Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
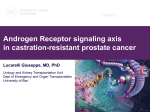
VOLUME 30 䡠 NUMBER 6 䡠 FEBRUARY 20 2012 JOURNAL OF CLINICAL ONCOLOGY UNDERSTANDING THE PATHWAY Molecular States Underlying Androgen Receptor Activation: A Framework for Therapeutics Targeting Androgen Signaling in Prostate Cancer Peter S. Nelson, Fred Hutchinson Cancer Research Center, Seattle, WA See accompanying article on page 637; listen to the podcast by Dr Taplin at www.jco.org/podcasts “You can observe a lot just by watching.” —Yogi Berra The androgen receptor (AR) is a resilient foe. Since the landmark studies of Huggins et al1 demonstrated the sensitivity of prostate cancer to androgenic hormones, androgen deprivation therapy has been the most widely used and effective treatment for metastatic disease. Although initial response rates exceed 90%, the eventual emergence of castration-resistant prostate cancer (CRPC) is nearly universal, and it represents a disease state that is usually fatal. However, a remarkable and extremely important aspect of CRPC is the near-universal reactivation of AR signaling, a finding readily substantiated through measurements of high serum concentrations prostatespecific antigen (PSA), a gene directly and exclusively regulated by the AR. Several studies have documented that most, and potentially all, genes known to be under AR transcriptional control in prostate cancer cells are re-expressed in CRPC tumors.2-4 In this context, the AR may be the earliest known example of a lineage oncogene—a master regulator to which neoplastic cells derived from prostate epithelium are addicted.5 AR engagement by androgenic ligands such as testosterone and dihydrotestosterone motivate AR migration from the cytoplasm to the nucleus, where AR target genes are recognized and activated through DNA binding to locations specified by nucleotide sequence and chromatin accessibility. The observation that AR-regulated genes are active in CRPC— despite undetectable levels of testosterone in blood— has prompted efforts to identify processes driving AR function in the castrate environment.6,7 Such alternative mechanisms of AR activation could represent targets for therapeutic inhibition. A key question that should influence further investment in obstructing the AR program in CRPC is whether the AR is continuing to provide the growth and survival signals for these tumors, or if the AR program is simply baggage carried along by other oncogenic drivers. Compelling evidence indicates the former is likely to be true. For example, experiments abolishing the AR itself in androgenrefractory prostate cancer cells in vitro effectively suppressed proliferation.8 CRPC tumors proliferating in castrate mice consistently regress after the targeted elimination of AR expression.9 Finally, clinical studies of secondary and tertiary methods to inhibit AR signaling in CRPC usually result in PSA and clinical responses, although they are generally of relatively short dura644 © 2011 by American Society of Clinical Oncology tion.10 Newer agents targeting androgen biosynthesis or blocking AR activation carry on this tendency.11,12 Together, these laboratory and clinical observations emphasize the continued relevance of the AR pathway as a key therapeutic node in the vast majority of patients with advanced CRPC. Unfortunately, over the past several decades, efforts to target AR signaling have blown hot and cold, with irrational exuberance followed by neglect. Insightful studies by Geller et al13,14 in the 1970s demonstrated that androgen levels within prostate cancers far exceeded concentrations found in castrate men, a finding that ushered in the era of combined androgen blockade (CAB) with steroidal and nonsteroidal androgen receptor antagonists. Despite many trials of CAB, the therapeutic advantage remains highly debated. Initial studies using either surgical or medical castration in conjunction with an antiandrogen suggested significant improvements in survival compared with historical controls.15 However, the benefits measured in subsequent randomized trials were not encouraging, although metaanalyses have consistently shown a statistically significant improvement in 5-year survival, on the order of 5%, in favor of CAB.16 Although certainly less impressive than anticipated, the trials of these early antiandrogens did not refute the hypothesis that AR is still a key driver in CRPC because of one key observation: Patients for whom these drugs failed experienced progression with a rising PSA, indicating the AR pathway remained active. Determining how the AR remained engaged awaited detailed molecular studies that identified mechanisms underlying the limited effectiveness of these AR antagonists and led to the next generation of AR inhibitors, such as MDV3100, with enhanced binding affinities and lacking agonist properties.17,18 To provide a framework for the clinical application of new agents designed to suppress