Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Drug-eluting stent wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Aortic stenosis wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Antihypertensive drug wikipedia , lookup
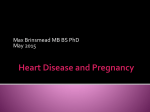
AJH 2002; 15:405– 409 Reflection in the Arterial System and the Risk of Coronary Heart Disease Tomoshige Hayashi, Yasunori Nakayama, Kei Tsumura, Kiyomichi Yoshimaru, and Hiroyasu Ueda Background: Although it was reported that the augmentation index and inflection time are closely related to reflection in the arterial system and large artery function, it is not known whether these indices of the ascending aortic pressure waveform increase the risk of coronary heart disease (CHD). The purpose of this study was to evaluate whether the aortic reflection of the ascending aortic pressure waveform is related to an increased risk of CHD. Methods: We enrolled 190 men and women who had chest pain, normal contractions, no local asynergy, and no history of myocardial infarction. We measured the ascending aortic pressure using a fluid-filled system. The inflection time was defined as the time interval from initiation of a systolic pressure waveform to the inflection point. We investigated the association between the inflection time and augmentation index of the ascending aorta and the risk of CHD. A Results: Both the inflection time and augmentation index were associated with an increased risk of CHD. The crude prevalence rates of CHD were 66.0% for the shortest quartile and 10.6% for the longest quartile of the inflection time, and 17.0% for the lowest quartile and 40.4% for the highest quartile of the augmentation index. The multipleadjusted odds ratio of CHD was 30.8 (95% confidence interval [CI] 7.43–128.05) for the shortest quartile of the inflection time compared with the longest quartile and was 3.82 (95% CI 1.26 –11.59) for the highest quartile of the augmentation index compared with the lowest quartile. Conclusions: The augmentation index and inflection time were associated with an increased risk of CHD. Am J Hypertens 2002;15:405– 409 © 2002 American Journal of Hypertension, Ltd. Key Words: Risk factors, inflection time, coronary disease, stenosis, aorta. lthough previous clinical studies on risk factors have greatly contributed to the understanding and prevention of coronary heart disease (CHD),1– 8 some risk factors remain a challenge. The major risks studied extensively include smoking, hypertension, high serum cholesterol, low levels of high-density lipoprotein cholesterol, type 2 diabetes, and aging.1–5 Although high systolic hypertension, high diastolic hypertension, and high pulse pressure are potent risk factors,6 – 8 the effects of the reflection of the ascending aortic pressure waveform on the occurrence of CHD have not been reported. The fact that the analysis of reflection waveform is detected by high fidelity measurements of arterial pressure waveform makes it impractical in clinical settings. Therefore, we measured inflection point using a fluid-filled recording system and examined whether the inflection time is correctly defined.9 To quantify the artery reflection, we used the augmentation index and inflection time.9 The augmentation index and inflection time using a fluid-filled recording system were reliable and unchanged by repeated measurements. Previous investigators demonstrated that the ascending aortic pressure waveform was divided by the augmentation index and that both inflection time and augmentation index were related to the impedance spectral pattern.8 –11 Thus, the impedance spectra represent larger reflections as the augmentation index becomes larger. In contrast, the impedance spectra reveal smaller and more diffuse reflections as the augmentation index gets smaller. Both the inflection time and augmentation index are closely related to reflection in the arterial system and large artery function. These indices are promising tools for understanding the arterial system using a fluid-filled recording system. We hypothesized that the inflection time