Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
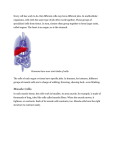
CPD Health Courses! Dry Needling Advanced WELCOME Copyright*CPD*Health*Courses*2014.** Safety in Advanced Dry Needling Practice! Avoidance of Pneumothorax: Lung & Pleural Fields A: Apex of Lung & Plura Mc: Mid Clavicular Ma: Mid Axillary P: Posterior (Spinous Process-Lower Border) L: Lung P: Plura A2.5-4! Mc! Ma! P! L! 6! 8! 10! P! 8! 10! 12! Eg: The Lung is at the level of the 8th rib on the Mid axillary line & the Plura is level with the lower border of the 12th Thoracic vertebrae posteriorly. Copyright*CPD*Health*Courses*2014.** ANTERIOR VIEW 1 2 MSA 3 A P 4 R C N 5 T 6 7 M XP P S 8 9 10 Copyright*CPD*Health*Courses*2014.*** L A! ! 2.5-4! LATERAL VIEW 2 3 4 5 6 7 8 9 10 Copyright*CPD*Health*Courses*2014.*** Mc! Ma! P! L! 6! 8! 10! P! 8! 10! 12! POSTERIOR VIEW T 3 T 7 A! ! 2.5-4! Mc! Ma! P! L! 6! 8! 10! P! 8! 10! 12! T10 T12 Copyright*CPD*Health*Courses*2014.*** Safety in Dry Needling Practice Pneumothorax: Signs & Symptoms! C-C-C-D-D-D-H-S-T-T Copyright*CPD*Health*Courses*2014.** AR13 - Dorsal Scapular (SI-14) Ma’s Acu Reflex Points In a tender depression on the superior border of the medial end of the scapular spine. AR7 - Greater Occipital (BL-10) From the ventral ramus of C5, passing along the medial border of the scapula. Supplies: Levator scapulae, rhomboid major & minor. Enters the Levator scapulae approximately 1 cm superior to the base of the scapulae. In a depression 1.5 cun lateral to the midline at the lateral edge of the trapezius muscle. Symptoms: Periscapular pain, rotator cuff injury & shoulder injuries. The greater occipital nerve is formed from the dorsal rami of the C2 spinal nerve. It emerges between C1 & C2, below the inferior oblique muscle. Supplies the skin of the sub-occipital area & the posterior skull. Needling Instructions: 0.25. Oblique medial insertion at a depth no greater than 25mm. Internal rotation of the arm moves the scapula away from the rib cage. Symptoms: Headache, neck pain, neck stiffness, temporal headache Caution: Deep perpendicular needling carries a substantial risk of injuring the lung. Needling Instructions: 0.22-0.25. Perpendicular insertion 10-20mm depth. AR8 - Suprascapular - Infraspinatus (SI-11) AR3 - Spinal Accessory (GB-21) In a tender depression in the middle of the infra-scapular fossa. At the apex of the shoulder, midway between the midline & the acromion process. The suprascapular nerve innervates the infra & supraspinatus muscles. Receiving fibres from C5 & C6 it enters the middle of the infraspinous fossa. This acureflex point contains both spinal (C1-C6) & cranial nerve (XI) fibres. It also contains efferent (motor) & afferent (sensory) nerve fibres. Symptoms: Periscapular pain, rotator cuff injury & shoulder injuries. Symptoms: Neck pain & headache. Needling Instructions: 0.25. Perpendicular or oblique direction. Needling Instructions: 0.25. Perpendicular insertion while applying a pincer grip to pull the trapezius away from the apex of the lung. Caution: Deep perpendicular needling carries a substantial risk of injuring the lung. AR21- Posterior Cutaneous of T6 (BL-16) Is at the crest of the erector spinae at the level of the lower border of the T6 spinous process. 1.5 cun lateral to the mid-line. From the cutaneous & medial branches of the post primary ramus of the T6 spinal nerve. Symptoms: Interscapular tension, periscapular pain & referred anterior chest pain. Needling Instructions: 0.25. Oblique direction towards the spine. Caution: The apex of the lung lies 2.5-4 cms superior to the clavicle. AR20 - Spinous Process of T7 (DU-9) In a depression just below the spinous process of T7. Level with the inferior angle of the scapula. From the posterior primary ramus of the seventh thoracic spinal nerve. Symptoms: Interscapular tension, periscapular pain & referred anterior chest pain. Needling Instructions: 0.25. Oblique insertion towards the interspinous ligament. Caution: The spinal canal lies 20-35mm deep to the surface of the skin. Caution: Deep perpendicular needling carries aCopyright*CPD*Health*Courses*2014.*** substantial risk of injuring the lung. AR2 - Greater Auricular (TE17) AR18 - Iliotibial (GB-31) Located in a depression behind the earlobe, between the mastoid process & the ramus of the mandible. Located at the point where the tip of the middle finger lies if you were to ask your patient to place their extended arm over the lateral thigh. The point is located just anterior to the mastoid attachment of the sternocleidomastoid muscle. The sciatic nerve may send sensory branches to innervate the iliotibial band. The greater auricular nerve ascends over the sternocleidomastoid over the earlobe angle of the mandible. Symptoms: Lower back pain, lateral thigh pain, ITB soreness & lateral knee pain. It supplies the ares of skin over the inferior part of the ear, the mandible & mastoid process. Needling Instructions: 0.25. Perpendicular & 30-40mm to the bone. Needling should be directed towards the opposite ear at a depth of 10-20 mm in order to avoid the external jugular vein. AR24 - Common Fibular (Peroneal) (GB-34) Symptoms: Headache, neck pain, ear ache & ear pain. In a tender depression 1 cun inferior & 1 cun anterior to the head of the fibula. Needling Instructions: 0.18-.22. Directed towards the other ear to a depth no greater than 10-15mm. The common peroneal nerve, a branch of the sciatic nerve (L4-S3 ventral rami) enters the knee at the popliteal fossa along the medial edge of the biceps femoris muscle. Caution: External Jugular vein AR4 - Saphenous (SP-9) Located on the medial side of the knee at the angle formed by the medial tibial condyle and the posterior shaft of the tibia. It passes superficially over the lateral gastrocnemius, posterior to the head of the fibula & pierces the peroneus longus muscle, where it divides into the superficial & deep fibular nerves. It is called the saphenous because the saphenous nerve emerges exactly at this location. The saphenous nerve is a sensory (cutaneous) branch of the femoral nerve that descends inferiorly from the femoral triangle. The area where it divides into superficial & deep is where this point is located. The skin of the antero-medial surface of the knee & leg up to & including the medial malleolus is supplied by the saphenous nerve. Symptoms: Lower back pain, lateral leg pain, sciatic pain. Symptoms: Needling Instructions: 0.25. Perpendicular insertion & depth of 30-40mm. Symptoms: Medial knee pain, groin pain & medial thigh pain. Copyright*CPD*Health*Courses*2014.** Needling Instructions: 0.25. Perpendicular & depth of 25-30mm Occipitalis & Frontalis Anatomy Origin: Occipitalis - Lateral 2/3 of superior nuchal line, external occipital protuberance. Frontalis – The area of skin that lies superiorly above the eyebrows. Insertion: Galea aponeurosis. This is a thin sheet of connective tissue that connects the Occipitalis & Frontalis muscles. Action: Occipitalis - Assists the Frontalis muscle by anchoring over the occiput & allowing the Frontalis to retract against it. Frontalis – Raises the eyebrows & wrinkles the forehead. Copyright CPD Health Courses 2014. Occipitalis Surface Anatomy Occipitalis is located by first finding the superior nuchal line and sliding upwards towards the vertex of the head. There are two thin oval shaped muscles in this area. Frontalis is found over the forehead and is engaged by asking the patient to wrinkle their forehead. Copyright CPD Health Courses 2014. Occipitalis Caution The posterior auricular nerve (Facial nerve), Maxillary artery & Occipital artery are located in the region of the Occipitalis & Frontalis. Superficial transverse needling is recommended to avoid damaging neurovascular structures. Copyright CPD Health Courses 2014. Occipitalis Needle Selection Quantity: 1-2 per muscle Size: 0.22-0.25 x 30mm Direction: Transverse Oblique/Transverse Depth : 20-25mm Suggested patient position: Supine Copyright CPD Health Courses 2013. Occipitalis Trigger Point The Occipitalis muscle trigger zone is in the centre of the muscle & refers pain over the ipsilateral parietal region and eye. The Frontalis muscle trigger zone lies just above the eyebrow & refers into the ipsilateral supraorbital area. Copyright CPD Health Courses 2014. Temporalis Anatomy Origin: Temporal fossa & fascia above the ear. Insertion: Anteriorly into the ramus of the mandible & the coronoid process below. Action: Elevation & retraction of the mandible. Copyright CPD Health Courses 2014. Temporalis Surface Anatomy Temporalis is located over the side of the head just anterior to the ear. It is easily located and engaged by placing the pads of your fingers over the muscle and asking the patient to clench their teeth. Copyright CPD Health Courses 2014. Temporalis Caution The Facial nerve & Superficial Temporal artery are located in the region of the Temporalis muscle. Superficial transverse needling is recommended to avoid dging neurovascular structures. Copyright CPD Health Courses 2014. Temporalis Needle Selection Quantity: 1-2 Size: 0.22-0.25 x 30mm Direction: Transverse Oblique/Transverse Depth : 20-25mm Suggested patient position: Supine Copyright CPD Health Courses 2013. Temporalis Trigger Point TrZ1, an enthesis type trigger point zone located over the anterior margin of the muscle just superior to the upper border of the zygomatic arch. It refers to the incisors of the ipsilateral upper jaw and eye. TrZ2 & TrZ3 are located immediately & numerically behind TrZ1and are also enthesis type trigger point zones. TrZ3 is the most commonly linked trigger point zone with TMJ pain. TrZ2 & TrZ3 refer upwards over the superior temporalis as well as the ipsilateral maxillary teeth on the upper jaw. TrZ 4 is located at a point just superior to the tip of the ear lobe. It refers postero-obliquely over the muscle and the temporal bone. Copyright CPD Health Courses 2014.