androgen signaling, it is useful to consider the molecular endocrinology that underlies the maintenance of AR activity. On the basis of current knowledge of prostate cancer molecular biology, at least four discrete cellular states of prostate cancer can be defined, based solely on the status of AR program activity and the mechanism by which it is activated. Of clinical relevance, the cellular states are dynamic and evolve either through adaptation or genomic events, and each molecular state is also associated with a specific therapeutic node that generally requires effective inhibition—and Journal of Clinical Oncology, Vol 30, No 6 (February 20), 2012: pp 644-646 Information downloaded from jco.ascopubs.org and provided by at Danish National Library Authority on March 26, 2014 from Copyright © 2012 American Society of Clinical Oncology. All rights reserved. 193.163.235.201 Understanding the Pathway STATE 1 Endocrine androgen dependent and AR dependent STATE 2 STATE 3 STATE 4 Intracrine androgen dependent and AR dependent Androgen (ligand) independent and AR dependent Androgen (ligand) independent and AR independent Others… IL-6 HER2 Intracrine testosterone Prostate cancer cells AR AR DHT T DHEA Endocrine T testosterone (T) Testis T testis Others… Adrenal ARSV T DHT cholesterol T testis DHEA DHE A Others Oth ers… Others… Adrenal N-cadherin Src? AR T DHT Src? AR T T DHT IL-6 HER2 Neuroendocrine carcinoma ? T testis DHEA Othe Oth ers… ers s Others… Adrenal Fig 1. Molecular states framework for androgen receptor (AR) activation in prostate cancer. Four discrete states of prostate carcinoma can be defined on the basis of sources of androgenic ligands and the activity of AR. In state 1 (endocrine androgen dependent and AR dependent), prostate carcinoma cells are dependent on high levels of circulating testosterone (T) synthesized in the testis. In state 2 (intracrine androgen dependent and AR dependent), after the suppression of circulating T, androgenic ligands can be found in tumor cells through de novo synthesis or the conversion of adrenal precursors such as DHEA. In state 3 (androgen independent and AR depentent), the AR remains active in the absence of ligands through crosstalk with other signal transduction pathways that may include HER2/neu, IL-6, Src kinase, and others, or through the expression of ligand-independent AR splice variant (ARSV). In state 4 (androgen independent and AR independent), AR signaling is abolished, and complete responses are achieved, or tumor progression is driven by other oncogenic programs yet to be determined. Ablating the AR program should be objective of the successful combinatorial applications of emerging AR therapeutics. DHEA, dehydroepiandrosterone; DHT, dihydrotestosterone; HER2, human epidermal growth factor receptor 2; IL-6, interleukin 6. subsequent resistance— before transition. For this discussion, dependence is operationally defined as that factor or component required by a cell for survival and the engagement of other functions carried out by neoplastic prostate epithelium such as PSA protein secretion. The molecular states (Fig 1) are as follows: State 1: Endocrine androgen dependent. The drivers and therapeutic node promoting the AR pathway in this state are serum androgens produced in the testis. With few exceptions, current therapies such as luteinizing hormone–releasing hormone agonists and antagonists generally produce excellent results in terms of achieving low serum testosterone levels in most patients. Thus, further research efforts in this domain are unlikely to contribute substantially to improved outcomes. State 2: Intracrine androgen dependent. The drivers of AR signaling in this state are also androgens, but they are produced within prostate cancer cells either from adrenal precursors or through de novo metabolism.19 Recent studies, fundamentally rediscovering the early work of Geller et al13,14 demonstrating high intratumoral androgen concentrations relative to serum levels, have strongly supported the existence of this cellular state, although many questions remain concerning how androgens are generated.20 The process of steroid biosynthesis, whether within the adrenal gland or the prostate, involves a series of metabolic enzymes responsible for the stepwise conversion of cholesterol to testosterone and dihydrotestosterone, and several represent druggable nodes. Although the metabolic pathway is complex (as reviewed21), the clinical responses observed in men with CRPC treated with the 17␣hydroxylase-17,20-lyase inhibitor abiraterone support at least CYP17 as a relevant target. Although abiraterone treatment extends survival, failure of this treatment is common and also marked by rising PSA— once again demonstrating that therapy failure is associated with reactivation of AR signaling.12 Establishing the mechanism by which the AR program is maintained in this setting is essential and will require direct assessments of tumor tissue to confirm