and large artery Received January 2, 2002. First Decision January 8, 2002. Accepted January 8, 2002. ment of Internal Medicine (HU), Osaka City University Medical School, Osaka, Japan. Address correspondence and reprint requests to Dr. Yasunori Nakayama, Department of Cardiology, Ishikiriseiki Hospital, 18-28, Yayoi, Higashiosaka-City, Osaka, 579-8026, Japan; e-mail: ahiru-nakayama@ par.odn.ne.jp From the Department of Cardiology, Ishikiriseiki Hospital (TH, YN, KY) and Department of Preventive Medicine and Environmental Health (TH), Second Department of Internal Medicine (KT), and First Depart© 2002 by the American Journal of Hypertension, Ltd. Published by Elsevier Science Inc. 0895-7061/02/$22.00 PII S0895-7061(02)02260-4 406 REFLECTION AND CORONARY HEART DISEASE function would be associated with coronary artery conditions. Therefore, we investigated the effects of large artery function, using the inflection time and augmentation index, in relation to the risk of CHD. Methods Study Subjects The study group consisted of 190 consecutive patients who were admitted to Ishikiriseiki Hospital, Osaka, Japan, because of a CHD diagnosis using cardiac catheterization. They were eligible for entry into the study if they had normal contractions, no local asynergy shown by left ventriculography, and no history of myocardial infarction to approximately fix cardiac function. We enrolled 1021 men ranging in age from 35 to 78 years between January 1990 and March 1999 in whom cardiac catheterizations were done for the first time. Of these, 831 were excluded from this study because of acute myocardial infarction, the presence of local asynergy shown by left ventriculography, chronic renal failure, severe valvular disease, post cardiac surgery, cardiomyopathy, arterial fibrillation, pacemaker implantation, sick sinus syndrome, or aortic dissection. The protocol was in accordance with the Institutional Guidelines for Human Research, and each individual provided a written statement of informed consent to the diagnostic and therapeutic procedures required for examination, which stated that the results of the examination could be used for the study. Measurement of Hemodynamic Variables Hemodynamic measurements were made with the patient in the supine position. Aortic pressure was measured using a fluid-filled system (5F pigtail catheter) at the ascending aorta. A hard copy was made of the pressure tracing using a chart recorder (Nihon Koden, Surgical Monitoring System, Tokyo, Japan) at a paper speed of 100 mm/sec. We compared tracings of systolic, diastolic, mean, and pulse pressures in patients with and without CHD. Ascending aortic pressure at the inflection point dividing into an early and late systolic phase was used as inflection pressure.8 –11 We used the inflection time as the time interval between onset of a systolic pressure waveform and the inflection point.8 –11 To examine whether inflection time measured by a fluid-filled recording system is correctly defined and truly reliable, we compared the values of inflection time measured by interobserver with those by intraobserver. There was a closely linear correlation between the inter- and intraobserver in this study population (Yinter ⫽ 0.96Xintra ⫹ 1.4, R ⫽ 0.93). The inflection time defined by a fluidfilled recording system was reliable and unchanged by repeated measurements. Measurement of Angiographic Variables Cardiac catheterization was performed according to a standard technique. Optimal views of the target lesions from AJH–May 2002–VOL. 15, NO. 5 all technically suitable angiograms were analyzed, and measurements were made of the maximal narrowing of the target lesion, as well as a noninvolved segment. Angiographic measurements were calibrated using a guiding catheter as the reference dimension. The absolute values for the minimal lumen diameter (MLD) and the reference lumen diameter were measured at end-diastole. Coronary heart disease was defined as MLD stenosis ⬎50% on the angiogram, and non-CHD was defined as MLD stenosis ⱕ50% on the angiogram. Statistical Analysis Values were expressed as mean ⫾ one