Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
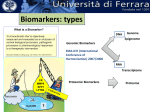
Why do we conduct biological correlative studies for targeted agents? 1. We often have difficulty in determining the optimal dose/schedule in phase 1 to take forward to Phase 2 • Standard cytotoxic drugs lead to predictable effects on proliferating tissues (neutropenia, mucositis, diarrhea), thus enabling dose selection via MTD and confirming MOA- not necessarily true for targeted agents 2. A toxicity-based MTD may not represent the optimal biological dose 3. These agents can be associated with absent or lowlevel tumor regression as single agents- we need to know that we are doing something prior to phase 2/3! A biological correlate can be: 1. Mechanism-based toxicity 2. Biological effects on tumor or surrogate tissue 3. Clinical efficacy Pharmacodynamic (PD) biomarker: Associated with drug exposure- so that’s what most of your protocols contain. Example: Reduction in p-ERK in PBMCs post-MEK inhibitor Predictive biomarker: Predicts outcome to therapy- most useful ones are used before treatment to select patients. Example: KRAS mutation, Her2/Neu, ER/PR Prognostic biomarker: Associated with outcome, independent of therapy- often discovered retrospectively in phase III trials. Example: Ki67 index Biomarkers: Clarifications • Pharmacodynamic (PD) biomarkers can also be predictive • Mechanism-based toxicity is toxicity attributable to MOA and is a type of PD biomarker • Prognostic biomarkers can also be predictive and vice versa, but a classic prognostic biomarker must be assessed in untreated patients • Just because a biomarker is prognostic, does not mean that it will be predictive for an agent that targets that pathway (VEGF is a classic example) How Biomarkers are Used in Early Clinical Development Single-agent activity (in unselected patients) can be limited with targeted agents, thus biomarkers– May be used to effectively screen numerous agents in phase I for biological activity – To prioritize agents going into phase II, and – To enhance activity through patient selection Increasingly the pharmaceutical industry is using biomarkers to make go/no-go decisions Few of them are validated preclinically prior to phase I trials- and this is a problem (and common in Vail protocols!) Biological Correlative Studies: Definitions • Target tissue: tumor! • Surrogate marker, tissue: feasible tumor substitute! • Mechanism-based toxicity: toxicity attributable to MOA (for cytotoxic agent- NTP) • Bioassay, biomarker, correlative assay, biological correlative assay, PD marker- different terms for the same thing Mechanism-Based Toxicity as a Biological Correlate • With drugs that interact with a target on normal tissues, mechanism-based toxicity is a type of biomarker: o skin rash, diarrhea- EGFR agents o hypertension, proteinuria- VEGF agents • Overall, not unlike the myelosuppression and GI effects (mucositis, diarrhea) observed with traditional cytotoxic agents • If a tissue-based biomarker is difficult to obtain, mechanism based toxicity may establish biological activity- and you don’t need to biopsy the patient! Decrease in Ki67 (top) and pERK1/2 (bottom) in skin biopsies following PF299804 (pan-EGFR TKI) treatment. Jänne P A et al. Clin Cancer Res 2011;17:1131-1139 ©2011 by American Association for Cancer Research Skin changes with EGFR-targeted agent So- if you establish that normal tissue (like skin) is a relevant biological target, then the presence of skin rash may substitute for a skin biopsy However, this will primarily indicate drug exposure, but not intended antitumor effects What are Commonly Used Biological Assays? Typical surrogate assays that are feasible: • Plasma or serum-based (usually ELISA) • PBMCs: immunoblotting/ IHC/flow cytometry/ELISAs • Normal skin/ buccal mucosa/hair: IHC • Circulating endothelial cells Tumor-based assays: • IHC/immunoblotting (proteins, phosphorylation, apoptosis) • Microvessel density (has not been useful in patients) • Gene expression (RT-PCR)/mutation/sequencing • Also consider circulating tumor cells Radiological: PET, DCE-MRI, CT, ultrasound How Do You Select an Assay? • First, if the drug has been used before- in humans or animalsobtain information. What has been done previously? Learn from others! • If it’s a brand-new target, search the literature for information about target – where expressed (normal tissue)- and how measured- protein? gene? activation status? cytokine? • Consider a research collaboration with a lab/investigator that is familiar/interested in the target to potentially design the best assay and test it preclinically in in vitro or in vivo models. • Make sure you understand why you are doing the assay- at the end of the study, how will this assay facilitate clinical development? What hypothesis is being tested? Some Considerations When Selecting an Assay 1. Patient acceptance: Is obtaining the sample painful to the patient? Is a separate consent form or check box required. 