:249-59. 6. Traxler H, Surd R, Laminger KA, Windisch A, Sora MC, Firbas W. The treatment of subcapital humerus fracture with dynamic helix wire and the risk of concommitant lesion of the axillary nerve. Clinical anatomy (New York, NY 2001;14:418-23. 7. Kontakis GM, Steriopoulos K, Damilakis J, Michalodimitrakis E. The position of the axillary nerve in the deltoid muscle. A cadaveric study. Acta Orthop Scand 1999;70:9-11. 8. Duparc F, Bocquet G, Simonet J, Freger P. Anatomical basis of the variable aspects of injuries of the axillary nerve (excluding the terminal branches in the deltoid muscle). Surg Radiol Anat 1997;19:127-32. 9. Wijgman AJ, Roolker W, Patt TW, Raaymakers EL, Marti RK. Open reduction and internal fixation of three and four-part fractures of the proximal part of the humerus. The Journal of bone and joint surgery 2002;84-A:1919-25. 10. Szyszkowitz R, Seggl W, Schleifer P, Cundy PJ. Proximal humeral fractures. Management techniques and expected results. Clinical orthopaedics and related research 1993:13-25. 11. Speck M, Lang FJ, Regazzoni P. [Proximal humeral multiple fragment fractures--failures after T-plate osteosynthesis]. Swiss surgery = Schweizer Chirurgie = Chirurgie suisse = Chirurgia svizzera 1996:51-6. 12. Bathis H, Tingart M, Bouillon B, Tiling T. [Surgical treatment of proximal humeral fractures. Is the T-plate still adequate osteosynthesis procedure?]. Zentralblatt fur Chirurgie 2001;126:211-6. 13. Hessler C, Schmucker U, Matthes G, Ekkernkamp A, Gutschow R, Eggers C. [Results after treatment of instable fractures of the proximal humerus using a fixed-angle plate]. Der Unfallchirurg 2006;109:86770, 72-4. 14. Koukakis A, Apostolou CD, Taneja T, Korres DS, Amini A. Fixation of proximal humerus fractures using the PHILOS plate: early experience. Clinical orthopaedics and related research 2006;442:115-20. 15. Plecko M, Kraus A. Internal fixation of proximal humerus fractures using the locking proximal humerus plate. Operative Orthopadie und Traumatologie 2005;17:25-50. 16. Fankhauser F, Boldin C, Schippinger G, Haunschmid C, Szyszkowitz R. A new locking plate for unstable fractures of the proximal humerus. Clinical orthopaedics and related research 2005:176-81.