standard deviation. Categoric variables were compared using the 2 test. Differences in the mean values between the two groups were compared using an unpaired t test. A P value of ⬍ .05 was considered significant. Multiple logistic regression analysis was used to evaluate the simultaneous effects of the augmentation index or inflection time, age, body mass index, smoking habits (current smokers or nonsmokers), hypertension (yes or no), type 2 diabetes (yes or no), hypercholesterolemia (yes or no), calcium channel blockers (yes or no), -blockers (yes or no), angiotensin converting enzyme (ACE) inhibitors (yes or no), nitrates (yes or no), parental history of CHD, and sex. The linear trends in the risks were evaluated by entering indicators for each categoric level of exposure using the median value for each category. We calculated the 95% confidence interval (CI) for each odds ratio (OR) and all P values were two tailed. Statistical analyses were performed using the SPSS 10.0 software package (SPSS Inc., Chicago, IL). Results Baseline Clinical Characteristics The baseline clinical characteristics of the study group are summarized in Table 1. Although the mean level of body mass index; the distribution of sex; the presence of parental history of CHD, hypertension, type 2 diabetes, or hypercholesterolemia; and the smoking status were similar in the two groups, the mean age was higher in patients with CHD than those without CHD. There were no significant differences in heart rate or ejection fraction between the two groups. Although systolic, diastolic, and mean pressures in the ascending aorta were not different between the two groups, the pulse pressure was higher in patients with CHD than those without CHD (66.5 ⫾ 21.3 and 73.6 ⫾ 19.7 mm Hg, respectively; P ⫽ .029). The augmentation index was significantly higher in patients with CHD than in those without CHD (0.22 ⫾ 0.16 and 0.30 ⫾ 0.14, respectively; P ⫽ .001), and the inflection time was significantly longer in patients with CHD than in those without CHD (110.3 ⫾ 21.1 and 90.5 ⫾ 22.5, respectively; P ⬍ .001). Illustrated in Fig. 1 are the waveforms of ascending aortic pressure in the cases of patient without CHD (left panel) and patient with CHD (right panel). Although heart AJH–May 2002–VOL. 15, NO. 5 REFLECTION AND CORONARY HEART DISEASE 407 Table 1. Baseline characteristics of study patients (n ⫽ 190) Variables Male sex (n) Age (y) Body mass index (kg/m2) Hypertension Type 2 diabetes Hypercholesterolemia Current smoker Parental history of CHD Heart rate (beats/min) Ejection fraction (%) Ascending aorta Systolic pressure (mm Hg) Diastolic pressure (mm Hg) Mean pressure (mm Hg) Pulse pressure (mm Hg) Augmentation index Inflection time (mm sec) CHD (ⴚ) 78 57.8 23.5 47 34 61 63 20.0 68.8 75.5 139.7 73.2 100.2 66.5 0.22 110.3 CHD (ⴙ) (60.9) ⫾ 11.4 ⫾ 3.3 (36.7) (26.6) (47.7) (49.2) (15.6) ⫾ 13.3 ⫾ 6.8 43 62.1 23.9 62 23 32 31 15.0 66.3 75.8 24.7 9.5 12.9 21.3 0.16 21.1 144.6 71.1 101.5 73.6 0.30 90.5 ⫾ ⫾ ⫾ ⫾ ⫾ ⫾ P (69.4) ⫾ 9.8 ⫾ 3.5 (48.4) (37.1) (51.6) (50.0) (24.2) ⫾ 11.7 ⫾ 7.2 .258 .012 .387 .125 .137 .609 .920 .153 .230 .812 22.2 10.7 13.3 19.7 0.14 22.5 .183 .162 .517 .029 .001 ⬍.001 ⫾ ⫾ ⫾ ⫾ ⫾ ⫾ CHD ⫽ coronary heart disease. Values are mean ⫾ SD or No. (%) of patients. rates are similar in the two cases, the inflection point is much earlier in patients with CHD than in patients without CHD. As a result, inflection time is shorter in patients with CHD than in patients without CHD. The Augmentation Index and the Risk of CHD To examine the association between the augmentation index and the risk of CHD, all patients were classified into quartiles of the augmentation index level. The augmenta- tion index was associated with an increase in the risk of CHD (Table 2). The crude prevalence rates of CHD were 17.0% for quartile 1, 25.0% for quartile 2, 47.9% for quartile 3, and 40.4% for quartile 4 of augmentation index levels. After adjustment for age, body mass index, smoking habits, hypertension, hypercholesterolemia, type 2 diabetes, calcium channel blockers, -blockers, ACE inhibitors, nitrates, parental history of CHD, and sex, the OR of CHD was 1.00 (reference) for quartile 1, 1.85 (95% CI 0.63–5.45) for quartile 2, 4.63 (95% CI 1.57–13.7) for FIG. 1. Left) Without coronary heart disease; (right) with coronary heart disease. Schematic representation of augmentation index and inflection time of ascending aortic artery in a representative case. Augmentation index is the ratio of inflection pressure to pulse pressure. The inflection time was defined as the time interval between onset of a systolic pressure waveform and the inflection point. 