2. Feasibility: How easy is it to obtain samples? Is the assay one that can be “banked”- or does it have to be run same-day? 3. Cost: This relates to #2 and also dictates frequency of sampling and how much grant funding is required. 4. Who will perform and where will assay be run? Will there be a central site or lab performing it? 5. Reproducibility/ validation/ quality control: Its best to have this done and figured out prior to trial- either using preclinical models or normal volunteer samples. Pros and Cons of Commonly Used Assays Assay Pro Con Plasma/Serum Easy to collect, non-invasive Only reflects what is circulating- does not sample tissue compartment PBMCs Relatively easy to collect, but Often require ex vivo requires special processing “stimulation” to see markerand storage which leads to variability Skin biopsy Can be done in clinic without imaging Invasive and may not express target Tumor biopsy Is the real target Invasive, expensive and often requires imaging Functional Imaging: PET/MRI Non-invasive and may demonstrate changes when tumor size does not change Expensive, should be validated in preclinical models What is the Appropriate Sampling Schedule? o Plasma/blood sampling: Baseline, and potentially at times that correspond to PKs, at steady-state, then periodically after C1 (weekly, monthly). o PBMCs: Require more processing, so usually feasible to obtain at baseline, 1-3 time points around PK samples, at steady-state, then perhaps once a course. o Tumor tissue/skin biopsy: Baseline, and then usually only feasible to obtain once more- either at a “kinetic” time point (peak drug concentration, steady-state) or “efficacy” time point (end of C1 or C2, with imaging). o Imaging: Similar to tumor tissue, but since non-invasive, can perform at “kinetic” and “efficacy” time points. Example: Preclinical-to Clinical Application of Biological Correlative Studies with MEK Inhibitor Figure 2"> Yeh, T. C. et al. Clin Cancer Res 2007;13:1576-1583 Copyright ©2007 American Association for Cancer Research Selumetinib Part B: Percentage change in pERK 19 of 34 paired biopsies (56%) evaluable * * Overall mean inhibition of pERK of 84% compared to predose * 200mg patients Patient 0255 (Melanoma, 100 mg BID) Pre-Dose CT Scan Post - Dose CT Scan Completed 3 Cycles 70% reduction of target lesions – Although non target lesion progression in brain 08-17-2005 01-05- 2006 Tumor – 100 % inhibition of pERK – 97% inhibition of Ki67 pERK Nras mutation Ki-67 Pre-Dose Post-Dose What Did We Learn from the Biological Assays in this Trial? • The preclinical PBMCs and tumor tissue were useful in designing the assays used in the first-in-man phase I trial. • Inhibition of p-ERK in PBMCs is observed at all dose levels and thus, although useful in establishing that the oral drug penetrates into tissue, is less useful for establishing dose-schedule. • Skin rash also occurred at all dose levels, was dose-limiting, and thus was the predominant factor in establishing the MTD. This is thought to be mechanism-based, thus precluding the need skin biopsies. • Tumor tissue reliably demonstrated a reduction in p-ERK which did not correlate to response. • Therefore, the drug is biologically active and can (and has) proceed to phase II/III, but will need other predictive and/or PD biomarkers for selecting patients and/or indicating clinical benefit. Tumor Biopsies: Lessons Learned • Tumor biopsies are feasible to obtain in patients enrolling on phase I trials, but should be restricted to motivated sites with adequate infrastructure. • Post-treatment biopsies can be missed due to clinical deterioration and other problems, so enrollment must always exceed the “n” needed for statistical purposes. • Regardless of the sample size, most assays exhibit substantial inter- and intra-tumor variability. • Avoid the temptation to link outcome with post-treatment changes in