adequate suppression of CYP17 activity and www.jco.org ideally quantitation of intratumor androgen levels. In this issue of the Journal of Clinical Oncology, Efstathiou et al22 provide an important first step in distinguishing those tumors that may be most susceptible to abiraterone by directly measuring the expression of CYP17 in metastatic tumor cells acquired from bone. Intense nuclear localization AR concomitant with CYP17 expression correlated with longer time remaining on treatment. Of interest, bone marrow plasma concentrations of testosterone and DHT were undetectable in men progressing while receiving abiraterone, indicating either that these tumors are no longer dependent on AR ligands or that marrow plasma is not an accurate surrogate for intratumoral measurements. State 3: Ligand independent, AR dependent. Extensive literature exists regarding mechanisms with the potential to activate the AR in the complete absence of androgens. Elegant in vitro studies, performed in laboratory situations in which androgen levels can be rigorously eliminated, have demonstrated that crosstalk with other signal transduction pathways can activate AR signaling.23,24 However, it has been challenging to confirm that these networks promote AR effects in humans. Recently, several AR variants (ARVs) have been identified that result from alternative splicing of the AR transcript.25-28 A striking feature of these receptors, if such terminology is still applicable, is the lack of a C-terminal ligand-binding domain; however, ARVs are functionally able to confer ligand-independent activation of known AR target genes. ARVs may also regulate a gene repertoire distinct from the full-length AR. Under the selective pressure of improved antagonists with higher affinities for AR and drugs that further suppress ligands, ARVs may emerge as more common mediators of ligandindependent AR-dependent tumor progression and will require new strategies, such as compounds that interfere with N-terminal ARDNA interactions.29 State 4: Ligand independent, AR independent. This state of prostate cancer may synonymously be termed AR pathway–independent prostate cancer, which is effectively AR null. With the exception of small-cell or neuroendocrine carcinomas, this tumor cell state is rarely observed in the clinical management of men with prostate cancer and © 2011 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at Danish National Library Authority on March 26, 2014 from Copyright © 2012 American Society of Clinical Oncology. All rights reserved. 193.163.235.201 645 Peter S. Nelson may be simply defined as tumor progression in the setting of undetectable levels of PSA. Only in this setting could the AR program be considered extinguished. Future clinical strategies for men with CPRC are obvious: As several new active drugs are approved or in late stages of development that inhibit distinct noncrossreactive nodes in the androgen signaling pathway, they should be evaluated in combinations to determine if such highly active anti-AR therapy will successfully extinguish the AR program, a concept analogous to the successful deployment of combinatorial, highly active antiretroviral therapy for the treatment of HIV.30 The result may produce complete remissions, possibly cures, or the emergence of prostate cancers that no longer depend on AR signaling. Until that time, it is important to follow Sutton’s law and go “where the money is,”30 because in this case, the money is still on the AR. REFERENCES 1. Huggins C, Hodges CV: Studies on prostate cancer 1: The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res 1:293-297, 1941 2. Nelson PS, Clegg N, Arnold H, et al: The program of androgen-responsive genes in neoplastic prostate epithelium. Proc Natl Acad Sci U S A 99:11890-11895, 2002 3. Tomlins SA, Mehra R, Rhodes DR, et al: Integrative molecular concept modeling of prostate cancer progression. Nat Genet 39:41-51, 2007 4. Holzbeierlein J, Lal P, LaTulippe E, et al: Gene expression analysis of human prostate carcinoma during hormonal therapy identifies androgenresponsive genes and mechanisms of therapy resistance. Am J Pathol 164:217-227, 2004 5. Garraway LA, Sellers WR: Lineage dependency and lineage-survival oncogenes in human cancer. Nat Rev Cancer 6:593-602, 2006 6. Montgomery RB, Mostaghel EA, Vessella R, et al: Maintenance of intratumoral androgens in metastatic prostate cancer: A mechanism for castration-resistant tumor growth. Cancer Res 68: 4447-4454, 2008 7. Stanbrough M, Bubley GJ, Ross K, et al: Increased expression of genes converting adrenal androgens to testosterone in androgen-independent prostate cancer. Cancer Res 66:2815-2825, 2006 8. Zegarra-Moro OL, Schmidt LJ, Huang H, et al: Disruption of androgen receptor function inhibits proliferation of androgen-refractory prostate cancer cells. Cancer Res 62:1008-1013, 2002 9. Cheng H, Snoek R, Ghaidi F, et al: Short hairpin RNA knockdown of the androgen receptor attenuates ligand-independent activation and delays tumor progression. Cancer Res 66:10613-10620, 2006 10. Oh WK: Secondary hormonal therapies in the treatment of prostate cancer. Urology 60:87-92, 2002; discussion 93 11. Scher HI, Beer TM, Higano CS, et al: Antitumour activity of MDV3100 in castration-resistant AUTHOR’S DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST Although all authors completed the disclosure declaration, the following author(s) indicated a financial or other interest that is relevant to the subject matter under consideration in this article. Certain relationships marked with a “U” are those for which no compensation was received; those relationships marked with a “C” were compensated. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interest policy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section in Information for Contributors. Employment or Leadership Position: None Consultant or Advisory Role: Peter S. Nelson, Janssen Biotech (C), Tokai Pharmaceuticals (C) Stock Ownership: None Honoraria: None Research Funding: None Expert Testimony: None Other Remuneration: None prostate cancer: A phase 1-2 study. Lancet 375: 1437-1446, 2010 12. de Bono JS, Logothetis CJ, Molina A, et al: Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med 364:1995-2005, 2011 13. Geller J, Albert J, Nachtsheim D, et al: Steroid levels in cancer of the prostate: Markers of tumor differentiation and adequacy of anti-androgen therapy. Prog Clin Biol Res 33:103-111, 1979 14. Geller J, Albert J, Vik A: Advantages of total androgen blockade in the treatment of advanced prostate cancer. Semin Oncol 15:53-61, 1988 15. Labrie F, Dupont A, Bélanger A, et al: Combination therapy with flutamide and castration (LHRH agonist or orchiectomy) in advanced prostate cancer: A marked improvement in response and survival. J Steroid Biochem 23:833-841, 1985 16. Caubet JF, Tosteson TD, Dong EW, et al: Maximum androgen blockade in advanced prostate cancer: A meta-analysis of published randomized controlled trials using nonsteroidal antiandrogens. Urology 49:71-78, 1997 17. Chen CD, Welsbie DS, Tran C, et al: Molecular determinants of resistance to antiandrogen therapy. Nat Med 10:33-39, 2004 18. Tran C, Ouk S, Clegg NJ, et al: Development of a second-generation antiandrogen for treatment of advanced prostate cancer. Science 324:787-790, 2009 19. Cai C, Chen S, Ng P, et al: Intratumoral de novo steroid synthesis activates androgen receptor in castration resistant prostate cancer and is upregulated by treatment with CYP17A1 inhibitors. Cancer Res 71:6503-6513, 2011 20. Mohler JL, Gregory CW, Ford OH 3rd, et al: The androgen axis in recurrent prostate cancer. Clin Cancer Res 10:440-448, 2004 21. Mostaghel EA, Nelson PS: Intracrine androgen metabolism in prostate cancer progression: Mechanisms of castration resistance and therapeutic implications. Best Pract Res Clin Endocrinol Metab 22:243-258, 2008 22. Efstathiou E, Titus M, Tsavachidou D, et al: Effects of abiraterone acetate on androgen signaling in castrate-resistant prostate cancer in bone. J Clin Oncol 30:637-643, 2012 23. Feldman BJ, Feldman D: The development of androgen-independent prostate cancer. Nat Rev Cancer 1:34-45, 2001 24. Scher HI, Sawyers CL: Biology of progressive, castration-resistant prostate cancer: Directed therapies targeting the androgen-receptor signaling axis. J Clin Oncol 23:8253-8261, 2005 25. Dehm SM, Schmidt LJ, Heemers HV, et al: Splicing of a novel androgen receptor exon generates a constitutively active androgen receptor that mediates prostate cancer therapy resistance. Cancer Res 68:5469-5477, 2008 26. Hu R, Dunn TA, Wei S, et al: Ligand-independent androgen receptor variants derived from splicing of cryptic exons signify hormone-refractory prostate cancer. Cancer Res 69:16-22, 2009 27. Guo Z, Yang X, Sun F, et al: A novel androgen receptor splice variant is up-regulated during prostate cancer progression and promotes androgen depletion-resistant growth. Cancer Res 69:23052313, 2009 28. Sun S, Sprenger CC, Vessella RL, et al: Castration resistance in human prostate cancer is conferred by a frequently occurring androgen receptor splice variant. J Clin Invest 120:2715-2730, 2010 29. Andersen RJ, Mawji NR, Wang J, et al: Regression of castrate-recurrent prostate cancer by a small-molecule inhibitor of the amino-terminus domain of the androgen receptor. Cancer Cell 17:535546, 2010 30. Palella FJ Jr, Delaney KM, Moorman AC, et al: Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection: HIV Outpatient Study Investigators. N Engl J Med 338:853-860, 1998 31. Wikipedia: Sutton’s Law. http://en.wikipedia. org/wiki/Sutton%27s_law DOI: 10.1200/JCO.2011.39.1300; published online ahead of print at www.jco.org on December 19, 2011 ■ ■ ■ 646 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at Danish National Library Authority on March 26, 2014 from Copyright © 2012 American Society of Clinical Oncology. All rights reserved. 193.163.235.201