408 REFLECTION AND CORONARY HEART DISEASE AJH–May 2002–VOL. 15, NO. 5 Table 2. Odds ratio of coronary heart disease according to the augmentation index and inflection time Augmentation index Quartile 1 (⫺0.14–0.14) Quartile 2 (0.15–0.26) Quartile 3 (0.27–0.36) Quartile 4 (0.37–0.74) Wald, 2 P for trend Continuous, per 0.1 Wald, 2 Inflection time (mm sec) Quartile 1 (56–85) Quartile 2 (86–102) Quartile 3 (103–123) Quartile 4 (124–208) Wald, 2 P for trend Continuous, per 10 mm sec decreased Wald, 2 Crude OR (95% CI) Multiple-Adjusted* OR (95% CI) 17.0 25.0 47.9 40.4 1.00 1.63 (0.60–4.43) 4.48 (1.74–11.58) 3.31 (1.27–8.62) 12.2 .002 1.40 (1.13–1.72) 9.7 1.00 1.85 (0.63–5.45) 4.63 (1.57–13.7) 3.82 (1.26–11.59) 9.4 .007 1.38 (1.08–1.76) 6.6 66.0 42.6 12.2 10.6 16.2 (5.38–49.20) 6.22 (2.08–18.56) 1.17 (0.33–4.14) 1.00 37.9 ⬍.001 30.8 (7.43–128.05) 6.77 (2.01–22.74) 1.04 (0.27–3.98) 1.00 34.1 ⬍.001 1.59 (1.33–1.90) 26.5 1.71 (1.38–2.13) 23.2 n Cases (%) 47 48 48 47 8 12 23 19 47 47 49 47 31 20 6 5 OR ⫽ odds ratio; CI ⫽ confidence interval. * Adjusted for age, body mass index, smoking habits, hypertension, type 2 diabetes, hypercholesterolemia, parental history of coronary heart disease, calcium channel blockers (yes or no), -blockers (yes or no), angiotensin converting enzyme inhibitors (yes or no), nitrates (yes or no), and sex. quartile 3, and 3.82 (95% CI 1.26 –11.59) for quartile 4 of the augmentation index level (Wald 2 ⫽ 9.4, P for trend ⫽ .007). To further quantify the effect of the augmentation index on CHD, we modeled the augmentation index as a continuous variable. The multiple-adjusted OR of CHD was increased by 38% when the augmentation index was increased by 0.1 (OR 1.38; 95% CI 1.08 –1.76, Wald 2 ⫽ 6.6). for age, body mass index, smoking habits, hypertension, type 2 diabetes, hypercholesterolemia, calcium channel blockers, -blockers, ACE inhibitors, nitrates, parental history of CHD, and sex, the association was significant. The inflection time had a stronger association with the risk of CHD than the augmentation index. The Inflection Time and the Risk of CHD Index to Quantify Large Artery Function To examine the association between the inflection time and the risk of CHD, all patients were classified into quartiles of inflection time. The analysis of inflection time in ascending aorta is summarized in Table 2. The inflection time as it decreased was also associated with an increase in the risk of CHD. The crude prevalence rates of CHD were 66.0% for quartile 1, 42.6% for quartile 2, 12.2% for quartile 3, and 10.6% for quartile 4 of inflection time. The multiple-adjusted OR of CHD was 30.8 (95% CI 7.43–128.05) for quartile 1, 6.77 (95% CI 2.01–22.74) for quartile 2, 1.04 (95% CI 0.27–3.98) for quartile 3, and 1.00 (reference) for quartile 4 of inflection time (Wald 2 ⫽ 34.1, P for trend ⬍ .001). When we modeled the inflection time as a continuous variable, the multipleadjusted OR of CHD was increased by 71% when the inflection time was decreased by 10 mm sec (OR 1.71; 95% CI 1.38 –2.13, Wald 2 ⫽ 23.2). Because arteriosclerosis decreases the compliance of the aortic artery and increases the characteristic impedance, it causes the aortic arterial input impedance to be relatively high. Although ascending aortic input impedance most clearly demonstrates manifest arteriosclerosis,12,13 the fact that the estimation of impedance necessitates high fidelity measurements of instantaneous ascending aortic flow and pressure makes it impractical in clinical settings. Instead of measuring ascending aortic input