phase I- the sample sizes are too small to assess predictive markers. • Suggestion: Validate the assay in preclinical models and then restrict to a more homogenous patient population at/around the recommended phase II dose, in phase I. (“Part B”) What Biological Assays CAN Do • Establish that an agent is pharmacologically active • Determine whether an agent is inducing the expected biological effects • Potentially establish a “threshold” dose or exposure for activity • For more toxic agents, define the “biological index” What Biological Assays CANNOT Do (or have not done to date) • Establish an effective dose independent of toxicity • Rescue an otherwise inactive drug or poor clinical development plan Phase I Trials Questions: • Is biologically active drug circulating in the patient? • Are the preclinical PK/biological studies recapitulated in patients? • What is the dose range of biological activity? Phase I Trials: “Part A”- Dose Escalation Phase Tools: • Pharmacokinetics. • Bioassays (ex vivo assays using patient serum or plasma). • Surrogate tissue assays (PBMCs, buccal mucosa, skin). • ? Tumor tissue biopsies • ? Biological imaging Design: • Multiple dose escalations. • Diverse patient population. • Standard endpoints (MTD, toxicity). Phase I Trials: “Part B”-Cohort Expansion Phase Questions: • Does the drug interact with the target (tumor) in the expected manner? • Is there a dose-response relationship to the effects? (if Part B has 1-3 dose levels) • What is the dose that yields adequate drug exposure, relevant biological effects, and is well tolerated? Phase I Trials: “Part B”- Dose Expansion Phase Tools: • Assays on tumor tissue using the relevant biological endpoints. • Biological imaging. • Pharmacokinetics to assess PK/PD relationships. Design: • More focused patient population- maybe even with 1-2 disease-specific arms. • 1-3 dose levels. • Tumor tissue available for assessment. Part B may also be useful for assessing feasibility of predictive biomarkers Recommended Algorithm “Part A” Dose Seeking Phase I (Toxicity or PK endpoint) Identify a dose range: Recommend Highest Tolerable Dose Biomarkers Optional: Best performed on PBMCs/plasma “Part B” Define Active Dose Range Expanded Phase I Cohort (preferable) or Separate Trial Patients/ level, Uniform Population (1+ strata) Final Dose or Active Dose Range Defined Phase II Trials Questions: • Does the drug reproducibly interact with the target in the expected manner? • Is there a relationship between the (baseline or posttreatment) biological marker and clinical outcome? Phase II Trials Tools: • Tumor biopsy- if feasible, or baseline tissue (predictive biomarkers). • Surrogate tissue assays. • Biological imaging. Design: • Single patient population. • Fixed dose level (unless randomized phase II warranted to explore 2 dose levels). • Relevant clinical endpoints that include disease stability. NCI CTEP Biomarker Guidelines • CTEP has developed a new Biomarker Review Committee (BRC) that will review all biomarker components of CTEPsponsored clinical trials • All LOIs will require BRC approval if they have any of the following: • Integral and/or integrated biomarkers (definition coming up) • Biomarker assays requesting NCI funding • Biomarkers that request NCI funding for sample acquisition Exploratory biomarkers not requesting NCI funding do not require BRC approval NCI CTEP Biomarker Guidelines • Integral biomarkers: essential for conducting the study as they define eligibility, stratification, disease monitoring or study endpoints • Integrated biomarkers: testing a hypothesis based on preexisting data and not simply generating hypotheses • Ideally performed on all patients in a trial/assay already tested in the disease in question with reproducible analytic qualities. • Exploratory biomarkers: May not be performed in all patients on the trial and collection may be voluntary Website: http://www.cancer.gov/aboutnci/organization/ccct/funding/BIQSFP/2013Updated-BIQSFP-Announcement What We Have Not Covered • Preclinical development of predictive and pharmacodynamic biomarkers • Details on functional imaging- preclinical and clinical • All of the useful ways to integrate biomarkers into biopsy-driven or disease-specific expanded cohorts • The increasing use and incorporation of nextgeneration sequencing into early phase trials (usually for prediction of patient outcome) • Biomarkers of resistance- increasingly important