impedance, we focused on more simple variables pertaining to the dynamic mechanical properties of the arterial system. The augmentation index and inflection time are closely related to reflection in the arterial system and large artery function. These indices are simple to measure and make attractive tools to understand the arterial system. We hypothesized that reflection in the arterial system and large artery function would be related to coronary artery conditions. Therefore, we investigated the effects of reflection in the arterial system and large artery function in relation to the risk of CHD. Our results revealed that these indices were associated with an increased risk of CHD. Discussion The inflection time and augmentation index were associated with an increased risk of CHD. Even after adjustment AJH–May 2002–VOL. 15, NO. 5 Clinical Implications Regarding the Augmentation Index and Inflection Time Although major risks include smoking, hypertension, high serum cholesterol, low levels of high-density lipoprotein cholesterol, diabetes mellitus, and aging,1–5 other risk factors for CHD remain a challenge in clinical settings. The augmentation index and inflection time of the ascending aortic pressure waveform can reveal the large artery function. Because large artery function is composed of compliance, characteristic impedance, and resistance, the inflection time and augmentation index of the ascending aortic pressure waveform would enable us to choose the best drugs for patients with hypertension and angina pectoris. This study contributes not only to the understanding and prevention of CHD, but also to the understanding of the arterial system. REFLECTION AND CORONARY HEART DISEASE 5. 6. 7. 8. 9. 10. References 11. 1. 2. 3. 4. Doyle JT: Cigarette smoking and coronary heart disease: combined experience of the Albany and Framingham studies. N Engl J Med 1988;266:796 –801. Kannel WB: Smoking and hypertension as predictors of cardiovascular risk in population study. J Hypertens 1990;8:53–58. Shah PK, Pasternak R: The role of lipids in restenosis following angioplasty. Curr Opin Lipidemiol 1993;4:310 –313. Gordon DJ, Probstfield JL, Garrison RJ, Neaton JD, Castelli WP, Knoke JD, Jacobs DR Jr, Bangdiwala S, Tyroler HA: High-density 12. 13. 409 lipoprotein cholesterol and cardiovascular disease: four prospective American studies. Circulation 1989;79:8 –15. Kannel WB: Diabetes and cardiovascular risk factors: the Framingham study. Circulation 1979;59:8 –13. Benetos A, Safar M, Rudnichi A, Smulyan H, Richard JL, Ducimetieere P, Guize L: Pulse pressure: a predictor of long-term cardiovascular mortality in a French male population. Hypertension 1997;30:1410 –1415. Mitchell GF, Moye LA, Braunwald E, Rouleau JL, Bernstein V, Geltman EM, Flaker GC, Pfeffer MA: Sphygmomanometrically determined pulse pressure is a powerful independent predictor of recurrent events after myocardial infarction in patients with impaired left ventricular function. Circulation 1997;96:4254 –4260. Kelly RP, Hayward CS, Avolio AP, O’Rourke MF: Non-invasive determination of age-related changes in the human arterial pulse. Circulation 1989;80:1652–1659. Nakayama Y, Nakanishi N, Hayashi T, Nagaya N, Sakamaki F, Satoh N, Ohya H, Kyotani S: Pulmonary artery reflection for differentially diagnosing primary pulmonary hypertension and chronic pulmonary thromboembolism. J Am Coll Cardiol 2001;38:214 – 218. Murgo JP, Westerhof N, Giolma JP, Altobelli SA: Aortic input impedance in normal man: relationship to pressure wave forms. Circulation 1980;62:105–116. Murgo JP, Westerhof N, Giolma JP, Altobelli SA: Effects of exercise on aortic input impedance and pressure wave forms in normal humans. Circ Res 1981;48:334 –343. Sunagawa K, Maughan WL, Sagawa K: Stroke volume effect of changing arterial input impedance over selected frequency ranges. Am J Physiol 1985;248:H477–H486. Nakayama Y, Tsumura K, Yamashita N, Yoshimaru K, Hayashi T: Pulsatility of ascending aortic pressure waveform is a powerful predictor of restenosis after percutaneous transluminal coronary angioplasty. Circulation 2000;101:470 –472.